

Vascular Closure Devices Attenuate Femoral Access Complications of Primary Percutaneous Coronary Intervention





Abstract: Objectives. To compare severe complications related to radial access and those related to femoral access using vascular closure devices for patients undergoing primary percutaneous coronary intervention (PCI). Background. Femoral artery access is still used for acute myocardial infarction management; studies comparing state-of-the-art radial and femoral techniques are required to minimize bias regarding the outcomes associated with operator preferences. Methods. We performed a randomized study comparing radial access with a compression device and anatomic landmark-guided femoral access with a hemostatic vascular closure device. The severe complication rates related to the access site were assessed until hospital discharge. A meta-analysis including studies with comparable populations reporting severe bleeding and major adverse cardiovascular event rates was performed. Results. A total of 250 patients were included who underwent PCI between January 2016 and February 2019. Mean age was 61.5 ± 12.2 years, 73.2% were men, and 28.4% had diabetes. There were no differences between groups or in vascular access-related severe complication rates (8.0% for femoral group vs 5.6% for radial group; P=.45). Although radial access was associated with decreased vascular complications related to the access site when compared with the femoral approach (relative risk [RR], 0.64; 95% confidence interval [CI], 0.43-0.95), the meta-analysis did not show an impact on severe bleeding (RR, 0.74; 95% CI, 0.37-1.46) or severe cardiovascular adverse events (RR, 0.69; 95% CI, 0.30-1.58). Conclusions. Compliance with femoral artery puncture techniques and routine use of a vascular closure device promoted low severe complication rates.
Key words: complications, femoral artery, myocardial infarction, radial artery, vascular closure device
Radial access is the preferred strategy for invasive coronary procedures, particularly for acute coronary syndromes, and is suggested by current guidelines.1,2 The benefits associated with radial access when compared with femoral access are lower morbidity and mortality rates, fewer vascular complications, and less-severe bleeding events.3 Although use of the radial approach has increased in the past 10 years, considerable geographical variability, institutional variability, and operator variability exist, particularly in the United States.4 Data from the National Cardiovascular Data Registry CathPCI have shown an increase, from 2% to 23%, in transradial primary percutaneous coronary intervention (PCI) between 2009 and 2015.5
Nevertheless, clinical trials that have shown more net clinical benefits of radial access compared with femoral access often do not analyze the preferred approach of the operator or the routine use of vascular closure devices (VCDs).6 Femoral access may be required in routine situations, such as upper-limb complex anatomic arterial variants, advanced age, and female sex, which are well-known predictive factors for radial access failure.7 Comparisons of femoral access complication rates reported in historical cohorts and current rates have suggested an increase in their prevalence, mainly when procedures are performed by operators considered “radialists.”8,9 A recent analysis of the randomized HEAT-PPCI study (How Effective are Antithrombotic Therapies in Primary Percutaneous Coronary Intervention) indicated that radial access was associated with lower rates of cardiac adverse events and severe bleeding. However, when events were analyzed based on the operators’ preferred access sites (used for >90% of their personal cases), outcomes were similar and femoral complications were increased among operators who preferred the radial approach.10 Therefore, additional studies capable of minimizing the bias caused by operators’ vascular access preferences are required to promote comparable outcomes of both state-of-the-art techniques.11 The present randomized study compared radial access with femoral access using VCD for patients who were diagnosed with ST-segment elevation myocardial infarction (STEMI) and underwent primary PCI to assess the occurrence of severe complications at the vascular access site.
Methods
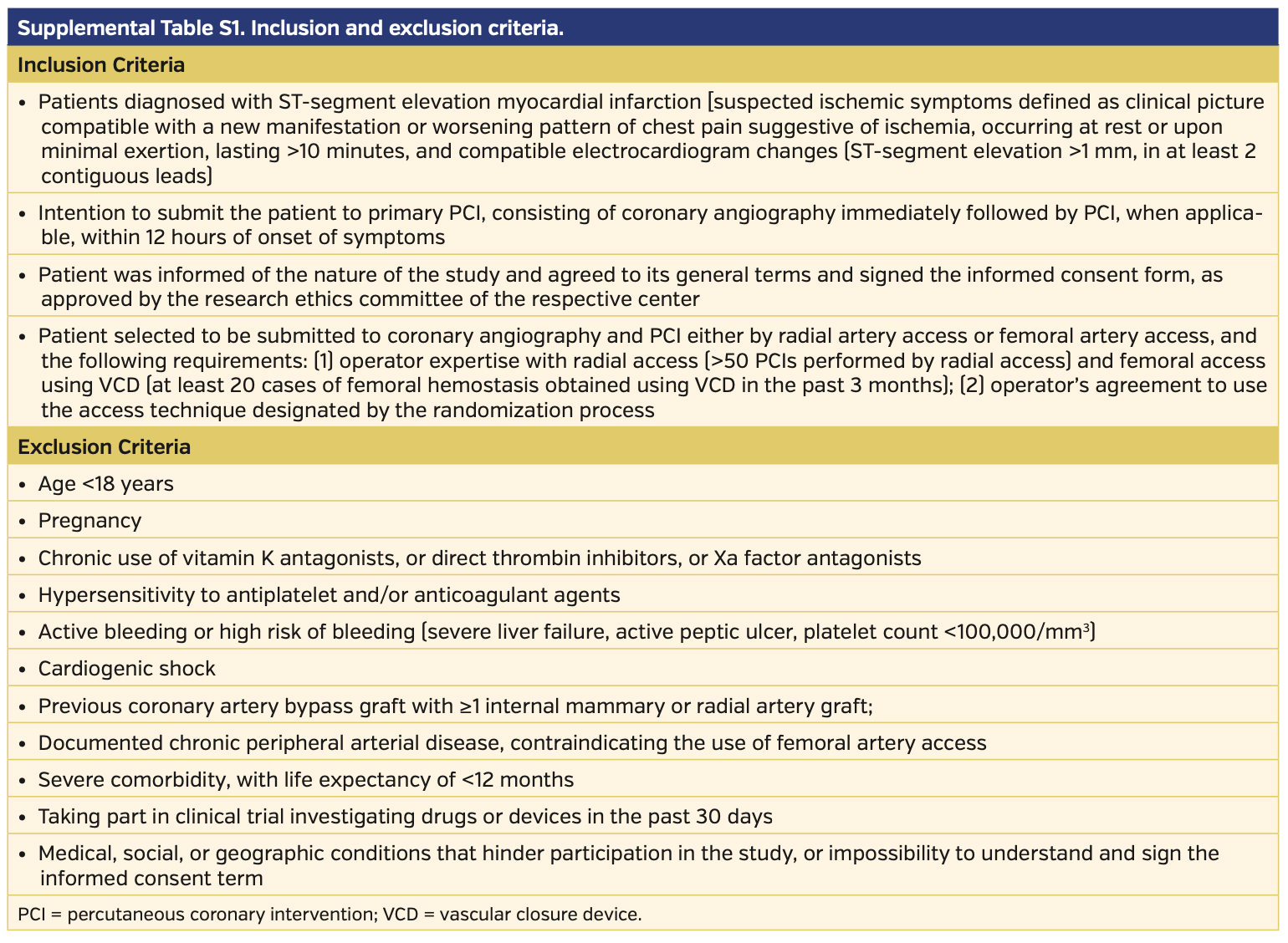
Study population. This randomized, multicenter study compared radial access with femoral access using VCD for patients diagnosed with STEMI and admitted for primary PCI within 12 hours of symptom onset. Cases were included if the conditions could be feasibly treated with both radial access or femoral access and if operators who performed the procedure were proficient in radial access (>250 PCI procedures performed via radial access) and femoral access using VCD (at least 50 femoral hemostasis procedures performed using VCD in the past 12 months). Detailed inclusion and exclusion criteria and study definitions are described Supplemental Tables S1 and S2 (available at www.invasivecardiology.com). For randomization, we used a random sequence obtained by computational algorithms and kept the results in individual, non-translucent, sealed envelopes to ensure the blinded allocation process. The study was approved by our local ethics committee and written informed consent was obtained from each patient. No extramural funding was used to support this work. The clinical trial was registered at www.clinicaltrials.gov (NCT02831166).
Objectives. The primary objectives were to compare radial access associated with a selective compression band and femoral access using VCD for patients who underwent primary PCI and to assess the occurrence of severe complications at the site of arterial puncture until hospital discharge. Outcomes of interest included type 3 or type 5 severe bleeding according to the Bleeding Academic Research Consortium definition,12 retroperitoneal hemorrhage, pseudoaneurysm, arteriovenous fistula, hematoma >5 cm, limb ischemia, or vascular repair surgery. The secondary objective was to compare the procedural success rate, device success rate, requirement for access-site crossover, and the in-hospital prevalence of cardiovascular deaths, acute myocardial infarction (MI), and stroke.
Study procedures. Radial access was obtained using a 6 Fr, 10 cm hydrophilic introducer; puncture was performed 1 cm proximal to the radial styloid process either by using a needle or by transfixing with a Jelco catheter (Smiths Medical). The TR Band radial compression device (Terumo Corporation) was used for hemostasis performed with the patent hemostasis technique according to a previously validated protocol.13 Femoral access was obtained by puncturing the anterior wall of the common femoral artery, which was confirmed by angiography, and being guided by an anatomic landmark (medial third of the femoral head) using a 6 Fr introducer. Ultrasound-guided and micropuncture techniques were not used. Hemostasis was obtained using the AngioSeal (Terumo Corporation), Perclose Proglide (Abbott Vascular), or StarClose device (Abbott Vascular) according to the technique described by the device manufacturer.
Dual-antiplatelet therapy consisted of aspirin associated with a thienopyridine class drug or a direct adenosine diphosphate platelet receptor antagonist. Anticoagulation was obtained by intravenous administration of 100 U/kg of unfractionated heparin. After successful PCI procedures, anticoagulant therapy was discontinued and prophylaxis for venous thromboembolism was maintained with fondaparinux. Some medications, such as angiotensin-converting enzyme inhibitors or angiotensin-receptor blockers, beta-blockers, statins, and aldosterone antagonists, were prescribed as recommended by the current guidelines for secondary heart disease prevention.
Myocardial necrosis markers were measured at the time of hospital admission and between 12 and 24 hours post procedure. An electrocardiogram was recorded soon after the procedure and then daily until hospital discharge, or when a new ischemic event was suspected. Hemoglobin and hematocrit levels were measured at the time of admission and then routinely (every 12 and 24 hours) post procedure. Complications related to the arterial vascular access site, as well as severe bleeding, cardiovascular death, MI, and stroke, were evaluated and verified by two cardiologists who did not participate in the procedures, at hospital discharge. Vascular access imaging was performed only when any complication was observed during physical examination of the patient.
Statistical analysis. This pilot study aimed to assess the safety and efficacy of femoral access using VCD compared with the radial approach for 250 patients presenting with STEMI and scheduled to undergo primary PCI. Safety and efficacy were based on the reduction in complications at the site of arterial puncture during hospital admission for all randomized patients. The allocation ratio of each group was 1:1. The study did not follow the criteria for sampling calculations or predicted outcomes. Quantitative variables were expressed as means ± standard deviations or medians (25th percentile-75th percentile) according to the distribution of each variable. The Student’s t-test or Mann-Whitney test was used for variables with normal distribution whenever required. Qualitative variables were summarized as absolute frequencies and percentages. For comparisons, Fisher’s Exact test, Chi-square test, or maximum likelihood Chi-square test was used as required. Variables with a potential influence on the primary outcome were included in a logistic regression model. After univariate analysis, variables with a significant P-value (P<.10) were selected to be evaluated by the multivariate logistic regression model. Results were described as relative risk (RR) and 95% confidence interval (CI) and were considered significant when the descriptive level (P-value) was <.05. A statistical analysis was performed using SAS for Windows software, version 9.2 (SAS Institute).
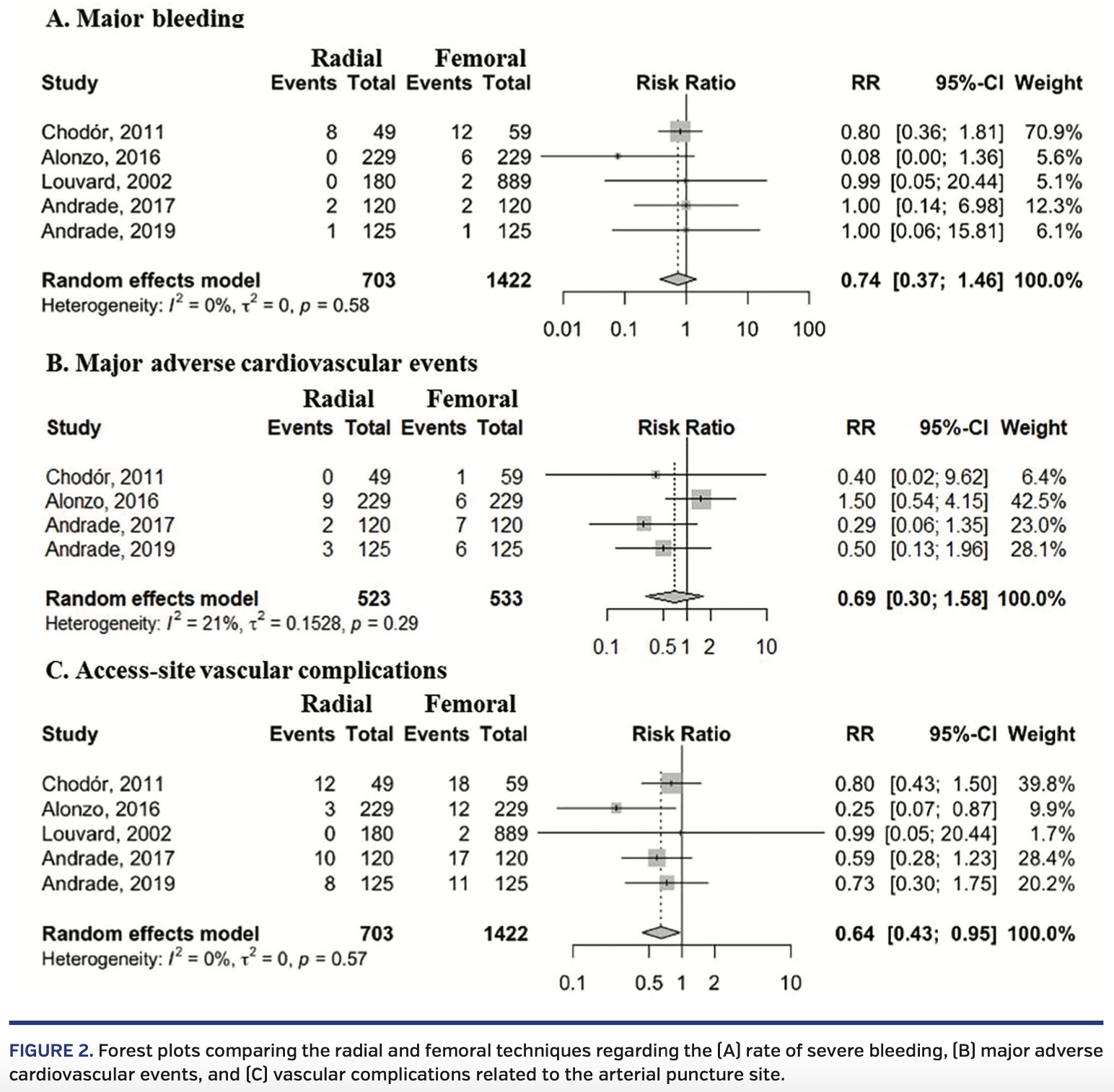
We performed a meta-analysis including the findings of the present study and those of studies that compared radial access with femoral access and the routine use of VCD for patients undergoing PCI due to MI who met the inclusion criteria for analysis; outcomes assessed were severe bleeding and major adverse cardiovascular events, including death, MI, or stroke. We searched PubMed and ISI of Science from January 2001 to June 2019. The random-effects model was used to account for the heterogeneity of the studies.
Results
Study participants from five Brazilian institutions were included from January 2016 to February 2019. Figure 1 describes the inclusion and randomization flow chart. Of 287 participants selected for triage, a total of 250 (87.1%) were randomized and assessed during hospital admission, enabling the analysis of the primary objective of the study.
Table 1 shows comparisons between groups regarding demographic and baseline clinical characteristics. The mean age was 61.5 ± 12.2 years. Participants were predominantly male (73.2%) and had a high prevalence of risk factors, such as diabetes mellitus (28.4%), arterial hypertension (64.8%), dyslipidemia (40.0%), and smoking (32.0%); there were no statistically significant differences between groups. Primary PCI was performed for all patients, except 1 patient in the femoral group. There were no differences between groups regarding the time of ischemia, MI site, duration and characteristics of the procedures, ST-segment elevation resolution rates, and adjuvant antithrombotic therapy (Table 2). Among the VCDs, AngioSeal was used most often (65.6%), followed by StarClose (21.6%) and Perclose Proglide (12.8%).
Table 3 shows the primary and secondary outcomes. No differences were found regarding the rates of severe complication related to vascular access (8.0% in the femoral group vs 5.6% in the radial group; P=.45). There were no cases of retroperitoneal hematoma, pseudoaneurysm, arteriovenous fistula, or compartment syndrome, and none required vascular repair surgery. Success rates of the procedures and hemostasis devices were high; the need for access-site crossover was <2%. The 3 cases of postprocedure MI were due to subacute stent thrombosis. Table 4 shows the logistic regression analysis results. The independent variables for the primary outcome were chronic renal failure (RR, 0.381; 95% CI, 0.14-1.05), age (RR, 1.076; 95% CI, 1.03-1.13), and total ischemic time (RR, 1.002; 95% CI, 0.99-1.05). In the multivariate analysis, only age influenced the occurrence of outcomes (RR, 1.077; 95% CI, 1.02-1.14). No statistical significance was observed for vascular access, and it did not interact with any other variables, including age (interaction P-value of .72).
For the meta-analysis, we considered data of the present study together with data from 4 studies (n = 2125) that presented information regarding the occurrence of complications at the vascular access site and severe bleeding14-17 and 3 studies (n = 1056) that described the rates of composite events, death, MI, and stroke.14,15,17 When comparing radial access with femoral access and the systematic use of VCD for acute coronary syndrome patients, although radial access was associated with lower rates of puncture-site related complications (RR, 0.64; 95% CI, 0.43-0.95), no significant effects on severe bleeding (RR, 0.74; 95% CI, 0.37-1.46) or severe cardiovascular adverse events (RR, 0.69; 95% CI, 0.30-1.58) based on the access site were observed (Figure 2).
Discussion
The findings of this pilot study involving operators with expertise in both types of vascular access suggested that femoral artery puncture guided by an anatomic landmark, followed by the use of VCD for hemostasis, noted vascular complication rates similar to those of radial access in a population at risk of vascular access-site related bleeding. The rate of severe bleeding was low, which was predominantly determined by hematomas >5 cm. The results were corroborated by those of a meta-analysis that included few publications, thus reflecting the scarcity of comparative studies with the same design.
The largest randomized study comparing hemostasis obtained by manual compression compared with that obtained by VCD indicated the non-inferiority of the latter based on the 30-day vascular complications; there was a significant reduction in time to attain hemostasis in a population of patients who underwent diagnostic procedures.18 However, current registries assessing patients with clinical conditions predisposed to bleeding and the currently used VCDs suggested potential clinical benefits associated with the use of these devices. A British national registry compared the management of femoral access after PCI for 271,845 patients with a wide spectrum of coronary atherosclerotic diseases and showed that 30-day mortality rates were lower for patients with VCDs. This finding was confirmed after correction with a propensity-score analysis.19 The benefits were more evident among women, patients with acute symptoms, and patients with recent thrombolysis. A retrospective analysis of the CathPCI registry analyzed 2,056,585 PCI procedures performed between 2009 and 2013 (VCD was used for 1,053,155 cases) and showed that VCD use was associated with an absolute RR of 0.36% in complication rates associated with the access site (95% CI, 0.31-0.42) and of 0.73% in severe bleeding rates (95% CI, 0.64-0.82).20 Rates of severe bleeding were 3.6% for operators who used VCDs for >80% of cases and 5.7% among those using VCDs for <20% of procedures, thereby confirming the relevance of technical proficiency.
There are few comparative randomized studies of radial access with femoral access and the routine use of VCD. Most studies were inconclusive, because they involved a small number of cases.14-17 Recent results from studies with larger populations have indicated the benefits of VCD compared with manual compression. A Korean registry of 11,596 patients undergoing PCI for MI from 2011-2015 compared radial access and femoral access with or without the use of VCD by applying propensity-score adjustment.21 The 30-day rate of major adverse cardiovascular events was significantly higher for the femoral group without VCD vs the radial group (5.2% vs 3.2%, respectively; log-rank P<.001), particularly due to the occurrence of severe bleeding (2.2% vs 0.6%, respectively; P<.001). However, when the radial group was compared with the femoral group that included VCD use, no significant difference was found for adverse cardiovascular events (2.6% vs 3.9%, respectively; log-rank P=.06) or for severe bleeding (0.7% vs 1.0%; P=.41). On the other hand, the SAFARI-STEMI study22 compared radial with femoral approaches regarding the outcomes of 30-day total mortality and reflected current practices for primary PCI, such as the high use of new oral antiplatelet agents (91.5%), low use of glycoprotein IIb/IIIa inhibitors (6%), and VCD use for 68.2% of patients in the femoral access group. It was terminated early due to futility after the inclusion of 2292 patients, and there was no difference in the primary outcome rates (1.5% vs 1.3%; P=.69) or severe bleeding (type 3-5) according to the Bleeding Academic Research Consortium criteria (2.3% vs 2.4%; P=.83).
Finally, we attempted to determine which clinical trial model would be capable of effectively comparing the “state of the art” of both vascular access techniques. Although the radial artery is less prone to vascular complications due to its superficial course, small diameter, and ease of compression, the femoral artery requires appropriate operator proficiency and the use of resources that can minimize the greater risk inherent to femoral artery characteristics. Therefore, the current concept of optimal femoral access would involve arterial puncture guided by fluoroscopy, ultrasound-guided puncture for patients with factors predictive of complications (eg, advanced age, female sex, obesity, peripheral arterial disease, use of anticoagulants, and large vessels), micropuncture, femoral artery angiography before the procedure, and VCD.11 No study has provided a comparison of the vascular access sites under these conditions or has considered the operator’s preferred vascular access site. Although we did not use ultrasound-guided punctures, we routinely adopted fluoroscopic anatomical landmarks, which is a strategy that has been validated.23 However, evidence in favor of using a micropuncture kit is limited and without a clear benefit that substantiates its routine use.24
Study limitations. This study included a low number of randomized participants. However, its findings are comparable to those of a previous randomized study with 240 participants performed by the same operators in the setting of non-ST segment elevation acute coronary syndrome (ie, low rate of vascular access-site related complications), with no differences between groups.17 In addition, the follow-up restricted to the in-hospital period plus the lack of standard imaging of the access site may have underestimated the prevalence of complications. Another limitation was its reproducibility of results; the team of operators had enough experience to perform invasive coronary procedures using both approaches, which is not true of all operators in the field.
Although the characteristics of radial access favor it as the technique of choice for percutaneous coronary procedures, randomized studies with adequate statistical power are warranted to compare the state of the art of both vascular access techniques, because femoral access is still preferred by a large number of operators who produce consistent results with low complication rates.
Conclusion
Adherence to the technical principles that guide femoral artery punctures and the routine use of VCD promote low rates of severe complications related to the femoral access site in patients undergoing primary PCI that are similar to the rates of using radial artery access in the same clinical scenario.
From 1the Santa Casa de Marília, São Paulo, Brazil; 2Instituto Dante Pazzanese de Cardiologia, São Paulo, Brazil; 3Faculdade de Medicina de Marília, São Paulo, Brazil; 4Rede D´Or São Luiz, São Paulo, Brazil; 5Rede D´Or São Luiz, Rio de Janeiro, Brazil; and 6Hospital do Coração de Londrina, Paraná, Brazil.
Disclosure: The authors have completed and returned the ICMJE Form for Disclosure of Potential Conflicts of Interest. The authors report no conflicts of interest regarding the content herein.
Manuscript accepted March 11, 2020.
Address for correspondence: Pedro Beraldo de Andrade, MD, PhD, Santa Casa de Marília, Avenida Vicente Ferreira, 828, Marília - São Paulo, Brazil. Email: pedroberaldo@gmail.com
- Neumann FJ, Sousa-Uva M, Ahlsson A, et al. 2018 ESC/EACTS guidelines on myocardial revascularization. Eur Heart J. 2019;40:87-165.
- Mason PJ, Shah B, Tamis-Holland JE, et al. An update on radial artery access and best practices for transradial coronary angiography and intervention in acute coronary syndrome: a scientific statement from the American Heart Association. Circ Cardiovasc Interv. 2018;11:e000035.
- Kolkailah AA, Alreshq RS, Muhammed AM, et al. Transradial versus transfemoral approach for diagnostic coronary angiography and percutaneous coronary intervention in people with coronary artery disease. Cochrane Database Syst Rev. 2018;4:CD012318.
- Shroff AR, Fernandez C, Vidovich MI, et al. Contemporary transradial access practices: results of the second international survey. Catheter Cardiovasc Interv. 2019;93:1276-1287.
- Valle JA, Kaltenbach LA, Bradley SM, et al. Variation in the adoption of transradial access for ST-segment elevation myocardial infarction: insights from the NCDR CathPCI registry. JACC Cardiovasc Interv. 2017;10:2242-2254.
- Valgimigli M, Frigoli E, Leonardi S, et al. Radial versus femoral access and bivalirudin versus unfractionated heparin in invasively managed patients with acute coronary syndrome (MATRIX): final 1-year results of a multicentre, randomised controlled trial. Lancet. 2018;392:835-848.
- Tröbs M, Achenbach S, Plank PM, et al. Predictors of technical failure in transradial coronary angiography and intervention. Am J Cardiol. 2017;120:1508-1513.
- Azzalini L, Tosin K, Chabot-Blanchet M, et al. The benefits conferred by radial access for cardiac catheterization are offset by a paradoxical increase in the rate of vascular access site complications with femoral access: the Campeau radial paradox. JACC Cardiovasc Interv. 2015;8:1854-1864.
- Hulme W, Sperrin M, Kontopantelis E, et al. Increased radial access is not associated with worse femoral outcomes for percutaneous coronary intervention in the United Kingdom. Circ Cardiovasc Interv. 2017;10:e004279.
- Blake SR, Shahzad A, Aggarwal SK, et al. Radial versus femoral vascular access in ST-elevation myocardial infarction: are the results of femoral operators unfairly represented in observational research? Am Heart J. 2019;210:81-87.
- Azzalini L, Jolicoeur EM. The wise radialist’s guide to optimal transfemoral access: selection, performance, and troubleshooting. Catheter Cardiovasc Interv. 2017;89:399-407.
- Mehran R, Rao SV, Bhatt DL, et al. Standardized bleeding definitions for cardiovascular clinical trials: a consensus report from the Bleeding Academic Research Consortium. Circulation. 2011;123:2736-2747.
- Rathore S, Stables RH, Pauriah M, et al. A randomized comparison of TR band and Radistop hemostatic compression devices after transradial coronary intervention. Catheter Cardiovasc Interv. 2010;76:660-667.
- Chodór P, Kurek T, Kowalczuk A, et al. Radial vs femoral approach with StarClose clip placement for primary percutaneous coronary intervention in patients with ST-elevation myocardial infarction. RADIAMI II: a prospective, randomised, single centre trial. Kardiol Pol. 2011;69:763-771.
- Alonzo A, Rigattieri S, Giovannelli F, et al. Transfemoral approach with systematic use of FemoSeal™ closure device compared to transradial approach in primary angioplasty. Catheter Cardiovasc Interv. 2016;87:849-854.
- Louvard Y, Ludwig J, Lefèvre T, et al. Transradial approach for coronary angioplasty in the setting of acute myocardial infarction: a dual-center registry. Catheter Cardiovasc Interv. 2002;55:206-211.
- Andrade PB, Mattos LA, Rinaldi FS, et al. Comparison of a vascular closure device versus the radial approach to reduce access site complications in non-ST-segment elevation acute coronary syndrome patients: the Angio-Seal versus the radial approach in acute coronary syndrome trial. Catheter Cardiovasc Interv. 2017;89:976-982.
- Schulz-Schüpke S, Helde S, Gewalt S, et al. Comparison of vascular closure devices vs manual compression after femoral artery puncture: the ISAR-CLOSURE randomized clinical trial. JAMA. 2014;312:1981-1987.
- Farooq V, Goedhart D, Ludman P, et al; British Cardiovascular Intervention Society and the National Institute for Cardiovascular Outcomes Research. Relationship between femoral vascular closure devices and short-term mortality from 271 845 percutaneous coronary intervention procedures performed in the United Kingdom between 2006 and 2011: a propensity score-corrected analysis from the British Cardiovascular Intervention Society. Circ Cardiovasc Interv. 2016;9:e003560.
- Wimmer NJ, Secemsky EA, Mauri L, et al. Effectiveness of arterial closure devices for preventing complications with percutaneous coronary intervention: an instrumental variable analysis. Circ Cardiovasc Interv. 2016;9:e003464.
- Kim N, Lee JH, Jang SY, et al. Radial versus femoral access with or without vascular closure device in patients with acute myocardial infarction. Am J Cardiol. 2019;123:742-749.
- Le May M, Wells G, So D, et al. Safety and efficacy of femoral access vs radial access in ST-segment elevation myocardial infarction: the SAFARI-STEMI randomized clinical trial. JAMA Cardiol. 2020;5:126-134.
- Marquis-Gravel G, Tremblay-Gravel M, Lévesque J, et al. Ultrasound guidance versus anatomical landmark approach for femoral artery access in coronary angiography: a randomized controlled trial and a meta-analysis. J Interv Cardiol. 2018;31:496-503.
- Dorman SH, Obaid DR. Vascular access and closure for cardiovascular intervention. Heart. 2019;105:1279-1288.







