Ultra-Low Contrast Percutaneous Coronary Intervention to Minimize the Risk for Contrast-Induced Acute Kidney Injury in Patients With Severe Chronic Kidney Disease
Abstract: Background. The incidence of contrast-induced acute kidney injury (CI-AKI) is particularly high in patients with severe chronic kidney disease (CKD). Novel contrast-sparing strategies are warranted to guarantee the benefit of revascularization in this challenging and growing patient population. We aimed to evaluate the feasibility of an ultra-low contrast volume percutaneous coronary intervention (ULC-PCI) protocol in patients with severe CKD. Methods. The ULC-PCI protocol is based on the prespecification of the maximum contrast volume to be administered, extensive intravascular ultrasound (IVUS) and/or dextran-based optical coherence tomography (OCT) guidance, and use of diluted contrast media. We created a retrospective registry to compare the outcomes of the ULC-PCI protocol vs conventional angiography-based PCI in patients with estimated glomerular filtration rate (eGFR) <30 mL/min/1.73 m2, applying no angiographic or procedural restriction criteria. Results. We included 111 patients (ULC-PCI group, n = 8; conventional group, n = 103). Baseline clinical and angiographic characteristics were similar between groups. Contrast volume (8.8 mL [interquartile range, 1.3-18.5] vs 90 mL [interquartile range, 58-140 mL]; P<.001) was markedly lower in the ULC-PCI group. Technical success was achieved in all ULC-PCI procedures; in 7 of the 8 cases (88%), the ULC-PCI protocol was also successful (contrast-volume-to-eGFR ratio <1). The incidence of CI-AKI was 0% vs 15.5% in the ULC-PCI and conventional groups, respectively (P=.28). Procedures in the ULC-PCI group included the use of rotational atherectomy, two-stent bifurcation PCI, and mechanically supported chronic total occlusion PCI. Conclusions. An ULC-PCI protocol in patients with advanced CKD is feasible, appears to be safe, and has the potential to decrease the incidence of CI-AKI, compared with angiographic guidance alone.
J INVASIVE CARDIOL 2019;31(6):176-182. Epub 2019 March 15.
Key words: contrast-induced acute kidney injury, CI-AKI, contrast-induced nephropathy, CIN, percutaneous coronary intervention
Renal insufficiency is the second most common cause for surgical turn-down in patients with multivessel coronary artery disease (CAD) requiring revascularization, and such patients suffer increased short-term and long-term mortality rates when revascularization is provided by percutaneous coronary intervention (PCI).1 This finding can be related to a variety of factors and complications arising in the postprocedural period, such as contrast-induced acute kidney injury (CI-AKI).
CI-AKI is a common complication of PCI (7% in the National Cardiovascular Data Registry Cath-PCI registry),2 although it most often manifests as an asymptomatic and transient increase in serum creatinine, without any clinical consequences.3 However, CI-AKI can develop in more than one-quarter of patients with an estimated glomerular filtration rate (eGFR) <30 mL/min/1.73 m2, for whom the incidence of in-hospital dialysis is >4%.2 Additionally, in patients with chronic kidney disease (CKD), even transient renal damage can have adverse consequences on long-term outcomes, including mortality.4
Among the factors linked to the development of CI-AKI, contrast volume plays a major role, as it has been linearly associated with the development of such complications.2,5,6 Therefore, efforts should be made to develop and implement contrast-sparing protocols to provide CAD patients with advanced CKD with state-of-the-art PCI, while guaranteeing preservation of renal function. The aim of this study was to analyze the outcomes of an ultra-low contrast volume PCI (ULC-PCI) protocol in patients with severe CKD requiring percutaneous revascularization.
Methods
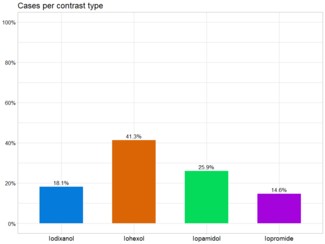
ULC-PCI protocol. The ULC-PCI protocol was developed and implemented by one experienced operator (LA) between January 2017 and April 2018 for non-emergent PCIs in patients with an eGFR ≤30 mL/min/1.73 m2 not on dialysis. This protocol is based on the following principles: (1) All patients receive CI-AKI prophylaxis according to guidelines7 — specifically, isotonic saline (1.0-1.5 mL/kg/h, or 0.5 mL/kg/h in cases of left ventricular ejection fraction [LVEF] <35% or decompensated heart failure) is administered intravenously, from 12 hours before up to 24 hours after contrast media exposure; (2) prespecification of the maximum contrast volume to be administered (contrast-volume-to-estimated-glomerular-filtration-rate [CV/eGFR] ratio is kept <18); (3) diagnostic coronary angiogram and PCI are separated by several days; (4) low-osmolar contrast media (ioversol, Optiray; Guerbet) is utilized and diluted to 50% with normal saline; (5) a “metallic roadmap” for PCI is created by wiring key side branches to provide topographic guidance during the procedure; and (6) intravascular imaging is extensively utilized. No restriction was applied with regard to angiographic characteristics (eg, chronic total occlusion [CTO], left main, bifurcations, etc) or procedural factors (eg, need for rotational atherectomy).
Intravascular imaging. Intravascular imaging is the mainstay of the ULC-PCI protocol and is performed at every key procedural step, including baseline (when feasible), predilation and adjunctive plaque-modification techniques (eg, rotational atherectomy, scoring/cutting balloon, etc), stenting, postdilation, and confirmation of final result. In our study, intravascular imaging was based on the following: (1) intravascular ultrasound (IVUS), which was performed with the 40 MHz Opticross catheter and the Polaris workstation (Boston Scientific) utilizing 0.5 mm/s pullbacks; and (2) dextran-based optical coherence tomography (OCT) provided by the Dragonfly Duo catheter and the Optis workstation (Abbott Vascular) with 54 mm or 75 mm pullbacks. OCT requires displacement of the red blood cells from the vessel lumen during image acquisition, which is usually accomplished using contrast media. In the ULC-PCI protocol, contrast media was substituted by dextran-40 (Plander 40,000; Fresenius), a colloid with similar viscous properties. Dextran-based OCT has been shown to provide excellent image quality and very good agreement with conventional contrast media-based OCT.9,10 Dextran was administered through the cath lab automated injector (CVi; Acist Medical Systems). Injection parameters were similar to those of standard contrast-media based OCT (flow rate, 4.0 mL/s [left coronary] or 3.5 mL/s [right coronary]; total volume, 14.0 mL; pressure, 400 psi; rise time, 0.0 s).
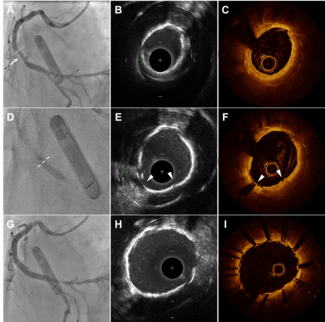
The choice of IVUS vs OCT was left at the operator’s discretion and was based on the consideration of several factors. In cases of CTO, aorto-ostial disease, and large vessels, IVUS was preferred. When the procedure was expected to require numerous imaging runs, involved bifurcation stenting, or in cases of suboptimal IVUS image quality, OCT was chosen. Examples of dextran-based OCT-guided and IVUS-guided PCIs are shown in Supplemental Figures S1 and S2, respectively (supplemental figures available at www.invasivecardiology.com).
Study population. This was a retrospective, single-center study including all subjects with an eGFR <30 mL/min/1.73 m2 and not on dialysis undergoing PCI at our institution for non-emergent indications between January 2012 and April 2018. Patients were divided into two groups: ULC-PCI (as previously described) and conventional PCI (performed without adhering to the strict recommendations outlined above). Conventional PCIs were performed both before and after the introduction of the ULC-PCI protocol by several operators. Follow-up was performed by means of phone interview, review of hospital records, or outpatient visit. All patients signed an informed consent, approved by the local ethics committee, for procedural data collection and for the anonymous use of data for retrospective evaluation.
Definitions. Using the most recent preprocedural serum creatinine level as baseline, eGFR was calculated using the Modification of Diet in Renal Disease equation. Complex PCI was defined as a total stent length >60 mm, ≥3 stents implanted, 3 vessels treated, chronic total occlusion (CTO), or rotational/laser atherectomy. CTO was defined as a 100% stenosis with TIMI flow grade 0 for at least 3 months. Technical success was defined as a residual stenosis <30% with TIMI flow grade 3. For zero-contrast PCIs, a residual area stenosis <30% by IVUS or OCT was regarded as technical success. ULC-PCI protocol success was defined as achieving technical success while maintaining a CV/eGFR ratio <1.
The primary in-hospital outcome was CI-AKI, which was diagnosed using the change from preprocedural to peak serum creatinine levels within 72 hours post PCI. CI-AKI was defined and graded according to the Acute Kidney Injury Network (AKIN) definition:11 AKI stage 1, ≥0.3 mg/dL or ≥50%-100% increase in serum creatinine; AKI stage 2, >100%-200% increase in serum creatinine; AKI stage 3, >200% increase in serum creatinine or increase in serum creatinine to ≥4.0 mg/dL with an acute increase of ≥0.5 mg/dL. CI-AKI requiring dialysis was defined as the new need for in-hospital renal replacement therapy. The primary outcome on follow-up was a composite of all-cause death and new need for dialysis. Other outcomes included each component of the primary endpoint separately, target-vessel failure (a composite of cardiac death, target-vessel myocardial infarction, and target-vessel revascularization) and its individual components, and definite/probable stent thrombosis.
Statistical analysis. Continuous variables are presented as median (interquartile range [IQR, defined as 25th-75th percentile]) and Mann-Whitney U-test was used for comparisons. Categorical variables are presented as frequency (percentages), and compared using Chi-square test or Fisher’s exact test, as appropriate. For all tests, a P<.05 was considered significant. Statistical analysis was performed using SPSS 24 (IBM Corporation).
Results
Baseline clinical characteristics. During the study period, a total of 111 out of 7498 patients (1.5%) met the inclusion criteria. Eight ULC-PCIs were performed and compared with 103 conventional PCIs. In general, there were no differences in clinical characteristics between the ULC-PCI and conventional groups (Table 1). In particular, median age was 76 years overall (IQR, 71-81 years), three-quarters of patients were men, and the prevalence of cardiovascular risk factors and conditions was very high (56% of patients had diabetes mellitus, 54% had prior myocardial infarction, 60% had prior PCI, and 25% had prior coronary artery bypass graft surgery). ULC-PCI patients had lower eGFR compared with subjects in the conventional group (19.0 mL/min/1.73 m2 [IQR, 17.0-23.0 mL/min/1.73 m2] vs 25.3 mL/min/1.73 m2 [IQR, 20.6-28.5 mL/min/1.73 m2], respectively; P=.02). More than half of the study population had left ventricular dysfunction. There were no differences in the Mehran CI-AKI risk score (the majority of patients in both groups were in the high-risk or very-high risk categories) or in the indication for PCI.
Angiographic and procedural data. Table 2 shows angiographic and procedural data of the study population. There were no differences in the target vessel for PCI (the left anterior descending [LAD] was the most frequent vessel in both groups), lesion complexity (most lesions were B2 or C according to the ACC/AHA classification), CTO, complex PCI, vascular access, use of rotational atherectomy, and type of stents utilized. Total stent length tended to be longer in ULC-PCI patients (60 mm [IQR, 50-76 mm] vs 37 mm [IQR, 22-56 mm], respectively; P=.06). As expected, contrast volume (8.8 mL [IQR, 1.3-18.5 mL] vs 90 mL [IQR, 58-140 ml], respectively; P<.001) and the contrast volume/eGFR ratio (0.5 [IQR, 0.1-0.8] vs 3.9 [IQR, 2.3-5.9]; P<.001) were lower in the ULC-PCI group, which also required longer fluoroscopy time. None of the ULC-PCI patients had a contrast volume/creatinine clearance ratio >3.7, which has been identified as a risk factor for CI-AKI,12 while 51% of subjects in the conventional group did (P<.01). Technical success was high and similar between groups. In particular, all 8 ULC-PCIs were successful (100%). In all but 1 case (88%), the ULC-PCI protocol was also successful. In the remaining patient, the CV/eGFR ratio exceeded 1 due to IVUS catheter entrapment during the final pullback in the distally implanted stent, which required additional maneuvers (mother-and-child catheter-assisted pull) to solve. Additionally, in this case, an Ellis type 2 perforation was noted at the entrapment site (probably due to balloon angioplasty performed in an attempt to release the entrapped IVUS probe), which was successfully treated with a covered stent. Contrast volume in this case was 60 mL, and CV/eGFR ratio was 2.22. The patient did not suffer CI-AKI and recovered uneventfully.
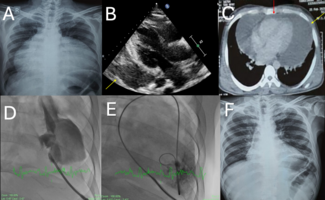
ULC-PCI data. Detailed data of the eight ULC-PCI patients and procedures are shown in Table 3. All patients had B2 or C type lesions. One subject underwent zero-contrast dextran-based OCT-guided PCI on an in-stent restenosis in a diagonal branch13 (Supplemental Figure S1) and subsequently an IVUS-guided, ULC-PCI protected with an Impella device (Abiomed) of a distal LAD-CTO, which was crossed antegradely and required rotational atherectomy of an under-expanded stent and the occlusion14 (Supplemental Figure S2). Another subject underwent complex distal left main bifurcation stenting (T-stenting) using rotational atherectomy.15 Most cases required cutting or scoring balloon atherectomy due to fibrocalcified disease. In 7 of the 8 cases, the CV/eGFR ratio was kept <1; the only exception was the aforementioned patient with IVUS catheter entrapment. IVUS guidance was used in 4 patients, dextran-based OCT was used in 3 patients, and 1 patient received both IVUS and dextran-based OCT guidance.
Incidence of CI-AKI. Figure 1 shows CI-AKI incidence in the ULC-PCI and conventional groups. In the ULC-PCI group, no patient suffered CI-AKI, while 1 patient who underwent zero-contrast PCI had an increase in postprocedural creatinine diagnostic of AKI (+0.40 mg/dL; stage 1 AKI) (Table 3). On the other hand, a total of 16 patients (15.5%) suffered CI-AKI in the conventional group, although the difference failed to reach statistical significance (P=.28). Ten of those 16 patients (9.7%) had stage 1 AKI and 6 patients (5.8%) had stage 3 AKI. The incidence of CI-AKI requiring dialysis was 0% in the ULC-PCI group vs 4.9% (n = 5) in the conventional PCI group (P=.68).
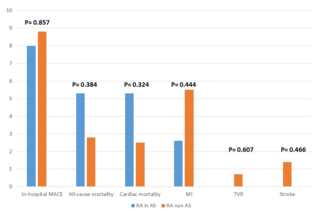
Follow-up. Follow-up was available for 98/111 patients (88%), including all 8 ULC-PCI patients (100%) and 90/103 (87%) in the conventional group. Median follow-up was 353 days (IQR, 148-760 days). There were no differences in the primary endpoint of all-cause death or new need for dialysis (50.0% for ULC-PCI vs 44.4% for conventional PCI; P=.52) or its separate components (Table 4). Similarly, there were no differences between groups in the incidence of target-vessel failure, its individual components, or definite/probable stent thrombosis.
Discussion
Our main study findings are: (1) at a high-volume center specializing in complex PCI, 1.5% of patients had an eGFR ≤30 mL/min/1.73 m2 and were not on chronic dialysis, and thus could potentially benefit from an ULC percutaneous revascularization; (2) our ULC-PCI protocol was reasonably safe, effective, and applicable without lesion restriction, as all patients were successfully treated (despite high lesion complexity) and did not develop CI-AKI; and (3) our ULC-PCI protocol has the potential to reduce the incidence of CI-AKI, compared with a conventional approach, although our small sample size prevented the identification of a statistically significant difference in CI-AKI rates.
CI-AKI is very common in patients with advanced CKD. In the National Cardiovascular Data Registry Cath-PCI registry,2 subjects with an eGFR <30 mL/min/1.73 m2 had a 26.6% incidence of CI-AKI, with 4.3% requiring in-hospital dialysis. Additionally, CI-AKI has repeatedly been associated with a higher incidence of long-term mortality, myocardial infarction, bleeding, need for dialysis, and stent thrombosis.16,17 Maioli et al4 showed that subjects with moderate-to-severe renal dysfunction (creatinine clearance <60 mL/min) are particularly vulnerable to adverse CI-AKI related events. In their study, the incidence of CI-AKI (defined as an absolute increase ≥0.5 mg/dL over baseline serum creatinine within 3 days) was 12.1%. Among those subjects, 18.6% suffered persistent renal damage (a relative decrease of creatinine clearance ≥25% over baseline at 3 months). At 5-year follow-up, CI-AKI patients suffered higher all-cause mortality. Remarkably, although the impact of CI-AKI was greater in patients who suffered persistent renal damage, subjects who developed transient renal damage also had decreased survival compared with subjects with no CI-AKI. This suggests that CI-AKI might exert adverse outcomes at three different levels: (1) acutely, by triggering the need for dialysis; (2) in the short term, by irreversibly decreasing renal function; and (3) in the long term, by impacting survival. Additionally, the actual long-term impact of CI-AKI in contemporary cohorts of CKD patients undergoing complex PCI might be greater, as only 54.8% of patients underwent PCI and 8.5% had severe CKD (creatinine clearance <30 mL/min) in Maioli et al.4
Several studies identified a linear association between contrast volume and the development of CI-AKI,2,5,6 which is particularly relevant in complex PCI, where large volumes of contrast media are administered. This could be further compounded (and amplified) by the fact that such interventions often involve tackling multiple lesions and utilize aggressive plaque modification techniques, which can in turn lead to hemodynamic instability and renal hypoperfusion, which have been shown to trigger AKI.2,3
Therefore, contrast-sparing strategies for PCI are warranted. Recently, Gurm et al18 found that ULC-PCI (defined as contrast volume less than or equal to the patient’s estimated creatinine clearance) was independently associated with a lower risk of CI-AKI and CI-AKI requiring dialysis. These benefits were most evident in patients with a high predicted risk of AKI. However, no technical insights on how to achieve the ULC goal were provided, as this was a population-based study. The MOZART (Minimizing cOntrast utiliZation With IVUS Guidance in coRonary angioplasty) trial19 proved the feasibility of utilizing an IVUS-based low-contrast PCI protocol. In their single-center trial of 83 patients, a strong reliance on IVUS imaging and other contrast-sparing strategies, as utilized in the present study (such as utilizing diluted contrast), allowed a remarkable decrease in total contrast volume, compared with traditional angiography-based PCI (20.0 mL vs 64.5 mL, respectively; P<.001). The ongoing MOZART II trial (ClinicalTrials.gov NCT02743156) is powered to assess clinical outcomes (CI-AKI), and will further shed light on the clinical usefulness of such an approach.
Ali et al8 recently published their experience treating 31 patients with advanced CKD (eGFR, 16 ± 8 mL/min/1.73 m2) with a zero-contrast PCI protocol based on IVUS guidance, as well as fractional flow reserve and coronary flow reserve to confirm physiological improvement. This strategy resulted in successful PCI, no major adverse cardiovascular events, and preservation of renal function without the need for dialysis, within a median follow-up time of 79 days, in all patients. However, a zero-contrast PCI protocol might have significant drawbacks compared with an ULC-PCI strategy, such as longer procedural times and the inability to safely and quickly rule out major complications. These include: dissection in wired but non-imaged side branches; perforation (although an echocardiogram can be performed at the end of the procedure, this does not rule out delayed effusions due to small perforations); no reflow; and distal embolization. A small contrast injection at the end of the procedure provides the operator with a huge amount of information both in the treated region and in other segments, such as perforation, dissection, stent expansion, residual stenoses, coronary flow, etc. While the benefits of such a maneuver are evident and remarkable, it remains to be proved that even very small amounts of contrast (<10 mL) are deleterious to the patient’s kidney function. Moreover, exclusive reliance on IVUS in such a protocol misses the advantages of OCT guidance, particularly its much faster pullbacks and superior resolution and tissue/stent characterization, which are very useful in case many imaging runs are needed during the procedure for guiding bifurcation PCI, visualizing calcium, etc. Prior to the present study, only anecdotal experience with non-contrast based OCT had been reported in patients with advanced renal failure undergoing PCI.13,20,21 Our study provides further insight into the technical aspects and outcomes of dextran-based OCT-guided PCI. Additionally, compared with both the MOZART trial19 and the study by Ali et al,8 the angiographic and procedural complexity of our ULC-PCI cohort was markedly more pronounced; in fact, the prevalence of B2/C lesions was 100% and median total stent length was 60 mm in our study, compared with 88% and 32 mm in the MOZART trial19 and 42% and 22 mm in Ali et al,8 respectively. Moreover, ours was the only study to apply no angiographic or procedural exclusion criteria, thus allowing the inclusion of CTO-PCI and use of mechanical support and rotational atherectomy in the study cohort.
The choice of dextran as a substitute for contrast in our OCT protocol was motivated by the fact that dextran has comparable viscosity, and provides optimal image quality.10 Although anecdotal cases of acute renal failure associated with dextran infusion (as a volume expander in critically ill patients) has been reported,22 in all such cases the infused volumes exceeded 2 L and tubular cell osmotic nephrosis was observed. However, each OCT pullback in our protocol required 14 mL, and a volume >100 mL of dextran was not administered in any OCT-guided PCIs in our cohort. Therefore, the likelihood of toxic effects of dextran as utilized in our protocol seems very low.
Study limitations. First, this is a retrospective registry utilizing historical controls, so that unknown confounder could have biased our analyses. Second, the very small sample size of the ULC-PCI group could have led to imprecise estimations of key outcomes (namely, ULC-PCI protocol success and CI-AKI) and did not allow the identification of a significant difference in CI-AKI rates between the ULC-PCI and conventional groups. Third, the same issue prevented us from performing adjusted analyses to ascertain whether the ULC-PCI protocol was independently associated with improved outcomes. Finally, all procedures were exclusively performed by one experienced operator, so that the widespread applicability of the ULC-PCI protocol could not be evaluated.
Conclusion
An ULC-PCI protocol in patients with advanced CKD is feasible and appears to be safe. Since no cases of CI-AKI were observed in our cohort, the ULC-PCI strategy has the potential to decrease the incidence of CI-AKI, in-hospital need for dialysis, and further deterioration of renal function, compared with a traditional approach based on angiographic guidance alone. Further larger, prospective, and ideally randomized studies should test this hypothesis.
References
- Waldo SW, Secemsky EA, O’Brien C, et al. Surgical ineligibility and mortality among patients with unprotected left main or multivessel coronary artery disease undergoing percutaneous coronary intervention. Circulation. 2014;130:2295-2301.
- Tsai TT, Patel UD, Chang TI, et al. Contemporary incidence, predictors, and outcomes of acute kidney injury in patients undergoing percutaneous coronary interventions: insights from the NCDR Cath-PCI registry. JACC Cardiovasc Interv. 2014;7:1-9.
- Azzalini L, Spagnoli V, Ly HQ. Contrast-Induced nephropathy: from pathophysiology to preventive strategies. Can J Cardiol. 2016;32:247-255.
- Maioli M, Toso A, Leoncini M, Gallopin M, Musilli N, Bellandi F. Persistent renal damage after contrast-induced acute kidney injury: incidence, evolution, risk factors, and prognosis. Circulation. 2012;125:3099-3107.
- Rihal CS, Textor SC, Grill DE, et al. Incidence and prognostic importance of acute renal failure after percutaneous coronary intervention. Circulation. 2002;105:2259-2264.
- Azzalini L, Vilca LM, Lombardo F, et al. Incidence of contrast-induced acute kidney injury in a large cohort of all-comers undergoing percutaneous coronary intervention: comparison of five contrast media. Int J Cardiol. 2018;273:69-73. Epub 2018 Sep 1.
- Levine GN, Bates ER, Blankenship JC, et al. 2011 ACCF/AHA/SCAI guideline for percutaneous coronary intervention: a report of the American College of Cardiology Foundation/American Heart Association Task Force on Practice Guidelines and the Society for Cardiovascular Angiography and Interventions. J Am Coll Cardiol. 2011;58:e44-e122.
- Ali ZA, Karimi Galougahi K, Nazif T, et al. Imaging- and physiology-guided percutaneous coronary intervention without contrast administration in advanced renal failure: a feasibility, safety, and outcome study. Eur Heart J. 2016;37:3090-3095.
- Frick K, Michael TT, Alomar M, et al. Low molecular weight dextran provides similar optical coherence tomography coronary imaging compared to radiographic contrast media. Catheter Cardiovasc Interv. 2014;84:727-731.
- Ozaki Y, Kitabata H, Tsujioka H, et al. Comparison of contrast media and low-molecular-weight dextran for frequency-domain optical coherence tomography. Circ J. 2012;76:922-927.
- Mehta RL, Kellum JA, Shah SV, et al. Acute kidney injury network: report of an initiative to improve outcomes in acute kidney injury. Crit Care. 2007;11:R31.
- Laskey WK, Jenkins C, Selzer F, et al. Volume-to-creatinine clearance ratio: a pharmacokinetically based risk factor for prediction of early creatinine increase after percutaneous coronary intervention. J Am Coll Cardiol. 2007;50:584-590.
- Azzalini L, Mitomo S, Hachinohe D, Regazzoli D, Colombo A. Zero-contrast percutaneous coronary intervention guided by dextran-based optical coherence tomography. Can J Cardiol. 2018;34:330-332.
- Regazzoli D, Hachinohe D, Demir OM, et al. Minimizing the risk of contrast-induced nephropathy and hemodynamic collapse during chronic total occlusion percutaneous coronary intervention with a percutaneous left ventricular assist device. Cardiovasc Revasc Med. 2018;19:712-716. Epub 2018 Feb 7.
- Slavich M, Gramegna M, Regazzoli D, et al. [Severe coronary artery disease and severely impaired renal function. Focused fluid expansion and ultra-low dose contrast medium administration]. G Ital Cardiol. 2018;19:510-513.
- Valle JA, Mccoy LA, Maddox TM, et al. Longitudinal risk of adverse events in patients with acute kidney injury after percutaneous coronary intervention: insights from the National Cardiovascular Data Registry. Circ Cardiovasc Interv. 2017;10:e004439.
- Giacoppo D, Madhavan MV, Baber U, et al. Impact of contrast-induced acute kidney injury after percutaneous coronary intervention on short- and long-term outcomes: pooled analysis from the HORIZONS-AMI and ACUITY trials. Circ Cardiovasc Interv. 2015;8:e002475.
- Gurm HS, Seth M, Dixon SR, et al. Contemporary use of and outcomes associated with ultra-low contrast volume in patients undergoing percutaneous coronary interventions. Catheter Cardiovasc Interv. 2019;93:222-230. Epub 2018 Aug 25.
- Mariani J Jr, Guedes C, Soares P, et al. Intravascular ultrasound guidance to minimize the use of iodine contrast in percutaneous coronary intervention: the MOZART (Minimizing cOntrast utiliZationWith IVUS Guidance in coRonary angioplasTy) randomized controlled trial. JACC Cardiovasc Interv. 2014;7:1287-1293.
- Karimi Galougahi K, Zalewski A, Leon MB, Karmpaliotis D, Ali ZA. Optical coherence tomography-guided percutaneous coronary intervention in pre-terminal chronic kidney disease with no radio-contrast administration. Eur Heart J. 2016;37:1059.
- Azzalini L, Hachinohe D, Regazzoli D, Colombo A. Ultra-low contrast percutaneous coronary intervention in patients with severe chronic kidney disease. EuroIntervention. 2018;14:896-897.
- Feest TG. Low molecular weight dextran: a continuing cause of acute renal failure. Br Med J. 1976;2:1300.
From the 1Division of Interventional Cardiology, Cardio-Thoracic-Vascular Department, San Raffaele Scientific Institute, Milan, Italy; 2Interventional Cardiology Unit, GVM Care & Research Maria Cecilia Hospital, Cotignola, Italy; 3Invasive Cardiology and Hemodynamics, Humanitas Research Hospital, Rozzano, Italy; 4Division of Cardiology, Department of Medicine, New Tokyo Hospital, Chiba, Japan; 5Sapporo Heart Center, Sapporo Cardio-Vascular Clinic, Sapporo, Japan; and 6Department of Cardiology, Hammersmith Hospital London, London, United Kingdom.
Disclosure: The authors have completed and returned the ICMJE Form for Disclosure of Potential Conflicts of Interest. Dr Azzalini reports honoraria from Abbott Vascular, Guerbet, Terumo, and Sahajanand Medical Technologies; research support from ACIST Medical Systems, Guerbet, and Terumo. The remaining authors report no conflicts of interest regarding the content herein.
The authors report that patient consent was provided for publication of the images used herein.
Manuscript submitted December 11, 2018, and accepted December 20, 2018.
Address for correspondence: Lorenzo Azzalini, MD, PhD, MSc, Division of Interventional Cardiology, Cardio-Thoracic-Vascular Department, San Raffaele Scientific Institute, Via Olgettina 60, 20132 Milan, Italy. Email: azzalini.lorenzo@hsr.it