

Tissue Removal by Ultrasound Evaluation (The TRUE Study): The Jetstream G2 System Post-Market Peripheral Vascular IVUS Study
ABSTRACT: Background. Balloon angioplasty and stenting of infra-inguinal lesions is limited by poor long-term patency rates. Atherectomy decreases plaque burden and provides an alternative means of revascularizing patients with peripheral arterial disease. The Jetstream G2™ (Pathway Medical Technologies, Inc., Kirkland, Washington) is a newer rotational aspiration atherectomy device, uniquely combining rotablation with aspiration capability. We evaluated the debulking properties of this device by analyzing changes in the plaque volume and composition and vessel size using intravascular ultrasound (IVUS) and virtual histology (VH). Freedom from target lesion revascularization (TLR) at 6 and 12 months was also evaluated. Methods and Results. Eighteen patients with peripheral arterial disease requiring intervention (severe claudication despite optimal medical treatment or critical limb ischemia) were treated with rotational atherectomy. The mean age was 69.6 ± 11 years, 66.7% were male, and 44.4% had diabetes. The mean total plaque volume decreased by 56.6 mm3 (479.8 ± 172.5 mm3 to 423.2 ± 156.6 mm3; p < 0.0001), which resulted in a mean luminal volume increase of 64.3 mm3 (148.4 ± 84.1 mm3 to 212.7 ± 72.1 mm3; p <0.0001). This was achieved without significant Dotter effect with either technique, as evidenced by the virtually unchanged vessel volume before and after treatment (628.3 ± 158.5 mm3 and 635.9 ± 169.0 mm3, respectively; p = 0.22). There was a significant reduction in fibrotic and fibro-fatty plaque volume, with no appreciable effect on necrotic core and dense calcium. There were no reported procedure-related complications and the 6- and 12-month TLR rate was 11% (2/18). Conclusion. Atherectomy with the Jetstream G2 system results in substantial plaque volume reduction by removing fibrotic and fibro-fatty plaque. This resulted in substantial luminal volume expansion without concomitant vessel expansion. There were no major procedure-related complications, along with a relatively low 6- and 12-month rate of TLR. Future studies involving a larger number of patients are warranted to examine the potential clinical benefits of this promising technology.
J INVASIVE CARDIOL 2011;23:269–273
Key words: atherectomy; intravascular ultrasound; Jetsteam G2; peripheral vascular disease; target-vessel revascularization
_____________________________________
Peripheral arterial disease (PAD) of the lower extremities has an incidence and prevalence nearly equal to coronary artery disease and is a major cause of morbidity in the United States.1 Clinical manifestations vary from intermittent claudication to critical limb ischemia and gangrene. PAD is also a risk factor for lower-extremity amputation and for systemic vascular disease in coronary, cerebral, and renal vessels.2 Data from the Framingham Heart Study show that PAD and coronary atherosclerosis share common risk factors, including diabetes mellitus, dyslipidemia, cigarette smoking, hypertension and advanced age.3
The management of severe symptomatic PAD has historically included highly-invasive procedures, including bypass surgery. Percutaneous intervention with balloon angioplasty showed similar short-term results in amputation-free survival.4 However, balloon angioplasty of femoropopliteal lesions is limited by a poor long-term patency rate.5–7 Balloon and stent-based interventions increase the lumen size by expanding the vessel (the ‘Dotter’ effect). Barring one recent study, stenting of femoropopliteal occlusions has been shown to have significant restenosis rates as well and does not appear to improve outcomes after intervention when compared with angioplasty alone.8–10
During the past decade, the endovascular treatment of PAD has become more widespread because of significant advances in technologies such as atherectomy. The promise of atherectomy is to avoid the complications of traditional angioplasty, such as dissection, elastic recoil, and disruption of the internal elastic lamina, resulting in overwhelming neo-intima and smooth muscle cell proliferation.11 Percutaneous removal of the atherosclerotic material may offer an alternative approach for improving procedural success, as well as long–term outcomes.12
The Jetstream G2™ (Pathway Medical Technologies, Inc., Kirkland, Washington) is a rotational aspiration atherectomy device, uniquely combining rotablation with aspiration capability. The device is designed to treat the wide spectrum of diseases found in patients with PAD, including hard and soft plaque, calcium, thrombus, and fibrotic lesions. The objective of our study was to investigate the debulking properties of this device by analyzing changes in plaque volume and composition and vessel size using intravascular ultrasound (IVUS) and virtual histology (VH). Freedom from target lesion revascularization (TLR) at 6 and 12 months was also evaluated.
Methods
Inclusion criteria. Patients who were referred for treatment of PAD were enrolled in this study if they met the following criteria: age ≥ 18 years; target lesion(s) located in a superficial femoral, popliteal or tibioperoneal trunk (TPT) artery with the vessel < 6.5 mm in diameter; reference vessel lumen (proximal to target lesion) ≥ 3.0 mm; and patient is an acceptable candidate for percutaneous intervention using the Jetstream G2 System in accordance with its labeled indications and instructions for use and has signed an approved informed consent form.
Exclusion criteria. Potential patients were excluded from the study if they had any of the following features: uncontrolled allergy to ninitol, stainless-steel or other stent materials or to contrast agent; unable to take appropriate antiplatelet therapy; patient has no distal run-off; interventional treatment is intended for in-stent restenosis at the peripheral vascular site; target vessel with moderate or severe angulation (e.g., > 30°) or tortuosity at the treatment segment; patient has history of coagulopathy or hypercogulable disorder, is undergoing hemodialysis or has impaired renal function (Cr > 2.5 mg/dl) at the time of treatment; patient has evidence of intracranial or gastrointestinal bleeding within last 3 months, history of severe trauma, fracture, major surgery or biopsy of a parenchymal organ within past 14 days, pregnant or nursing a child; or intended interventional treatment includes planned laser, brachytherapy or atherectomy procedure other than Jetstream G2; and finally, patients with nonanalyzable IVUS images.
Rotational atherectomy. The Jetstream G2 consists of a sterile, single-use catheter and control pod and a reusable, compact console that mounts to a standard IV stand. The catheter has an expandable cutting tip that safely debulks and preemptively removes both hard and soft plaque, as well as calcium, thrombus and fibrotic lesions. An aspiration port located just proximal to the cutting blades continually removes excised tissue and thrombus from the treatment site to a collection bag located on the console. A fully recessed masticating system within the aspiration port helps break aspirated material into smaller pieces before removal. The distal portion of the catheter also possesses infusion ports that provide continuous infusion of sterile saline during the atherectomy procedure. Active aspiration is a safety feature that minimizes the risk of distal embolization.13
Intravascular ultrasound analysis. The Eagle Eye® Gold catheter is a 5-French (Fr) compatible catheter that performs intravascular analysis of the culprit lesion, measuring both grey-scale images and Virtual Histology® (VH) over a 0.014˝ guidewire. Automated pullback (1.0 mm/sec) was implemented by using the Track Back® II disposable pullback device. Images were recorded on DICOM format and stored on the s5i™ imaging system hard drive for later analysis. All pullbacks were performed at a set and sufficiently distal point using an external ruler to mark the precise start point. All pullbacks were precisely 60 seconds, or 60 mm in length in order to assure adequate assessment of possible longitudinal displacement of plaque. If there was any evidence of drag on the first run, the studied segment had to adjust to that fact; often, the worst stenosis had to be eliminated from the study so that the segments were truly identical. All images were assessed independently by two experienced reviewers who were blind to the treatment status.
A newer, novel approach to lesion assessment is to include the radiofrequency backscatter information obtained during IVUS to further delineate the composition of the plaque into 4 specific histologic composition categories. VH has been shown to have a high concordance with histopathologic examinations.14 The reproducibility and reliability also translates to longitudinal analysis and volumetric measurements.15
The plaque can be broken down into four primary components: fibrotic, fibro-fatty, necrotic core and dense calcium.16 Fibrous tissue is represented as dark green pixels. Histologically, this tissue type is characterized by bundles of collagen fibers with little to no lipid accumulation in or around the fibrous area. This tissue shows high mechanical stability. Fibro-fatty tissue is denoted by light green pixels. Fibro-fatty tissue contains little to no necrotic core or cholesterol clefts, but is instead composed of loosely packed collagen fibers (fibrous tissue) and proteoglycan, and can be cellular, with or without interspersed foam cells. Necrotic core is represented by red pixels. This tissue type is characterized by a high concentration of extracellular lipid within a necrotic core that is made up of remnants of dead, lipid-filled smooth muscle cells, foam cells and trapped white blood cells. This tissue shows poor mechanical stability. White pixels represent dense calcium on VH IVUS. This tissue is characterized by compact calcium crystals and shows high mechanical stability.17
Quantitative assessment of the treated segments was performed using the VIAS® Image Analysis Software, version 3.0. Since VH is acquired in a gated method, the use of a motorized pullback allows reliable and reproducible plaque volumes for overall and specific studied segments. The external elastic membrane (EEM) was used to denote the overall area of the vessel, which is defined as the interface between the inner edge of the adventitia as it abuts the sonolucent zone. The lumen area was determined by tracing the leading intimal edge of the plaque burden, with the difference between the EEM and lumen denoted as the plaque area.
All patients underwent two runs of IVUS: a pre-treatment run to assess the severity and morphology of the plaque composition and a post-Pathway run to assess changes in overall and histologic volumes. All segments were later analyzed in a 20-mm segment centered on the target lesion site. By using one or more axial landmarks and a known pull-back speed, we achieved identical 20-mm long segments on serial studies for comparative analysis. In order to ensure appropriate matching, collateral circulation was assessed and the distance from the collateral to the lesion was also used to ensure that the segments studied were identical. Plaque reduction for this volumetric study was defined as the plaque volume change (pre-treatment minus post-treatment) divided by the change in lumen volume (post-treatment minus pre-treatment).
Statistical analysis. The mean differences between pre-procedure and post-procedure measures were analyzed using paired t-tests. All analyses were completed using PASW v. 18.0. A p-value of ≤ 0.05 was considered to indicate statistical significance.
The study was approved by the institutional review board at St. John Hospital and Medical Center.
Results
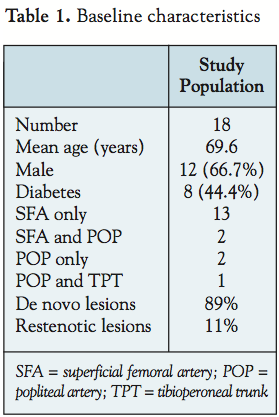 Patient population. PAD required intervention in 18 patients (severe claudication despite optimal medical treatment or critical limb ischemia) were treated with rotational atherectomy (RA). The mean age was 69.6 ± 11 years, 66.7% were male, and 44.4% had diabetes. Thirteen patients had superficial femoral artery lesions (SFA), two had SFA and popliteal artery lesion (POP), two had POP and one had POP and tibioperoneal trunk lesion (TPT). Of the 18 patients, 89% were de novo lesions and 11% were restenotic. The index lesion was studied with IVUS and VH at baseline, and after RA. In no case was pre-dilation needed for the IVUS catheter to cross the stenotic lesions.
Patient population. PAD required intervention in 18 patients (severe claudication despite optimal medical treatment or critical limb ischemia) were treated with rotational atherectomy (RA). The mean age was 69.6 ± 11 years, 66.7% were male, and 44.4% had diabetes. Thirteen patients had superficial femoral artery lesions (SFA), two had SFA and popliteal artery lesion (POP), two had POP and one had POP and tibioperoneal trunk lesion (TPT). Of the 18 patients, 89% were de novo lesions and 11% were restenotic. The index lesion was studied with IVUS and VH at baseline, and after RA. In no case was pre-dilation needed for the IVUS catheter to cross the stenotic lesions.
 Adverse events and follow-up. All study patients were followed for 1 year post-RA, including a 6- and 12-month assessment of TLR. Assessment was made on the basis of clinical follow-up only. Routine surveillance duplex or repeat angiography was not performed. Until the time of the analysis, freedom from TLR and adverse events were available on all 18 patients who had met the 6-month and 1-year follow-up visit criteria. There were no angiographically obvious emboli, dissections, perforations or abrupt closures reported during the study. The 6-month TLR rate was 11% (2/18) and remained the same at 11% (2/18) throughout the 12-month follow-up period.
Adverse events and follow-up. All study patients were followed for 1 year post-RA, including a 6- and 12-month assessment of TLR. Assessment was made on the basis of clinical follow-up only. Routine surveillance duplex or repeat angiography was not performed. Until the time of the analysis, freedom from TLR and adverse events were available on all 18 patients who had met the 6-month and 1-year follow-up visit criteria. There were no angiographically obvious emboli, dissections, perforations or abrupt closures reported during the study. The 6-month TLR rate was 11% (2/18) and remained the same at 11% (2/18) throughout the 12-month follow-up period.
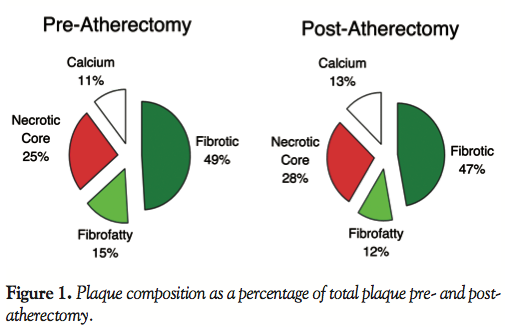
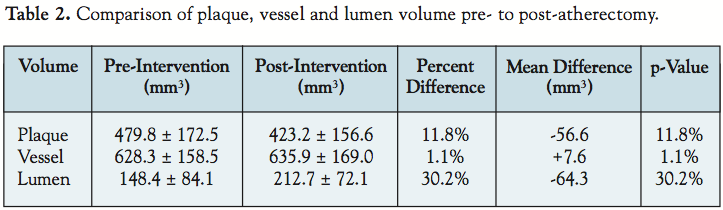 IVUS analysis of plaque volume, lumen volume, and vessel size. Figure 1 shows the percent composition of the plaque pre- and post-RA. Overall, the mean total plaque volume decreased by 56.6 mm3 (479.8 ± 172.5 mm3 to 423.2 ± 156.6 mm3; p < 0.0001), which resulted in a mean luminal volume increase of 64.3 mm3 (148.4 ± 84.1 mm3 to 212.7 ± 72.1 mm3; p < 0.0001) (Table 2). This was achieved without a significant Dottering effect with either technique, as evidenced by the
IVUS analysis of plaque volume, lumen volume, and vessel size. Figure 1 shows the percent composition of the plaque pre- and post-RA. Overall, the mean total plaque volume decreased by 56.6 mm3 (479.8 ± 172.5 mm3 to 423.2 ± 156.6 mm3; p < 0.0001), which resulted in a mean luminal volume increase of 64.3 mm3 (148.4 ± 84.1 mm3 to 212.7 ± 72.1 mm3; p < 0.0001) (Table 2). This was achieved without a significant Dottering effect with either technique, as evidenced by the 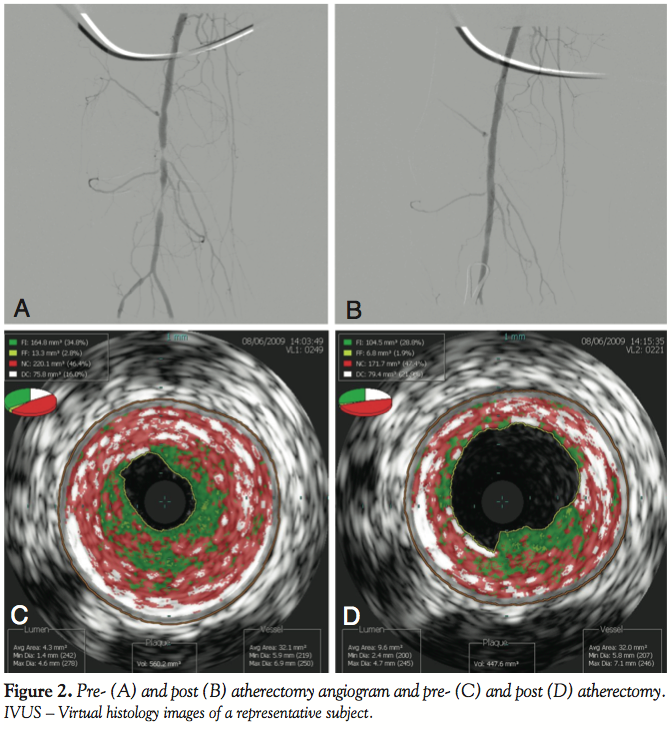 virtually unchanged vessel volume before and after treatment (628.3 ± 158.5 mm3 to 635.9 ± 169.0 mm3; p = 0.22). An angiogram and virtual histology pre- and post-atherectomy of a representative patient is shown in Figure 2. Overall, there was a 43% increase in the size of the lumen despite only reducing the total plaque burden by 11.8%.
virtually unchanged vessel volume before and after treatment (628.3 ± 158.5 mm3 to 635.9 ± 169.0 mm3; p = 0.22). An angiogram and virtual histology pre- and post-atherectomy of a representative patient is shown in Figure 2. Overall, there was a 43% increase in the size of the lumen despite only reducing the total plaque burden by 11.8%.
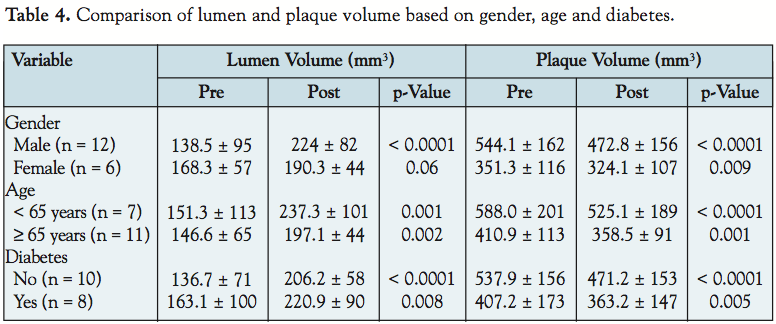
In the subset of patients (7/18) whose post-intervention vessel  volume was smaller than the pre-intervention vessel volume, there remained an equivalent decrease in the plaque volume (421.4 ± 123.4 mm3 to 357.9 ± 100.1 mm3; p = 0.005; Table 3). Table 4 shows the differences in luminal and plaque volume based on gender, age and presence or absence of diabetes. Among each subgroup, the differences remained statistically significant.
volume was smaller than the pre-intervention vessel volume, there remained an equivalent decrease in the plaque volume (421.4 ± 123.4 mm3 to 357.9 ± 100.1 mm3; p = 0.005; Table 3). Table 4 shows the differences in luminal and plaque volume based on gender, age and presence or absence of diabetes. Among each subgroup, the differences remained statistically significant.
 Virtual histology analysis of plaque composition. The lesions were primarily fibrotic in nature, with an average total plaque volume of 64%. Fibro-fatty plaque formed 15% of the total plaque volume on average, whereas necrotic core and dense calcium formed 25% and 11%, respectively. Post-treatment, of the plaque remaining in the vessel, the percentage of fibrotic plaque burden remained at 47% and fibro-fatty plaque accounted for 12%. However, the proportion of necrotic core and dense calcium actually increased to 28% and 13%, respectively (Figure 1).
Virtual histology analysis of plaque composition. The lesions were primarily fibrotic in nature, with an average total plaque volume of 64%. Fibro-fatty plaque formed 15% of the total plaque volume on average, whereas necrotic core and dense calcium formed 25% and 11%, respectively. Post-treatment, of the plaque remaining in the vessel, the percentage of fibrotic plaque burden remained at 47% and fibro-fatty plaque accounted for 12%. However, the proportion of necrotic core and dense calcium actually increased to 28% and 13%, respectively (Figure 1).
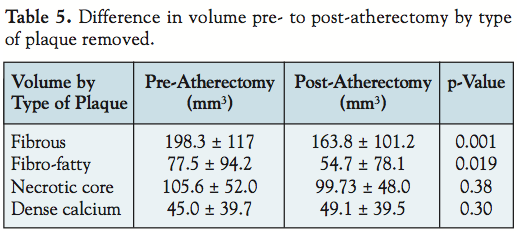 There was significant effect on fibrotic plaque volume (198.3 ± 117 mm3 to 163.8 ± 101.2 mm3; p = 0.001). This represented a 17.4% decrease in fibrotic plaque volume and 58% of the plaque volume removed (Table 5).
There was significant effect on fibrotic plaque volume (198.3 ± 117 mm3 to 163.8 ± 101.2 mm3; p = 0.001). This represented a 17.4% decrease in fibrotic plaque volume and 58% of the plaque volume removed (Table 5).
Fibro-fatty volume decreased significantly pre- to post-RA (77.5 ± 94.2 mm3 to 54.7 ± 78.1 mm3; p = 0.019). There was a total removal of 29.4% of all fibro-fatty tissue, which represents 38.6% of all plaque removed.
Necrotic core plaque was not as amenable to atherectomy. The mean difference in necrotic core plaque volume was not statistically significant (105.6 ± 52.0 mm3 to 99.73 ± 48.0 mm3; p = 0.38). Post-RA, only 5% of all necrotic core was removed, which actually raised the necrotic core percentage of the remaining plaque. Overall, 10% of all plaque removed was necrotic core.
Dense calcium volume was not affected by atherectomy (45.0 ± 39.7 mm3 to 49.1 ± 39.5 mm3; p = 0.30). Post-RA, no appreciable volume was removed, and the percentage of dense calcium to total plaque volume remaining also increased.
Discussion
Traditional atherectomy in lower extremities has major limitations of causing distal embolization.18 The Pathway Jetstream G2 device used in the study has an advantage of aspiration concomitant with atherectomy, thereby reducing if not eliminating all distal embolization. None of the study patients had distal embolization. IVUS has emerged as an important tool in assessing plaque morphology and the ex vivo accuracy of automated plaque characterization by spectral analysis of IVUS has been well established in the coronary19 and carotid circulation.20 VH has been used to examine plaque reduction and luminal gain by atherectomy devices in both coronary21 and peripheral circulation.22 Our study indicates that the mechanism of lumen gain achieved by the Jetstream G2 device is not associated with a “Dottering” effect, but rather related to plaque excision, as evidenced by vessel volume remaining unchanged prior to and after the procedure.
Hassan et al12 showed the utilization of IVUS in an earlier Pathway PV system; however, that study was limited by small numbers, with only 6 patients. Also, in that study, plaque composition by virtual histology with IVUS was not performed. Our study is a multicenter study of 18 patients describing the detailed plaque composition by IVUS, thereby enabling us to quantify the amount of various components of plaque removed. Although this study still had a relatively small sample size, we believe that this is the largest case series that has been reported to date and the first study with the newer Jetstream G2 second-generation device.
Although in our study the type of plaque excised was predominantly fibrous and fibro-fatty, there was little improvement in the necrotic core and dense calcium component of plaque with the second-generation device used in this study. The increase in calcium can interfere with the accurate assessment and visibility of the EEM, and therefore in most cases, the most calcified segment was not studied. More recently, however, the third-generation device (Jetstream G3), which has recently been cleared by the U.S. Food and Drug Administration, has shown promise in removing necrotic core. Because our study was not designed with the intent of assessing and quantifying RA in the specific treatment of necrotic core and dense calcium, future study in these plaque components is needed.
While this device is not a stand-alone device, it did achieve an average lumen of 2.82 mm in diameter, which based on the cutter size, would be the anticipated lumen achievement. We saw a 43% increase in the size of the lumen and 11.8% reduction in the total plaque burden. It is mathematically expected that the plaque reduction measured in percentage will be less than the lumen gain measured in percentage, given the smaller volume off the lumen, as compared to the plaque.
Another noteworthy finding of our study was that patients with a decrease in vessel volume post-intervention (hypothesized to be secondary to spasm) also had significant and equivalent reduction of plaque volume. Even in these patients who were believed to have vessel spasm with significant reduction in plaque, there were no complications, including vessel injury/perforation, obviating the need for additional vasodilators (i.e., nitroglycerin) frequently used in coronary interventions.
Study limitations. The major limitation of this study is the small sample size. Since VH demands that the field of examination be fixed at 10 mm, there were a few patients excluded due to the large size of the superficial femoral artery, which precluded accurate assessment of the EEM. We had to exclude a similar number of subjects to the study population due to unanalyzable IVUS data, the availability of which could have significantly bolstered the sample size. However, to date, this is still the largest study for this technology. In addition, this study was a single treatment strategy and there was no control or comparison group. There is limited correlation between VH IVUS and plaque assessment in non-coronary arterial trees. This is a significant limitation in using a coronary VH IVUS system for assessing limb PAD. We needed to have segments that could reasonably and reproducibly be assessed, which meant that the most calcified segments were often not used. The increase in calcium can interfere with the accurate assessment and visibility of the EEM. In addition, VH can underestimate the extent of deep-wall calcium in the presence of superficial calcium. While this was a very small percentage of the total plaque volume, it is arguable that more calcium was removed than can be appreciated by VH. An additional limitation is that statistical significance is easier to reach with volumetric analysis in this small sample size. However, a substantial reduction in plaque volume and improvement in luminal volume were noted in all the subjects studied who underwent atherectomy with this promising technology.
Conclusion
Atherectomy with the Jetstream G2 system resulted in substantial plaque reduction by removing fibrotic and fibro-fatty plaque. This resulted in substantial plaque volume reduction and luminal volume expansion without causing vessel expansion. Furthermore, there were no major complications during the procedure or index hospitalization, and an acceptable TLR rate was observed after a 1-year follow-up. Future studies in a larger number of patients are warranted to examine the potential clinical benefits of this promising technology.
References
- Gardner AW, Poehlman ET. Exercise rehabilitation programs for the treatment of claudication pain. A meta-analysis. JAMA 1996;275:519–520.
- Criqui MH. Peripheral arterial disease — Epidemiological aspects. Vasc Med 2001;6(3 Suppl):3–7.
- Murabito JM, D’Agostino RB, Silbershatz H, Wilson WF. Intermittent claudication. A risk profile from the Framingham heart study. Circulation 1997;96:44–49.
- Adam DJ, Beard JD, Cleveland T, et al. Bypass versus angioplasty in severe ischaemia of the leg (BASIL): Multicentre, randomised controlled trial. Lancet 2005;366:1925–1934.
- Krepel VM, van Andel GJ, van Erp WF, Breslau PJ. Percutaneous transluminal angioplasty of the femoropopliteal artery: Initial and long-term results. Radiology 1985;156:325–328.
- Matsi PJ, Manninen HI, Söder HK, et al. Percutaneous transluminal angioplasty in femoral artery occlusions: Primary and long-term results in 107 claudicant patients using femoral and popliteal catheterization techniques. Clin Radiol 1995;50:237–244.
- Johnston KW. Femoral and popliteal arteries: Reanalysis of results of balloon angioplasty. Radiology 1992;183:767–771.
- Vroegindeweij D, Vos LD, Tielbeek AV, et al. Balloon angioplasty combined with primary stenting versus balloon angioplasty alone in femoropopliteal obstructions: A comparative randomized study. Cardiovasc Intervent Radiol 1997;20:420–425.
- Zdanowski Z, Albrechtsson U, Lundin A, et al. Percutaneous transluminal angioplasty with or without stenting for femoropopliteal occlusions. A randomized controlled study. Int Angiol 1999;18:251–255.
- Laird JR, Katzen BT, Scheinert D, et al. Nitinol stent implantation versus balloon angioplasty for lesions in the superficial femoral artery and proximal popliteal artery: Twelve-month results from the RESILIENT randomized trial. Circ Cardiovasc Interv 2010;3:267–276.
- Schwarzwälder U, Zeller T. Debulking procedures: Potential device specific indications. Tech Vasc Interv Radiol 2010;13:43–53.
- Hassan AH, Ako J, Waseda K, et al. Mechanism of lumen gain with a novel rotational aspiration atherectomy system for peripheral arterial disease: Examination by intravascular ultrasound. Cardiovasc Revasc Med 2010;11:155–158.
- Pathway Medical Technologies receives FDA clearance to market the Jetstream G2™ System for thrombectomy. Last accessed Jan 5, 2011. www.medicalnewstoday.com/articles/143515.php.
- Nasu K, Tsuchikane E, Katoh O, et al. Accuracy of in vivo coronary plaque morphology assessment. J Am Coll Cardiol 2006;47:2405–2412.
- Prasad A, Cipher D, Prasad A, et al. Reproducibility of intravascular ultrasound virtual histology analysis. Cardiovasc Revasc Med 2008;9:71–77.
- Nair A, Kuban BD, Tuzcu EM, et al. Coronary plaque classification with intravascular ultrasound radiofrequency data analysis. Circulation 2002;106:2200–2206.
- In vivo coronary plaque classification by intravascular ultrasonography. https://www.medscape.com/viewarticle/570565_4. Last accessed Jan 5, 2011.
- Shammas NW, Dippel EJ, Coiner D, et al. Preventing lower extremity distal embolization using embolic filter protection: Results of the PROTECT Registry. J Endovasc Ther 2008;15:270–276.
- Nair A, Margolis MP, Kuban BD, Vince DG. Automated coronary plaque characterization with intravascular ultrasound backscatter: Ex vivo validation. Euro Intervention 2007;3:113–120.
- Diethrich EB, Pauliina Margolis M, Reid DB, et al. Virtual histology intravascular ultrasound assessment of carotid artery disease: The Carotid Artery Plaque Virtual Histology Evaluation (CAPITAL) study. J Endovasc Ther 2007;14:676–686.
- Ikeno F, Braden GA, Kaneda H, et al. Mechanism of luminal gain with plaque excision in atherosclerotic coronary and peripheral arteries: Assessment by histology and intravascular ultrasound. J Interv Cardiol 2007;20:107–113.
- Aboufakher R, Torey J, Szpunar S, Davis T. Peripheral plaque volume changes pre- and post-rotational atherectomy followed by directional plaque excision: Assessment by intravascular ultrasound and virtual histology. J Invasive Cardiol 2009;21:501–505.
_____________________________________
From the Department of Cardiology at St. John Hospital and Medical Center, 22101 Moross Road, Detroit, Michigan.
Disclosures: The study was funded by Pathway Medical Technologies, Inc., Kirkland, Washington. Dr. Thomas Davis is on the advisory board of Pathway Medical Technologies, Inc.
Submitted March 21, 2011, provisional acceptance given April 20, 2011, final version accepted April 25, 2011.
Address for correspondence: Thomas Davis, MD, St. John Hospital and Medical Center, 22101 Moross Road, VEP 2nd Floor, Cardiac Cath Lab, Detroit, MI 48236. Email: tejwant.singh@stjohn.org





