

Regional Cardiac Tamponade Resulting in Hypoxia from Acute Right to Left Inter-Atrial Shunting
ABSTRACT: Loculated pericardial effusion, as a cause of acute hypoxia, is an unusual finding. Here, we describe the case of a patient who underwent percutaneous coronary intervention, complicated by a localized pericardial hematoma compressing the right atrium, resulting in right to left shunting of blood through a patent foramen ovale and subsequent hypoxia. Evacuation of the hematoma was eventually performed via a pericardial window with resolution of hypoxia.
J INVASIVE CARDIOL 2011;23:E96–E98
______________________________________
Regional cardiac tamponade (CT) is an unusual finding most commonly seen in post-operative patients.1–3 We describe a unique case of regional CT sustained after coronary perforation during percutaneous coronary intervention (PCI) resulting in compression of the right atrium, right to left shunting of blood through a patent foramen ovale, and subsequent hypoxia.
Case Report. A 67-year-old male with a history of three-vessel coronary artery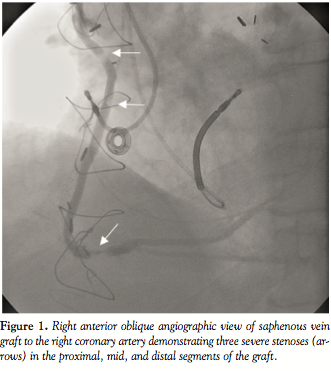 bypass graft surgery 9 years prior, presented with symptoms of progressive angina. Physical examination was unremarkable with normal heart sounds and no audible murmur, rub, or gallop on cardiac auscultation. Echocardiogram prior to admission demonstrated a mildly dilated left ventricle with moderate to severe global hypokinesis and ejection fraction of 25–35%.
bypass graft surgery 9 years prior, presented with symptoms of progressive angina. Physical examination was unremarkable with normal heart sounds and no audible murmur, rub, or gallop on cardiac auscultation. Echocardiogram prior to admission demonstrated a mildly dilated left ventricle with moderate to severe global hypokinesis and ejection fraction of 25–35%.
Coronary and graft angiography revealed patent bypass grafts with 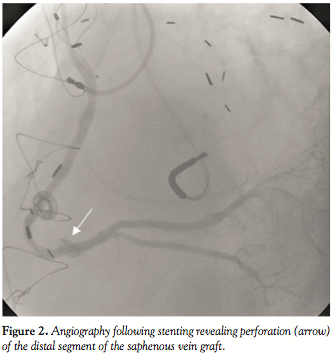 three tandem stenoses of 80–90% involving the proximal, mid, and distal segments of the saphenous vein graft (SVG) to the right coronary artery (Figure 1). PCI was performed successfully with deployment of three non-overlapping bare-metal stents without the use of a distal embolization protection device due to lack of sufficient distal space in the SVG for positioning. However, during final stent deployment, perforation of the distal segment of the SVG with extravasation
three tandem stenoses of 80–90% involving the proximal, mid, and distal segments of the saphenous vein graft (SVG) to the right coronary artery (Figure 1). PCI was performed successfully with deployment of three non-overlapping bare-metal stents without the use of a distal embolization protection device due to lack of sufficient distal space in the SVG for positioning. However, during final stent deployment, perforation of the distal segment of the SVG with extravasation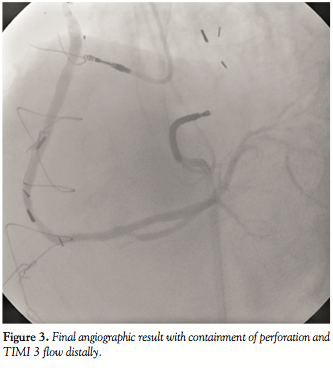 of contrast was noted (Figure 2). The patient remained hemodynamically stable while a 4.0 x 12 mm balloon was inserted for two prolonged inflations proximal to the site of the perforation in an effort to curb the leak. Meanwhile, anticoagulation was reversed with intravenous protamine, but the patient started clinically deteriorating, becoming hypotensive and hypoxic, requiring supplemental oxygen via face mask, intravenous neosynephrine and saline resuscitation for blood pressure support.
of contrast was noted (Figure 2). The patient remained hemodynamically stable while a 4.0 x 12 mm balloon was inserted for two prolonged inflations proximal to the site of the perforation in an effort to curb the leak. Meanwhile, anticoagulation was reversed with intravenous protamine, but the patient started clinically deteriorating, becoming hypotensive and hypoxic, requiring supplemental oxygen via face mask, intravenous neosynephrine and saline resuscitation for blood pressure support. 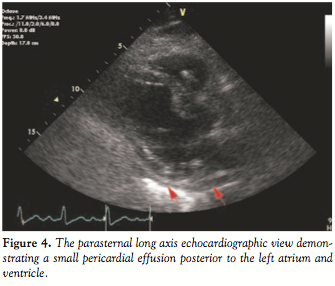 Two overlapping 3.0 x 12 mm Jomed covered stent grafts (Jomed International AB, Helsingborg, Sweden) were deployed over the affected site and subsequent angiography showed TIMI 3 flow with no further extravasation or distal plaque embolization (Figure 3). Bedside echocardiogram revealed a small pericardial effusion posterior to the left atrium and ventricle and no significant fluid around the right ventricle, while the right atrium was not well visualized (Figure 4). Right heart catheterization showed normal right-sided pressures without equalization of diastolic pressures.
Two overlapping 3.0 x 12 mm Jomed covered stent grafts (Jomed International AB, Helsingborg, Sweden) were deployed over the affected site and subsequent angiography showed TIMI 3 flow with no further extravasation or distal plaque embolization (Figure 3). Bedside echocardiogram revealed a small pericardial effusion posterior to the left atrium and ventricle and no significant fluid around the right ventricle, while the right atrium was not well visualized (Figure 4). Right heart catheterization showed normal right-sided pressures without equalization of diastolic pressures.
The patient was transferred to the coronary care unit, where intravenous vasopressors and fluids were weaned off and hemodynamic measurements stabilized. However, he continued to require supplemental oxygen due to hypoxia with pulse oximetry of 85% on 4 liters oxygen by nasal cannula. Physical examination did not reveal signs of fluid overload or congestive heart failure. Repeat echocardiogram demonstrated a large, localized pericardial effusion measuring 8 cm in diameter, surrounding and compressing the right atrium; hypermobile interatrial 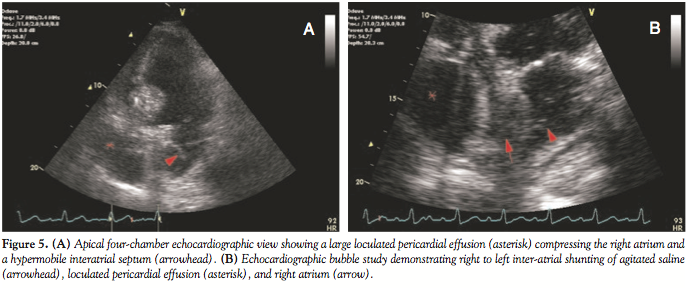 septum; and a right to left shunt through a patent foramen ovale by color flow Doppler and agitated saline injection (Figures 5A and 5B). Repeat angiography confirmed TIMI 3 flow in the SVG and distal right coronary artery with no angiographic evidence of persistent perforation. Serial bedside echocardiograms demonstrated no change in the size of pericardial effusion with persistent right to left inter-atrial shunting of blood. However, since the patient continued to exhibit significant hypoxia requiring
septum; and a right to left shunt through a patent foramen ovale by color flow Doppler and agitated saline injection (Figures 5A and 5B). Repeat angiography confirmed TIMI 3 flow in the SVG and distal right coronary artery with no angiographic evidence of persistent perforation. Serial bedside echocardiograms demonstrated no change in the size of pericardial effusion with persistent right to left inter-atrial shunting of blood. However, since the patient continued to exhibit significant hypoxia requiring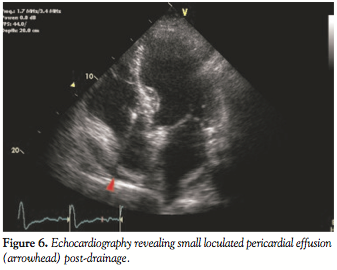 moderate supplemental oxygen, he was ultimately referred for a pericardial window by right-sided video-assisted thoracoscopic surgical approach evacuating approximately 150 ml of blood from the pericardial space and complete resolution of hypoxia. Repeat transthoracic echocardiogram demonstrated minimal pericardial fluid with no visible right to left inter-atrial shunt (Figure 6). The remainder of the patient’s clinical course was uncomplicated and the patient was discharged home on hospital day 14.
moderate supplemental oxygen, he was ultimately referred for a pericardial window by right-sided video-assisted thoracoscopic surgical approach evacuating approximately 150 ml of blood from the pericardial space and complete resolution of hypoxia. Repeat transthoracic echocardiogram demonstrated minimal pericardial fluid with no visible right to left inter-atrial shunt (Figure 6). The remainder of the patient’s clinical course was uncomplicated and the patient was discharged home on hospital day 14.
Discussion. Coronary perforation is a rare but serious complication of PCI, occurring in 0.2–0.3% of coronary interventional procedures.4 The development of a hemodynamically significant pericardial effusion may occur in up to 46% of these patients, and require urgent intervention.5 Prolonged balloon inflation under low pressure can often effectively seal a small perforation; however, when this technique fails, a coronary stent graft can allow successful containment of vessel perforation in the majority of cases.6
CT is a potentially life-threatening syndrome characterized by accumulation of pericardial fluid with hemodynamic compromise.7 Increasing intrapericardial pressure causes slow or rapid compression of all cardiac chambers and as chamber size decreases and myocardial diastolic compliance is reduced, cardiac inflow becomes limited, eventually leading to equalization of mean pericardial and intracardiac diastolic pressures resulting in low cardiac output.8
Regional CT is an infrequent occurrence most often seen after pericardiotomy. The subsequent development of pericardial adhesions in the setting of effusion increases the likelihood of regional CT. It has also been rarely reported in PCI complicated by coronary perforation.9–11 The characteristic clinical and echocardiographic signs of CT may not be apparent due to selective chamber compression.3,9 Isolated acute hypoxia with right to left shunting of blood through a patent foramen ovale is rarely reported in CT. Contributing factors include positive pressure ventilation, positive end expiratory pressure support, changes in right ventricular compliance, and altered right atrial geometry, which may cause distortion of the interatrial septum resulting in right to left shunting of blood.12 Saunders et al describe the only published case of post-coronary artery bypass graft surgery from compression of the main pulmonary artery by extravascular thrombus resulting in acute hypoxia by right to left shunting of blood through a patent foramen ovale, where urgent surgical exploration and evacuation of clot was performed with resolution of hypoxia.1 Treatment of CT from coronary perforation is aimed at relieving external compression by drainage of pericardial fluid, and often involves open thoracotomy if percutaneous pericardiocentesis and containment of perforation is not feasible.
We describe a unique case of an SVG perforation sustained during PCI, with ensuing large loculated pericardial effusion compressing the right atrium and alteration of interatrial septum and right atrial geometry, causing right to left shunting of blood through a patent foramen ovale, resulting in significant hypoxia, and relieved after a pericardial window and evacuation of effusion. Although rare, a high clinical suspicion for localized pericardial effusion is critical in select patients, specifically post-pericardiotomy, with persistent hypoxia despite hemodynamic stability. Hypoxia may be an isolated finding depending on the location of the effusion and early identification is necessary for favorable outcomes. Transthoracic or transesophageal echocardiogram should be used to establish the diagnosis followed by therapeutic drainage of the effusion.
References
- Saunders PC, Grau JB, Chen CL, et al. Localized pericardial hematoma presenting with acute hypoxia. Annal Thorac Surg 2005;79:2141–2143.
- Saner HE, Olson JD, Goldenberg IF, et al. Isolated right atrial tamponade after open heart surgery role of echocardiography in diagnosis and management. Cardiology 1995;86:464–472.
- Ionescu A, Wilde P, Karsch KR. Localized pericardial tamponade difficult echocardiographic diagnosis of a rare complication after cardiac surgery. J Am Soc Echocardiogr 2001;14:1220–1223.
- Javaid A, Buch AN, Satler SF, et al. Management and outcomes of coronary artery perforation during percutaneous coronary intervention. Am J Cardiol 2006;98:911–914.
- Gunning MG, Williams IL, Jewitt DE, et al. Coronary artery perforation during percutaneous intervention: Incidence and outcome. Heart 2002;88:495–498.
- Lansky AJ, Yang YM, Khan Y, et al. Treatment of coronary artery perforations complicating percutaneous coronary intervention with a polytetrafluoroethylene-covered stent graft. Am J Cardiol 2006;98:370–374.
- LeWinter MM. Pericardial diseases. In: Braunwald’s Heart Disease, A Textbook of Cardiovascular Medicine, 8th Edition. Libby P, Bonow RO (eds). Saunders Elsevier, Philadelphia, Pennsylvania: pp. 1829–1854.
- Spodick D. Acute cardiac tamponade. New Engl J Med 2003;349:684–690.
- Russo AM, O’Connor WH, Waxman HL. Atypical presentations and echocardiographic findings in patients with cardiac tamponade occurring early and late after cardiac surgery. Chest 1993;104:71–78.
- Crete M, Barbeau G, Bertrand O, Sénéchal M. Tamponade from acute left atrium compression. Circulation 2005;112:E250–E251.
- Kadner A, Chen RH, Collard CD, Adams DH. Isolated left atrial tamponade following circumflex artery angioplasty. Heart 2000;84:514–519.
- Schoevaerdts D, Gonzalez M, Evrard P, et al. Patent foramen ovale: A cause of significant post-coronary artery bypass grafting morbidity. Cardiovasc Surg 2002;10:615–617.
_____________________________
From the Division of Cardiovascular Medicine, Deborah Heart and Lung Center, Browns Mills, New Jersey.
The authors report no conflicts of interest regarding the content herein.
Manuscript submitted July 20, 2010, provisional acceptance given July 27, 2010, final version accepted August 10, 2010.
Address for correspondence: Jon C. George, MD, Director of Clinical Research, Division of Cardiovascular Medicine, Deborah Heart and Lung Center, 200 Trenton Road, Browns Mills, NJ 08015. Email: jcgeorgemd@hotmail.com





