

Real-Time Three-Dimensional Intracardiac Echocardiography: An Early Single-Center Experience
Abstract: As interventional procedures in structural heart diseases are coming of age, there is a significant lag in the periinterventional imaging development for these procedures to become safe, expedient, accurate, and well tolerated by this patient population. Currently, transesophageal echocardiography (TEE), including real-time three-dimensional (RT-3D), has been used for monitoring and guidance for these procedures. Accurate identification of the pathology, its anatomy, and its relationship with the adjoining structures along with spatial resolution is of paramount importance for wire and catheter placement, device deployment, evaluation of the results, and any potential complications. Two-dimensional intracardiac echocardiography (ICE) has been used extensively for a variety of interventional procedures that undergo conscious sedation of monitored anesthesia. RT-3D ICE has recently become available; we describe our initial experience with this new imaging technology.
J INVASIVE CARDIOL 2015;27(1):E5-E12
Key words: cardiac imaging, real-time imaging
________________________________

Echocardiography in its various forms has become the most clinically used diagnostic tool in the field of cardiology. The development of two-dimensional (2D) intracardiac echocardiography (ICE) has added a new dimension to the imaging modalities available to cardiologists1 and over the years has been increasingly used to close secundum atrial septal defects,2 safely perform transseptal punctures,3 and to guide complex ablation procedures.4,5 Although 2D-ICE has impacted our capability for diagnostic imaging and become a part of therapeutic interventional procedures, the concept of three-dimensional (3D) imaging would be envisioned as a natural evolution of this technology. Advantages of currently available ICE transducers include high-quality near-field imaging and the ability to achieve multiple image planes using a steerable quadridirectional catheter with color flow and Doppler capabilities. However, the use of RT-3D ICE has not been previously described.
 The field of percutaneous structural heart disease interventions has blossomed with transcatheter aortic valve implantation (TAVI) approved by the Food and Drug Administration (FDA) for inoperable, high-risk patients,6,7 a multitude of trials evaluating the efficacy of TAVI in the intermediate-risk group of patients, and the FDA approval for prohibitively high-risk patients with mitral regurgitation for transcatheter mitral valve repair with the Mitraclip device.8 It’s also worth mentioning the positive studies on left atrial appendage (LAA) closure with the Watchman device,9,10 and the unmet need for a non-pharmacological option for stroke prophylaxis in patients with atrial fibrillation.
The field of percutaneous structural heart disease interventions has blossomed with transcatheter aortic valve implantation (TAVI) approved by the Food and Drug Administration (FDA) for inoperable, high-risk patients,6,7 a multitude of trials evaluating the efficacy of TAVI in the intermediate-risk group of patients, and the FDA approval for prohibitively high-risk patients with mitral regurgitation for transcatheter mitral valve repair with the Mitraclip device.8 It’s also worth mentioning the positive studies on left atrial appendage (LAA) closure with the Watchman device,9,10 and the unmet need for a non-pharmacological option for stroke prophylaxis in patients with atrial fibrillation.
 More than a half century after its invention, the theoretical and practical limitations of angiography have been confirmed. Echocardiography, including 3D transesophageal echocardiography (TEE) along with real-time (RT) 3D TEE, have become standard of care for these procedures to ensure precise deployment of these devices and prevention of bad outcomes.2,11-13 Because of the discomfort associated with TEE and the need for adequate airway protection in the supine position, the procedure is performed under general anesthesia with endotracheal intubation,14 which adds additional time, complexity, and cost to the procedure.
More than a half century after its invention, the theoretical and practical limitations of angiography have been confirmed. Echocardiography, including 3D transesophageal echocardiography (TEE) along with real-time (RT) 3D TEE, have become standard of care for these procedures to ensure precise deployment of these devices and prevention of bad outcomes.2,11-13 Because of the discomfort associated with TEE and the need for adequate airway protection in the supine position, the procedure is performed under general anesthesia with endotracheal intubation,14 which adds additional time, complexity, and cost to the procedure.
 The recently introduced AcuNav V (Siemens, Inc) represents the only commercially available RT-3D ICE system. This 10 Fr catheter carries a matrix transducer providing a 22° x 90° RT volume image. This technology has been used for a multitude of procedures at our institution and we are therefore describing our early experience with this novel technology.
The recently introduced AcuNav V (Siemens, Inc) represents the only commercially available RT-3D ICE system. This 10 Fr catheter carries a matrix transducer providing a 22° x 90° RT volume image. This technology has been used for a multitude of procedures at our institution and we are therefore describing our early experience with this novel technology.
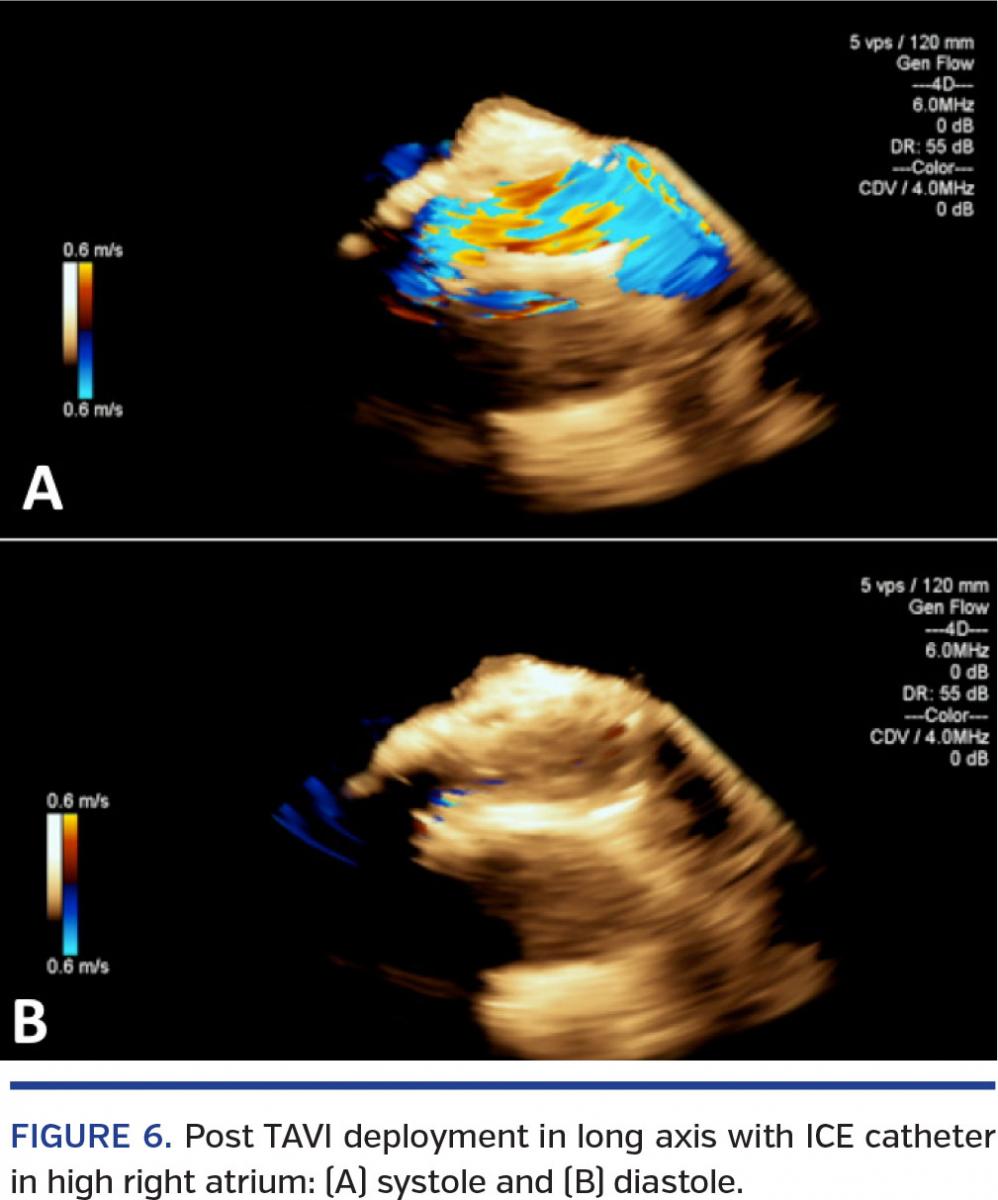
3D-ICE for TAVI (Figures 1-11)

TAVI has become an accepted alternative to surgery for inoperable and high-risk patients with severe symptomatic aortic stenosis.7,15-17 TEE is an important supplement to fluoroscopic imaging for this procedure. Since TEE is performed under general anesthesia, some have proposed a minimalist approach. However, general consensus and practice continue to support the use of TEE guidance.13 RT-3D ICE may be a suitable alternative in this patient population.18-20
 Longitudinal views are obtained from the cavoatrial junction with RT-3D ICE. This view continuously displays the ascending aorta, aortic valve with the non-coronary cusp (NCC), and the left coronary cusps (LCC). Identification of the pigtail in the NCC and visualization of the annular hinge point of the NCC are very important for accurate deployment of the TAVI device. The aortic valve is visualized in short axis from the mid-right ventricle or the right ventricular outflow tract. The calcification and debris on the aortic valve can be easily identified. With further research, the degree of calcification and debris on the valve may lend themselves to a grading classification, which may be able to
Longitudinal views are obtained from the cavoatrial junction with RT-3D ICE. This view continuously displays the ascending aorta, aortic valve with the non-coronary cusp (NCC), and the left coronary cusps (LCC). Identification of the pigtail in the NCC and visualization of the annular hinge point of the NCC are very important for accurate deployment of the TAVI device. The aortic valve is visualized in short axis from the mid-right ventricle or the right ventricular outflow tract. The calcification and debris on the aortic valve can be easily identified. With further research, the degree of calcification and debris on the valve may lend themselves to a grading classification, which may be able to
prognosticate the risk of embolic phenomenon during the TAVI procedure. The RT-3D imaging allows the operator to negotiate the wire across the orifice, thus preventing a blind search for a “needle in a haystack.” The aortic annulus may be measured again prior to choosing the appropriately sized valvuloplasty balloon. The importance of assessing the degree of aortic regurgitation both before and after valvuloplasty cannot be emphasized enough. This can all be accomplished without moving the catheter in the cavoatrial junction.
 Other potential complications that may be easily identified with ICE imaging include examining the right ventricular free wall to evaluate for effusion and tamponade. This is accomplished by flexing the catheter to face the tricuspid valve. The temporary pacemaker (TP) is also visible in this view, and the TP balloon may be assessed for appropriate positioning.
Other potential complications that may be easily identified with ICE imaging include examining the right ventricular free wall to evaluate for effusion and tamponade. This is accomplished by flexing the catheter to face the tricuspid valve. The temporary pacemaker (TP) is also visible in this view, and the TP balloon may be assessed for appropriate positioning.
Assessing left ventricular function and identifying any regional wall-motion abnormalities is critical prior to TAVI. This may be performed with RT-3D ICE very effectively, and may be assessed either from the right ventricle or from the inferior cavoatrial junction in the eventuality of a complication. The ventricular cavity size may also be assessed, including the degree of left ventricular hypertrophy.

The cavity size is critical in planning the procedure, including shaping the wire to fit the cavity well. With the advent of TAVI, the complication of the suicide ventricle has been described after relief of aortic stenosis and profound hypotension not responsive to vasopressors (but rather volume resuscitation and beta-blockers). Evaluating left ventricular cavity size and outflow obstruction may very easily assess this situation.
Wire entrapment in the mitral valvular apparatus results in severe acute mitral regurgitation and hence hypotension. Advancing the catheter into the right ventricular outflow tract to visualize the mitral valve apparatus, and thereby resolving this easily treatable condition if recognized, makes the identification of this complication early enough very important.
 Wire perforation is a catastrophic complication of the TAVI procedure. Real-time assessment may be performed and ensure that the stiff wire is adequately prolapsed in the left ventricular cavity.
Wire perforation is a catastrophic complication of the TAVI procedure. Real-time assessment may be performed and ensure that the stiff wire is adequately prolapsed in the left ventricular cavity.
Appropriate positioning of the TAVI device to the NCC annulus is of extreme importance and may be performed with great precision with either the Sapien or the CoreValve device. Since the deployment of the self-expanding Core-Valve is slower, continued attention to maintaining the position at the annulus without excessive need for angiographic contrast cannot be overemphasized. Appropriate assessment of the valve after deployment is crucial to assess transvalvular and paravalvular regurgitation. Such an assessment may be made in RT with the catheter in the cavoatrial junctions and the right ventricle. Coaptation of the leaflets in 3D views is also easily assessed.
 Assessment of the ascending aorta is very important for preprocedural planning, in order to assess the puncture site for direct aortic access to ensure there is enough purchase length to advance the equipment and deploy the valve safely. Also, it is critical to evaluate dissections post procedure. This may be performed easily by advancing the catheter to the superior vena cava. This view also enables visualization up to the innominate and proximal aortic arch.
Assessment of the ascending aorta is very important for preprocedural planning, in order to assess the puncture site for direct aortic access to ensure there is enough purchase length to advance the equipment and deploy the valve safely. Also, it is critical to evaluate dissections post procedure. This may be performed easily by advancing the catheter to the superior vena cava. This view also enables visualization up to the innominate and proximal aortic arch.
3D-ICE for Transcatheter Mitral Valve Repair (Figures 12-17)

The Mitraclip device8,21 (Abbott Vascular), which was used in an investigational fashion and only recently approved for prohibitively high-risk patients suffering from degenerative mitral regurgitation, has required TEE for guidance.
RT-3D ICE may be used for an appropriately positioned transseptal puncture and safe guidance of the guiding sheath into the left atrium along with guidance of the delivery catheter across the mitral valve. The guidance across the septum may be performed with the catheter in the right atrium. The remainder of the procedure may be performed with the catheter in the mid-right ventricle and the outflow tract. The ICE images allow good visualization of A2 and P2, and therefore grasping the leaflets becomes easy. It is noteworthy that during catheter delivery across the mitral valve and the grasping process, the ICE catheter is not moved physically and the different views are obtained by manipulating the workstation software (including using color Doppler to assess the mitral regurgitation).

Much like TAVI, the Mitraclip procedure may have associated complications that may be assessed with the ICE catheter, including tamponade, residual mitral regurgitation, and left ventricular function.
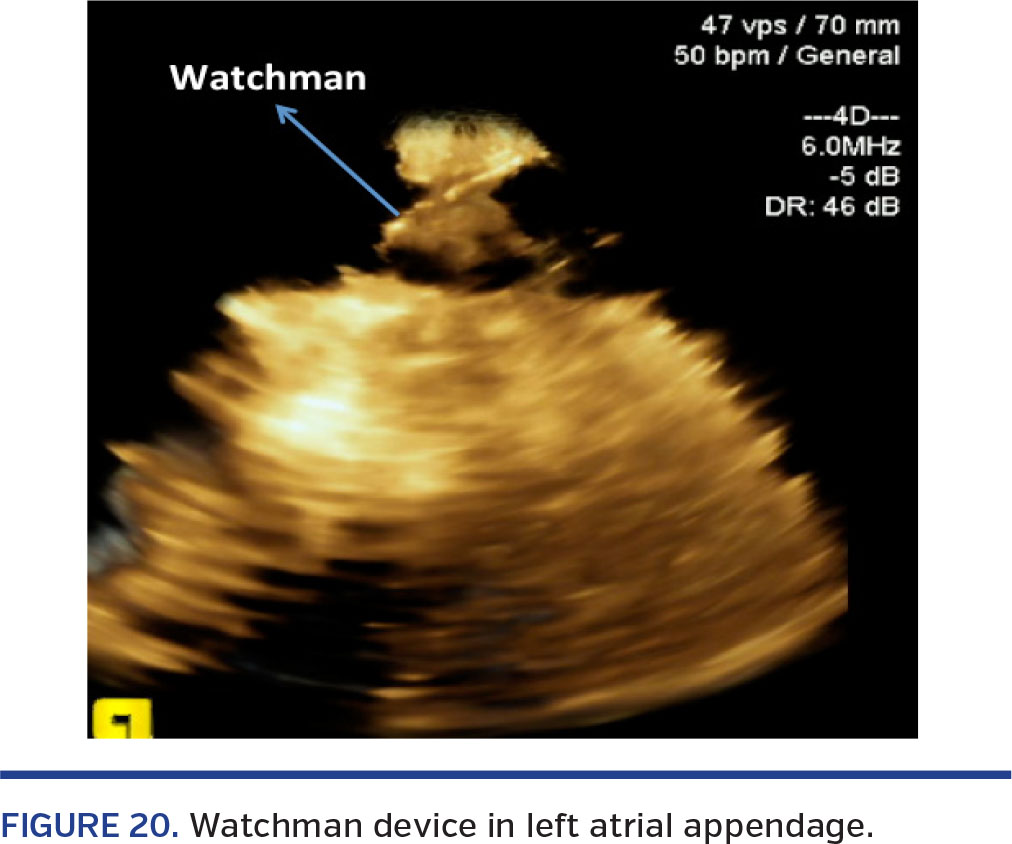
3D-ICE for LAA Closure (Figures 18-20)

LAA closure with the Watchman device9,10 (Boston Scientific) continues to be investigational in the United States. RT-3D ICE may be used as guidance during LAA closure for transseptal puncture and guide the delivery catheter into the LAA using RT-3D imaging. Right atrial views are generally insufficient to assess the anatomy of the LAA, and therefore we have used the right ventricular outflow tract to visualize the LAA.
Thrombi in the LAA may be excluded, the length assessed, and the orifice of the appendage measured including the perimeter. RT deployment, including assessment of leaks, is feasible. The device is deployed after a so-called “tug test” that could be assessed by RT-3D ICE. A study evaluating the correlation of sizing by TEE and RT-3D ICE is underway and undergoing enrollment at our site. As of now, the device is deployed using TEE as well, since the use of TEE is mandated by protocol.

3D-ICE for Atrial Septal Defect Closure (Figure 21)
Secundum atrial septal defects are amenable to device closure and have been closed effectively with the use of 2D ICE for years;2 however, for larger defects, a number of operators like to use TEE (especially RT-3D imaging). We therefore feel that RT-3D ICE may be a very good alternative in this patient population. Assessment of the rim (or lack thereof) is extremely important, especially on the aortic side.

The rim may be assessed very well in RT, as well as distance ascertained from the aorta after the device is deployed but not yet released, making the procedure safer, particularly in large defects.
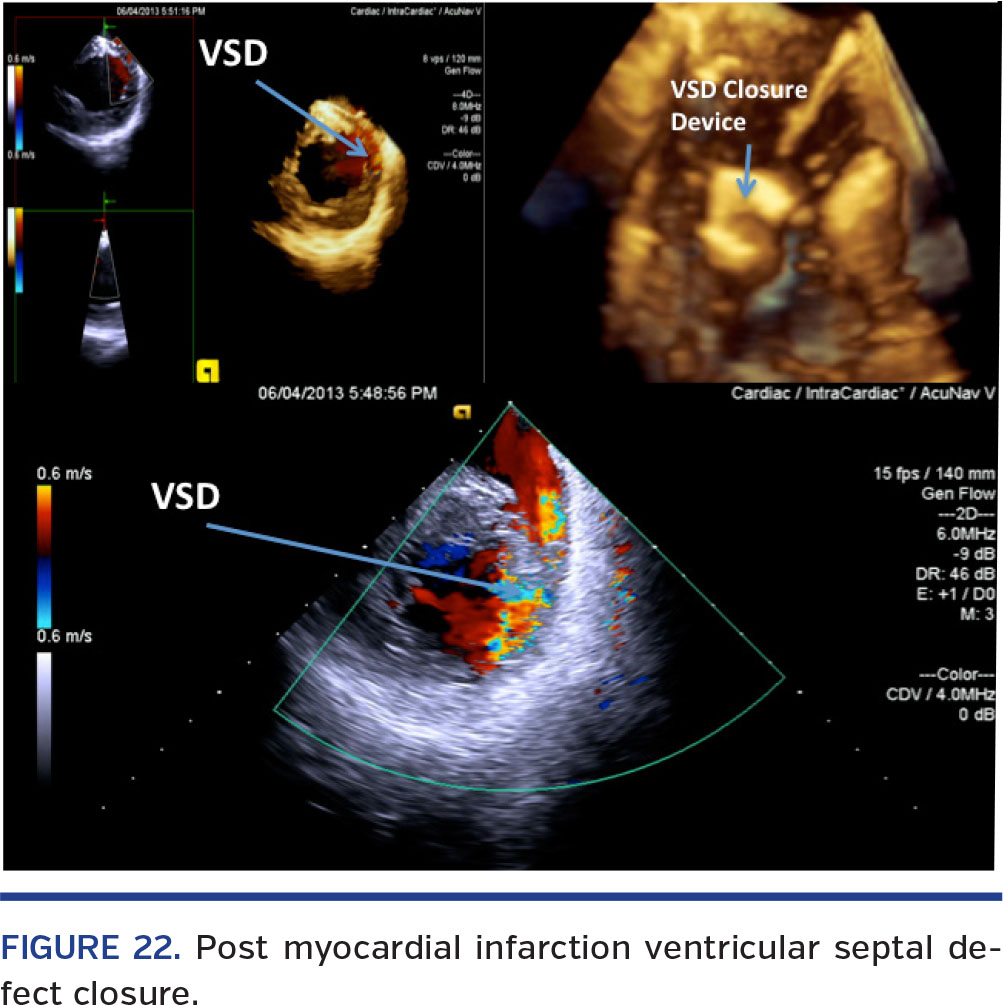
3D-ICE for Ventricular Septal Defect Closure (Figure 22)

ICE has been used for closure of ventricular septal defects. RT-3D ICE may be especially helpful in patients with post myocardial infarction ventricular septal defects. Given the presence of necrotic tissue and multiple rents, visualization with RT-3D ICE may allow easier crossing of the defect and more appropriate device deployment. The catheter placement in this case would be in the inferior cavoatrial junction and in the right ventricle.
Conclusion

RT-3D ICE is a new novel technology that has many potential benefits. As newer devices are coming to market to treat structural heart disease, we cannot continue to rely on age-old fluoroscopy. It behooves us to develop new imaging technology that would be complementary to the advances being made in the device world. Most of the patients offered these new-era devices are high risk, if not inoperable, and we therefore need to try and evaluate options that would allow us to do these procedures without general anesthesia. We feel that RT-3D ICE may be able to provide these sick patients that option.
 Accuracy of deployment of these devices is of paramount importance, and unfortunately fluoroscopy lacks the imaging with which these devices may be deployed. Multimodality imaging and fusion imaging in the future would allow operators the luxury of very accurate placement of these devices and hence result in superior outcomes.
Accuracy of deployment of these devices is of paramount importance, and unfortunately fluoroscopy lacks the imaging with which these devices may be deployed. Multimodality imaging and fusion imaging in the future would allow operators the luxury of very accurate placement of these devices and hence result in superior outcomes.
Less need for angiography may translate into fewer procedure-related renal complications as well as less radiation exposure for both the patient and clinical staff.

In the current economic environment, it is of great importance that we maintain a streamlined workflow and decrease costs incurred with each procedure and have the best outcomes. Our early experience with RT-3D ICE has been promising; however, in its current configuration, it certainly has limitations, including the small volume of 22° x 90°, lack of M-mode, and continuous-wave Doppler. Newer RT-3D ICE catheters are under development and undergoing animal studies, including the development of fusion technology. A more direct comparison with the imaging quality by 3D-TEE imaging is warranted, and we are in the process of doing direct comparison studies between RT-3D ICE and 3D-TEE imaging.
As the era of structural heart device therapies is dawning, the imaging world must catch up and provide us the visual capabilities similar to the 10x loops that the surgeons have used with such finesse over so many decades. RT-3D ICE may just be the useful tool that will help revolutionize further development in this field.
References
 Bruce CJ, Packer DL, Seward JB. Intracardiac Doppler hemodynamics and flow: new vector, phased-array ultrasound-tipped catheter. Am J Cardiol. 1999;83(10):1509-1512, A9.
Bruce CJ, Packer DL, Seward JB. Intracardiac Doppler hemodynamics and flow: new vector, phased-array ultrasound-tipped catheter. Am J Cardiol. 1999;83(10):1509-1512, A9.- Vaidyanathan B, Simpson JM, Kumar RK. Transesophageal echocardiography for device closure of atrial septal defects: case selection, planning, and procedural guidance. JACC Cardiovasc Imag. 2009;2(10):1238-1242.
- Daoud EG, Kalbfleisch SJ, Hummel JD. Intracardiac echocardiography to guide transseptal left heart catheterization for radiofrequency catheter ablation. J Cardiovasc Electrophysiol. 1999;10(3):358-363.
- Hijazi ZM, Shivkumar K, Sahn DJ. Intracardiac echocardiography during interventional and electrophysiological cardiac catheterization. Circulation. 2009;119(4):587-596.
 Epstein LM, Mitchell MA, Smith TW, Haines DE. Comparative study of fluoroscopy and intracardiac echocardiographic guidance for the creation of linear atrial lesions. Circulation. 1998;98(17):1796-1801.
Epstein LM, Mitchell MA, Smith TW, Haines DE. Comparative study of fluoroscopy and intracardiac echocardiographic guidance for the creation of linear atrial lesions. Circulation. 1998;98(17):1796-1801.- Durand E, Borz B, Godin M, et al. Transfemoral aortic valve replacement with the Edwards Sapien and Edwards Sapien XT prosthesis using exclusively local anesthesia and fluoroscopic guidance: feasibility and 30-day outcomes. JACC Cardiovasc Interv. 2012;5(5):461-467. Epub 2012 May 9.
- Smith CR, Leon MB, Mack MJ, et al. Transcatheter versus surgical aortic-valve replacement in high-risk patients. N Engl J Med. 2011;364(23):2187-2198. Epub 2011 Jun 5.
- Feldman T, Foster E, Glower DD, et al. Percutaneous repair or surgery for mitral regurgitation. N Engl J Med. 2011;364(15):1395-1406. Epub 2011 Apr 4.
- Holmes DR, Reddy VY, Turi ZG, et al. Percutaneous closure of the left atrial appendage versus warfarin therapy for prevention of stroke in patients with atrial fibrillation: a randomised non-inferiority trial. Lancet. 2009;374(9689):534-542.
- Nucifora G, Faletra FF, Regoli F, et al. Evaluation of the left atrial appendage with real-time 3-dimensional transesophageal echocardiography: implications for catheter-based left atrial appendage closure. Circ Cardiovasc Imaging. 2011;4(5):514-523.
- Altiok E, Becker M, Hamada S, et al. Real-time 3D TEE allows optimized guidance of percutaneous edge-to-edge repair of the mitral valve. JACC Cardiovasc Imaging. 2010;3(11):1196-1198.
- Berry C, Oukerraj L, Asgar A, et al. Role of transesophageal echocardiography in percutaneous aortic valve replacement with the CoreValve Revalving system. Echocardiography. 2008;25(8):840-848. Epub 2008 May 13.
- Lang RM, Badano LP, Tsang W, et al. EAE/ASE recommendations for image acquisition and display using three-dimensional echocardiography. J Am Soc Echocardiogr. 2012;25(1):3-46.
- Hijazi Z, Wang Z, Cao Q, Koenig P, Waight D, Lang R. Transcatheter closure of atrial septal defects and patent foramen ovale under intracardiac echocardiographic guidance: feasibility and comparison with transesophageal echocardiography. Catheter Cardiovasc Interv. 2001;52(2):194-199.
- Kodali SK, Williams MR, Smith CR, et al. Two-year outcomes after transcatheter or surgical aortic-valve replacement. N Engl J Med. 2012;366(18):1686-1695. Epub 2012 Mar 26.
- Makkar RR, Fontana GP, Jilaihawi H, et al. Transcatheter aortic-valve replacement for inoperable severe aortic stenosis. N Engl J Med. 2012;366(18):1696-1704. Epub 2012 Mar 26.
- Leon MB, Smith CR, Mack M, et al. Transcatheter aortic-valve implantation for aortic stenosis in patients who cannot undergo surgery. N Engl J Med. 2010;363(17):1597-1607.
- Bartel T, Bonaros N, Muller L, et al. Intracardiac echocardiography: a new guiding tool for transcatheter aortic valve replacement. J Am Society Echocardiogr. 2011;24(9):966-975.
- Bartel T, Konorza T, Arjumand J, et al. Intracardiac echocardiography is superior to conventional monitoring for guiding device closure of interatrial communications. Circulation. 2003;107(6):795-797.
- Bartel T, Muller S, Biviano A, Hahn RT. Why is intracardiac echocardiography helpful? Benefits, costs, and how to learn. Eur Heart J. 2014;35(2):69-76. Epub 2013 Oct 21.
- Altiok E, Hamada S, Brehmer K, et al. Analysis of procedural effects of percutaneous edge-to-edge mitral valve repair by 2D and 3D echocardiography. Circ Cardiovasc Imaging. 2012;5:748-755.
______________________________________________________________________
From the Pinnacle Health Cardiovascular Institute, Wormleysburg, Pennsylvania.
Disclosure: The author has completed and returned the ICMJE Form for Disclosure of Potential Conflicts of Interest. Dr Maini reports consultant fees, honoraria, research grants, and other support from Siemens, Abbott Vascular, Medtronic, Boston Scientific, St. Jude Medical, and Abiomed.
Manuscript submitted March 5, 2014, provisional acceptance given May 15, 2014, final version accepted June 13, 2014.
Address for correspondence: Brijeshwar Maini, MD, FACC, 1000 North Front Street, Wormleysburg, PA 17043. Email: bmaini@pinnaclehealth.org







