

Purulent Pericarditis Caused by Haemophilus influenzae Type B
ABSTRACT: Purulent pericarditis, once a common entity associated with intrathoracic infections, such as pneumonia and empyema, has become an infrequent illness in the post-antibiotic era. Prompt recognition and therapy are vital in improving disease-related mortality. Herein, we describe a rare case of Haemophilus influenzae type B purulent pericarditis and associated cardiac tamponade. Antibiotic therapy, pericardial drainage, and subsequent pericardiectomy were performed with resolution of illness.
J INVASIVE CARDIOL 2011;23:E110–E112
______________________________________
Purulent pericarditis (PP) is defined as a localized infection of the pericardial space. In the pre-antibiotic era, PP occurred primarily from a pulmonary focus, but since the introduction of antibiotics, it has become a rare finding limited to patients with direct pericardial injury or immuno-compromised conditions. Herein, we describe a patient diagnosed with a rare case of PP caused by Haemophilus influenzae type B (HiB) that was successfully managed with prompt diagnosis and definitive therapy.
Case Report. A 57-year-old male presented with 10 days of worsening cough and dyspnea. He described the cough as productive of yellow sputum but denied any fevers, chills, chest pain, recent travel, or ill contacts at home. Four years earlier, he was diagnosed with multiple myeloma, requiring two bone marrow transplants — most recent being one year prior, right subclavian port-a-cath placement, and immunosuppression on thalidomide 200 mg daily and pamidronate disodium 90 mg monthly.
On physical examination, he was afebrile (temperature: 36.5 °C), hypotensive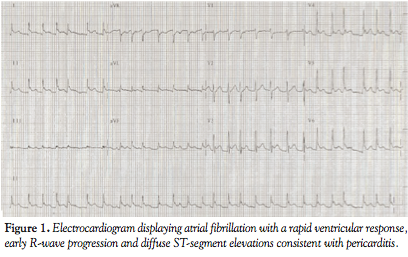 (blood pressure: 95/60 mmHg), tachycardic (pulse irregular at 169 beats/minute), tachypneic (respiratory rate: 38 breaths/minute), and hypoxic (pulse oximetry 98% on 100% oxygen non-rebreather mask). He was in moderate respiratory distress with distended jugular veins at 15 cm of H2O and diminished breath sounds bilaterally. Cardiac exam revealed a tachycardic irregular rate without an audible murmur or rub and a laterally displaced point of maximal impulse.
(blood pressure: 95/60 mmHg), tachycardic (pulse irregular at 169 beats/minute), tachypneic (respiratory rate: 38 breaths/minute), and hypoxic (pulse oximetry 98% on 100% oxygen non-rebreather mask). He was in moderate respiratory distress with distended jugular veins at 15 cm of H2O and diminished breath sounds bilaterally. Cardiac exam revealed a tachycardic irregular rate without an audible murmur or rub and a laterally displaced point of maximal impulse.
Diagnostic testing revealed a white blood cell count of 9,600 with 85%  neutrophils, hematocrit of 40.1%, platelet count of 235,000, blood urea nitrogen of 53 mg/dl, creatinine of 1.1 mg/dl, and albumin of 1.4g/dl. Cardiac biomarkers were negative for myocardial injury. Electrocardiogram displayed new-onset atrial fibrillation with a rapid ventricular response at 163 beats/minute, early R-wave progression and diffuse ST-segment elevations consistent with pericarditis (Figure 1). Chest radiograph demonstrated an enlarged cardiac silhouette with pulmonary venous congestion, a right subclavian port-a-cath, and multiple old healed rib fractures (Figure 2).
neutrophils, hematocrit of 40.1%, platelet count of 235,000, blood urea nitrogen of 53 mg/dl, creatinine of 1.1 mg/dl, and albumin of 1.4g/dl. Cardiac biomarkers were negative for myocardial injury. Electrocardiogram displayed new-onset atrial fibrillation with a rapid ventricular response at 163 beats/minute, early R-wave progression and diffuse ST-segment elevations consistent with pericarditis (Figure 1). Chest radiograph demonstrated an enlarged cardiac silhouette with pulmonary venous congestion, a right subclavian port-a-cath, and multiple old healed rib fractures (Figure 2).
The patient was initiated on intravenous antibiotics with broad-spectrum coverage, fluid resuscitation with normal saline, and intravenous rate control with diltiazem infusion. Computed tomography angiography of the chest 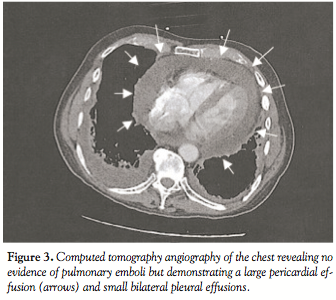 revealed no evidence of pulmonary emboli, but demonstrated a large pericardial effusion and small bilateral pleural effusions (Figure 3). Bedside transthoracic echocardiogram confirmed the presence of a large circumferential pericardial effusion with diastolic collapse of the right ventricle (Figure 4) with marked respiratory variation of mitral and tricuspid inflow velocities, and plethora of the inferior vena cava verifying the clinical diagnosis of cardiac tamponade.
revealed no evidence of pulmonary emboli, but demonstrated a large pericardial effusion and small bilateral pleural effusions (Figure 3). Bedside transthoracic echocardiogram confirmed the presence of a large circumferential pericardial effusion with diastolic collapse of the right ventricle (Figure 4) with marked respiratory variation of mitral and tricuspid inflow velocities, and plethora of the inferior vena cava verifying the clinical diagnosis of cardiac tamponade.
The patient underwent urgent pericardiocentesis, yielding 500 milliliters of thick, ![]() purulent fluid and immediate stabilization of blood pressure and heart rate upon completion of the procedure. Gram stain of the pericardial fluid revealed abundant white blood cells and gram-negative bacilli with final cultures isolating HiB. Cytology, mycobacterial, and fungal studies were unremarkable. Antibiotic coverage was narrowed and blood cultures remained sterile throughout his hospitalization. The patient was ultimately referred for complete pericardiectomy before discharge on hospital day 15.
purulent fluid and immediate stabilization of blood pressure and heart rate upon completion of the procedure. Gram stain of the pericardial fluid revealed abundant white blood cells and gram-negative bacilli with final cultures isolating HiB. Cytology, mycobacterial, and fungal studies were unremarkable. Antibiotic coverage was narrowed and blood cultures remained sterile throughout his hospitalization. The patient was ultimately referred for complete pericardiectomy before discharge on hospital day 15.
Discussion. PP, first described in the 19th century by Galen, has become an uncommon disease in the modern era, due to the widespread use of antibiotics.1 Most reported cases now occur in patients with history of recent thoracic surgery, pre-existing pericardial disease, chest trauma, or in those with an immuno-compromising condition such as chronic renal failure or malignancy.2
Common bacterial pathogens associated with PP include Streptococcus pneumoniae most frequently, Staphylococcus aureus, and gram-negative organisms such as Proteus, Escherichia coli, Pseudomonas, and Klebsiella.3 HiB is an unusual cause of PP: a review of published literature by Garg and colleagues found only 15 reported adult cases of bacterial pericarditis involving HiB.4
Clinical presentation of patients affected by PP can vary, but in a review of 68 cases, fever was present in 88% of patients, dyspnea in 61%, and chest pain in 57%.3 Other frequently noted signs include tachycardia, cough, and fatigue. A pericardial friction rub may be audible in 35–45% of patients.5
Diagnosis of PP begins with a transthoracic echocardiogram to evaluate for the presence of a pericardial effusion followed by drainage and fluid analysis for confirmation. Microscopic analysis, including gram, fungal, and acid-fast stains, in addition to culture and sensitivities allow for isolation of specific pathogens to guide therapy.
Treatment involves prompt initiation of broad-spectrum intravenous antibiotics, with narrowing of therapy once the causal agent is identified. In 42–77% of patients with PP that present with cardiac tamponade,5 diagnostic, and often therapeutic, options for drainage include pericardiocentesis, pericardial window, partial pericardiectomy with pericardial drainage, and total pericardiectomy.6
Late complications of PP include constrictive pericardial disease from thickening and scarring of the pericardium, resulting in a fixed diastolic chamber volume with impaired expansion, and isolation of the cardiac chambers from intrathoracic pressure changes.7 Complete pericardiectomy should always be considered due to the risk of developing constrictive pericarditis in up to 45% of patients.8 In all cases of HiB PP, drainage by pericardiectomy or pericardial window is recommended due to its tendency to cause thick, loculated pus, eventually leading to constrictive pericarditis.6
The prognosis of PP remains poor, primarily due to the lack of prompt recognition and initiation of treatment.5 Bacterial pericarditis carries a high mortality rate of 30–50% despite appropriate therapy, with the majority of deaths due to cardiac tamponade.7
Summary. PP is now an infrequent, yet clinically relevant, disease process. Suspicion should be high in an acutely ill patient with recent thoracic surgery or immune-compromised state. Cardiac tamponade, if present, must be recognized and treated promptly in order to impact survival. Consideration should be given for pericardiectomy to prevent the late complication of constrictive pericarditis. In our patient with a rare case of PP caused by HiB, prompt diagnosis and management as discussed resulted in a favorable outcome.
References
- Siegel RE. Galen on surgery of the pericardium: An early record of therapy based on anatomic and experimental studies. Am J Cardiol 1970;26:524–527.
- Klacsmann PG, Bulkley BH, Hutchins GM. The changed spectrum of purulent pericarditis: An 86 year autopsy experience in 200 patients. Am J Med 1977;63:666–673.
- Hall IP. Purulent pericarditis. Postgrad Med J 1989;65:444–448.
- Garg P, Gupta R, Szalados JE. Bacterial pericarditis and tamponade due to nonencapsulated Haemophilus influenzae complicating a case of adult community-acquired pneumonia. MedGenMed 2006;8:48.
- Alzand, BSN, Meeder JG, Koster A. Purulent pericarditis, an uncommon entity in modern practice: A case report. Neth Heart J 2006;14:309–311.
- Bhaduri-McIntosh S, Prasad M, Moltedo J, Vazquez M. Purulent pericarditis caused by Group A Streptococcus. Tex Heart Inst J 2006;33:519–522.
- Shiber JR. Purulent pericariditis: Acute infections and chronic complications. Hosp Physician 2008;44:9–17; 45.
- Greenberg D, Siefkin AD, Velji MA, Hoeprich PD. Pericarditis caused by beta-lactamase-producing Haemophilus influenzae: Report of two cases in adults and review of the literature. Tex Heart Inst J 1986;13:297–303.
__________________________
From the Deborah Heart and Lung Center, Browns Mills, New Jersey.
The authors report no conflicts of interest regarding the content herein.
Manuscript submitted September 13, 2010 and accepted September 21, 2010.
Address for correspondence: Dr. Jon C. George, MD, Deborah Heart and Lung Center, Interventional Cardiology and Endovascular Medicine, 200 Trenton Road, Browns Mills, NJ 08015. Email: jcgeorgemd@hotmail.com





