

Physical Exertion at High Altitude — Another Risk Factor for Coronary Stent Thrombosis?
Download a PDF of this article.
ABSTRACT: We report 2 cases of very late stent thrombosis (VLST) in patients previously treated with drug-eluting stent (DES). In both cases, VLST occurred during intense physical activities at high altitudes. Exposure to high altitudes alters the coagulation cascade, platelet morphology, and function, resulting in a hypercoagulable state. In addition, strenuous exercise provokes a procoagulant state along with increasing the risk of endothelial damage through the effects on coronary blood flow. In light of these cases, we hypothesize that individuals who are involved in intense physical activities at high altitudes may be at increased risk of stent thrombosis. Use of DES in such patients should be carefully considered.
J INVASIVE CARDIOL 2013;25(4):E66-E68
Key words: stent thrombosis, high altitude, drug-eluting stent, physical exertion
__________________________________________
Drug-eluting stents (DESs) have galvanized coronary intervention with significantly lower rates of restenosis in comparison to bare-metal stents (BMSs) and are currently the first choice of stents in most cases of coronary intervention. However, a steady trickle of reports and publications on very late stent thrombosis (VLST) have questioned their long-term safety. The factors responsible for VLST are less well understood. We encountered two cases of VLST that occurred in unique situations (described below). We have drawn evidences from the literature and propose a hypothesis that poses another risk factor for VLST.
Case 1
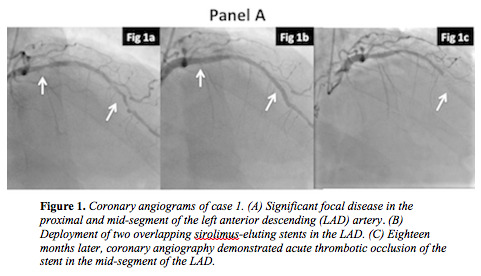 A 58-year-old man underwent coronary angiography for stable angina in 2008, and was found to have significant focal disease in the proximal and mid-segment of the left anterior descending artery (LAD) (Figure 1A). The left circumflex artery was chronically occluded with excellent collaterals from the right coronary artery, which itself had only mild plaque disease. The patient was not keen for surgical revascularization and hence was treated by percutaneous coronary intervention (PCI). He underwent deployment of two overlapping sirolimus-eluting stents in the LAD without any complications (Figure 1B). There was resolution of his symptoms following PCI and he was subsequently discharged after follow-up exam. He completed 1 year of dual-antiplatelet therapy (aspirin 75 mg once daily and clopidogrel 75 mg once daily) and continued on life-long aspirin 75 mg once daily. Eighteen months after stent implantation, he developed sudden onset of chest pain while involved in cross-country skiing in Vail, Colorado in the United States at an altitude of 3000 meters. Further assessment at a local hospital led to a diagnosis of anterior ST-segment elevation myocardial infarction. Coronary angiography demonstrated acute thrombotic occlusion of the stent in the mid-segment of LAD (Figure 1C). His symptoms had settled at the time of coronary angiography with resolution of electrocardiographic (ECG) changes. In view of this, he was managed conservatively, and was repatriated to the United Kingdom. Six weeks later, he had viability assessment of the anterior wall, which was not only viable but also demonstrated significant inducible ischemia. Given his coronary anatomy, he underwent uncomplicated coronary bypass grafting after discussion with the surgeons and is doing well.
A 58-year-old man underwent coronary angiography for stable angina in 2008, and was found to have significant focal disease in the proximal and mid-segment of the left anterior descending artery (LAD) (Figure 1A). The left circumflex artery was chronically occluded with excellent collaterals from the right coronary artery, which itself had only mild plaque disease. The patient was not keen for surgical revascularization and hence was treated by percutaneous coronary intervention (PCI). He underwent deployment of two overlapping sirolimus-eluting stents in the LAD without any complications (Figure 1B). There was resolution of his symptoms following PCI and he was subsequently discharged after follow-up exam. He completed 1 year of dual-antiplatelet therapy (aspirin 75 mg once daily and clopidogrel 75 mg once daily) and continued on life-long aspirin 75 mg once daily. Eighteen months after stent implantation, he developed sudden onset of chest pain while involved in cross-country skiing in Vail, Colorado in the United States at an altitude of 3000 meters. Further assessment at a local hospital led to a diagnosis of anterior ST-segment elevation myocardial infarction. Coronary angiography demonstrated acute thrombotic occlusion of the stent in the mid-segment of LAD (Figure 1C). His symptoms had settled at the time of coronary angiography with resolution of electrocardiographic (ECG) changes. In view of this, he was managed conservatively, and was repatriated to the United Kingdom. Six weeks later, he had viability assessment of the anterior wall, which was not only viable but also demonstrated significant inducible ischemia. Given his coronary anatomy, he underwent uncomplicated coronary bypass grafting after discussion with the surgeons and is doing well.
Case 2
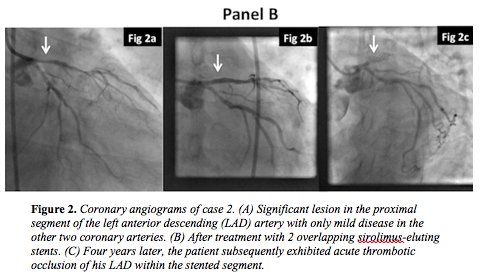 A 75-year-old man was investigated for angina in 2006. Coronary angiography demonstrated a significant lesion in the proximal segment of the LAD with only mild disease in the other two coronary arteries (Figure 2A). The LAD disease was successfully treated with 2 overlapping sirolimus-eluting stents (Figure 2B). He was prescribed dual-antiplatelet therapy for 12 months (aspirin 75 mg once daily and clopidogrel 75 mg once daily) and was advised to continue life-long aspirin (75 mg once daily). Four years after stent implantation, he developed acute onset of severe chest pain while hill walking in Ben Nevis in the Highlands of Scotland at an altitude of 1300 meters. He was transferred to a local cardiology unit via air ambulance and his initial ECG exhibited anterior ST-segment elevation myocardial infarction. Coronary angiography subsequently exhibited acute thrombotic occlusion of his LAD within the stented segment (Figure 2C). The occlusion was treated by deployment of 2 further DESs and he made an uneventful recovery. He now remains on life-long clopidogrel and aspirin.
A 75-year-old man was investigated for angina in 2006. Coronary angiography demonstrated a significant lesion in the proximal segment of the LAD with only mild disease in the other two coronary arteries (Figure 2A). The LAD disease was successfully treated with 2 overlapping sirolimus-eluting stents (Figure 2B). He was prescribed dual-antiplatelet therapy for 12 months (aspirin 75 mg once daily and clopidogrel 75 mg once daily) and was advised to continue life-long aspirin (75 mg once daily). Four years after stent implantation, he developed acute onset of severe chest pain while hill walking in Ben Nevis in the Highlands of Scotland at an altitude of 1300 meters. He was transferred to a local cardiology unit via air ambulance and his initial ECG exhibited anterior ST-segment elevation myocardial infarction. Coronary angiography subsequently exhibited acute thrombotic occlusion of his LAD within the stented segment (Figure 2C). The occlusion was treated by deployment of 2 further DESs and he made an uneventful recovery. He now remains on life-long clopidogrel and aspirin.
Discussion
The use of DESs in PCI has risen exponentially in the last decade. Stent thrombosis is an uncommon but serious complication that often presents as myocardial infarction (usually with ST-segment elevation) and/or death.1,2
Acute stent thrombosis is usually related to procedural problems, such as incomplete stent expansion, presence of dissection, or thrombus. Subacute and late stent thrombosis are often due to premature cessation of antiplatelet therapy.2 Although the risk factors for VLST are not well defined, it is attributed to delayed neointimal coverage, ongoing vessel wall inflammation, and late acquired incomplete stent apposition.3,4 In the setting of delayed neointimal coverage, changes in the coagulation cascade, status of blood cells (platelets and red blood cells), and/or hemodynamics may potentiate the development of stent thrombosis.
Exposure to high altitude has various physiological effects, such as hypoxia, hyperventilation, and tachycardia.5 Thrombosis is a well-recognized complication following exposure to high altitude and has been attributed to alterations in the coagulation cascade, hematocrit values, and platelet count and function.6,7 Two studies have demonstrated significant and sustained elevation of platelet count on ascent to high altitudes.8,9 The mean platelet volume and platelet activities (adhesiveness and aggregation) are shown to be significantly increased at high altitudes.10-15 Furthermore, hypoxic conditions seen at high altitudes can lead to long-term effects on the red blood cells, such as increased cell volumes and hemoglobin levels, and are associated with an increase in the myocardial work load.5 A combination of these factors probably increases the risk of coronary thrombosis and myocardial infarction at high altitudes.
It is a well-known factor that myocardial infarction can be triggered by heavy or intense physical exertion.16,17 This is due to a combination of various factors, such as increased activity of platelets and coagulation factors.18-24 Kestin et al demonstrated transient platelet activation, platelet hyperreactivity and increased platelet count with strenuous exercise.19 Another study by Aurigemma demonstrated similar effects in patients with known coronary artery disease following exercise.20 Healthy individuals can react to these changes in platelets by acutely increasing their fibrinolytic capacity. However, it is proposed that reduced fibrinolytic potential in patients with ischemic heart may increase the risk of acute ischemic events upon extreme physical exertion.21 Increase in the levels of fibrinogen, factor VIII and von Willebrand factor (vWF) have also been noted following heavy exercise, which may contribute toward the development of thrombosis.22
In our patients, stent thrombosis occurred 1 year after the procedure and more importantly the event was triggered during intense physical exertion at high altitudes.
There are 4 reported cases of stent thrombosis following heavy exercise.22-25 In one of the reports, platelet function studies performed before and after the exercise demonstrated hyperactivity of platelets.22 Interestingly in another report, stent thrombosis was encountered during cross-country skiing, although the authors have not brought any correlations.25 In addition, our patients had overlapping DESs, which may have played a potential contributory role for the generation of stent thrombosis.
Reviewing these evidences along with our cases, we hypothesize that intense physical activities undertaken at high altitudes in patients with semi-endothelialized stents may pose an additional risk for stent thrombosis. The choice of stent type (BMS versus DES) needs to be clearly discussed with patients who have such aspirations (extreme exertion at high altitudes). If DESs are clinically indicated, it may be pragmatic to consider dual-antiplatelet agents for the long term. This may not be an issue with new-generation bio-absorbable scaffolds. However, such stents are not currently used globally and most centers still rely on first- and second-generation DESs, which have an associated risk of VLST.
Limitations
Although we have drawn indirect evidences from the literature on platelet activities at high altitude and during extreme physical exertion, we could not perform platelet functional studies on our patients as they were assessed at different hospitals, which lacked such facilities at the time of event. Due to similar reasons, intravascular ultrasound studies could not be performed to understand the mechanism of stent thrombosis. The availability of these two investigations could have strengthened our case report.
Conclusion
The issue of VLST has questioned the long-term safety of DESs. We reported two cases of VLST that occurred in individuals involved in strenuous activities at high altitudes. Consideration of DESs in individuals with such interests (frequent strenuous physical exertion at high altitudes) must be carefully considered and patients should be involved in decision making.
References
- Lüscher TF, Steffel J, Eberli FR, et al. Drug-eluting stent and coronary thrombosis: biological mechanisms and clinical implications. Circulation. 2007;115(8):1051.
- van Werkum JW, Heestermans AA, Zomer AC, et al. Predictors of coronary stent thrombosis: the Dutch Stent Thrombosis Registry. J Am Coll Cardiol. 2009;53(16):1399.
- Finn AV, Joner M, Nakazawa G, et al. Pathological correlates of late drug-eluting stent thrombosis: strut coverage as a marker of endothelialization. Circulation. 2007;115(18):2435.
- Nakagawa Y. Speculative mechanisms for very late stent thrombosis after drug-eluting stent implantation. Circ J. 2011;75(4):779-780.
- Ramirez G, Bittle PA, Rosen R. et al. High altitude living: genetic and environmental adaptation. Aviat Space Environ Med. 1999;70(1):73-81.
- Al-Huthi MA, Raja'a YA, Al-Noami M, Abdul Rahman AR. Prevalence of coronary risk factors, clinical presentation, and complications in acute coronary syndrome patients living at high vs low altitudes in Yemen. MedGenMed. 2006;8(4):28.
- Presti B, Berthrong M, Sherwin RM. Chronic thrombosis of pulmonary arteries. Hum Pathol. 1990;21(6):601-606.
- Hudson JG, Bowen AL, Navia P, et al. The effect of high altitude on platelet counts, thrombopoietin and erythropoietin levels in young Bolivian airmen visiting the Andes. Int J Biometeorol. 1999;43(2):85-90.
- Simon-Schnass I, Korniszewski L. The influence of vitamin E on rheological parameters in high altitude mountaineers. Int J Vitam Nutr Res. 1990;60(1):26-34.
- Martin JF, Bath PM, Burr ML. Influence of platelet size on outcome after myocardial infarction. Lancet. 1991;338(8780):1409-1411.
- Endler G, Klimesch A, Sunder-Plassmann H, et al. Mean platelet volume is an independent risk factor for myocardial infarction but not for coronary artery disease. Br J Haematol. 2002;117(2):399-404.
- Cay S, Biyikoglu F, Cihan G, Korkmaz S. Mean platelet volume in patients with cardiac syndrome X. J Thromb Thrombolysis. 2005;20(3):175-178.
- Alper AT, Sevimli S, Hasdemir H. Effects of high altitude and sea level on mean platelet volume and platelet count in patients with acute coronary syndrome. J Thromb Thrombolysis. 2009;27(2):130-134.
- Chohan IS. Blood coagulation changes at high altitude. Defence Sci J. 1984;34:361-379.
- Singh I, Chohan IS. Abnormalities of blood coagulation at high altitude. Int J Biometeorol. 1972;16(3):283-297.
- Willich SN, Lewis M, Lowel H et al. Physical exertion as a trigger of acute myocardial infarction. N Engl J Med. 1993;329(23):1684-1690.
- Mittleman MA, Maclure M, Tofler GH, et al. Triggering of acute myocardial infarction by heavy physical exertion. Protection against triggering by regular exertion. Determinants of Myocardial Infarction Onset Study Investigators. N Engl J Med. 1993;329(23):1677-1683.
- Lippi G, Maffulli N. Biological influence of physical exercise on hemostasis. Semin Thromb Hemost. 2009;35(3):269-276.
- Kestin AS, Ellis PA, Barnard MR, et al. Effect of strenuous exercise on platelet activation state and reactivity. Circulation. 1993;88:1502-1511.
- Aurigemma C, Fattorossi A, Sestito A, et al. Relationship between changes in platelet reactivity and changes in platelet receptor expression induced by physical exercise. Thromb Res. 2007;120(6):901-909.
- Yilmaz MB, Saricam E, Biyikoglu SF, et al. Mean platelet volume and exercise stress test. J Thromb Thrombolysis. 2004;17(2):115-120.
- Ormezzano O, Polack B, Vanzetto G, et al. Platelet hyperactivity during exercise leading to iterative coronary stent thrombosis: clinical implications. J Thromb Thrombolysis. 2010;30(1):105-108.
- Dash H. Delayed coronary occlusion after successful percutaneous transluminal coronary angioplasty: association with exercise testing. Am J Cardiol. 1983;52(8):1143-1144.
- Simsek Z, Arslan S, Gundogdu F. Late stent thrombosis associated with heavy exercise. Tex Heart Inst J. 2009;36(2):154-157.
- Jamshidi P, Toggweiler S, Erne P. In-stent restenosis and thrombosis 41 months after drug-eluting stent implantation. Int J Cardiol. 2008;130(3):e111-e113.
__________________________________________
From the 1Papworth Hospital, Cambridge, United Kingdom and 2Imperial College, London, United Kingdom.
Disclosure: The authors have completed and returned the ICMJE Form for Disclosure of Potential Conflicts of Interest. The authors report no conflicts of interest regarding the content herein.
Manuscript submitted August 15, 2012, provisional acceptance given September 12, 2012, final version accepted October 17, 2012.
Address for correspondence: Dr Sandeep Basavarajaiah, Department of Interventional Cardiology, Imperial College, Du Cane Road,€London, United Kingdom W12 0HS. Email: sandeep270478@gmail.com





