

Percutaneous Coronary Intervention of Coronary Chronic Total Occlusions Improves Peak Oxygen Uptake During Cardiopulmonary Exercise Testing
Abstract: Objectives. Although coronary chronic total occlusions (CTOs) are treated with percutaneous coronary intervention (PCI) to improve symptoms, studies demonstrating symptom improvement have been mostly limited to questionnaire responses. The current study assessed for changes in peak oxygen uptake (V̇O2) during cardiopulmonary exercise testing after CTO-PCI. Methods. Patients with heart failure or angina symptoms referred for CTO-PCI were prospectively enrolled. The primary outcome of the study was improvement in peak V̇O2 during cardiopulmonary exercise (CPX) testing 5 months after CTO-PCI. Secondary outcomes included improvement in physical capacity, angina, and self perception of health as assessed by questionnaires, and in plasma brain natriuretic peptide (BNP) levels. Results. CTO-PCI was attempted in 32 men (mean age, 62 ± 6 years; CTO vessel: 47% right coronary, 44% left anterior descending). CTO-PCI was unsuccessful in 1 patient, and 3 patients had restenosis of their CTO vessel at follow-up. In the 28 patients with patent CTO vessel at follow-up, significant improvements were noted in self-reported physical capacity, angina, and several aspects of health perception. In the 25 patients who underwent baseline and follow-up CPX testing, peak V̇O2 significantly improved from 17.7 ± 4.3 mL/kg/min to 19.1 ± 4.0 mL/kg/min (P=.02). Plasma BNP levels significantly decreased from 143 ± 138 pg/mL to 102 ± 123 pg/mL (P=.01). Conclusions. CTO-PCI in symptomatic patients was associated with improvements in cardiovascular exercise capacity, as assessed by peak V̇O2. These results suggest that in symptomatic patients with CTOs, PCI appears clinically beneficial.
J INVASIVE CARDIOL 2017;29(3):83-91
Key words: chronic total occlusion, percutaneous coronary intervention, exercise stress testing, symptoms
Coronary chronic total occlusions (CTOs) are highly prevalent in patients with suspected coronary artery disease referred for coronary angiography.1,2 Despite the high prevalence of CTOs, percutaneous coronary intervention (PCI) has traditionally been attempted in only a small fraction of cases due to the associated technical and procedural difficulty.3,4 Recently, novel techniques and specialized equipment have enhanced procedural success, and current guidelines recommend coronary CTO-PCI “in patients with appropriate clinical indications and suitable anatomy, when performed by operators with appropriate expertise.”5,6 To date, evidence for patient symptom improvement has been mainly derived through use of questionnaires, such as the Seattle Angina Questionnaire (SAQ) or SF-36.7-9 With the exception of one study that assessed improvement in 6-minute walk test, objective measures of improvement in exercise capacity are lacking.10
We performed a prospective study to determine whether CTO-PCI results in improvement of peak oxygen uptake (V̇O2) measured during cardiopulmonary exercise (CPX) testing in patients presenting with angina or congestive heart failure symptoms. Improvements in patients’ angina, exercise capacity, and self perception of health were evaluated by questionnaires.
Methods
Study patients. Patients with symptoms of angina or congestive heart failure who were clinically referred for CTO-PCI at the North Texas VA Medical Center between September 2013 and January 2016 were prospectively enrolled in the study. Patients were eligible for the study if they were >18 years, able to provide informed consent, referred to the cardiac catheterization laboratory for PCI of a CTO of an epicardial coronary artery, and had at least New York Heart Association (NYHA) class II or higher heart failure or Canadian Cardiovascular Society (CCS) class II or higher angina symptoms. Coronary CTOs were defined as coronary lesions with Thrombolysis in Myocardial Infarction (TIMI) flow grade 0 for a duration of at least 3 months. CTO-PCI technical success was defined at <30% residual diameter stenosis within the treated segment and restoration of Thrombolysis in Myocardial Infarction (TIMI) 3 antegrade flow. Patients with life expectancy of <1 year or those who had a myocardial infarction <1 month prior to CTO-PCI were excluded. Baseline visits were performed within 1 month prior to the planned CTO-PCI. History of angina and congestive heart failure symptoms were obtained by a study physician at baseline and at follow-up visits.
Thirty-two men were enrolled in the study. CTO-PCI was not successful in 1 patient and 3 patients were found to have restenosis of the CTO vessel on subsequent clinically indicated coronary angiography, resulting in 28 patients with successful CTO-PCI and clinically patent CTO target vessel at follow-up (Figure 1). Of the 28 patients, 2 could not undergo adequate CPX testing at follow-up due to musculoskeletal/orthopedic limitations and in 1 patient the CPX test at follow-up was discontinued by study staff due to the development of atrial fibrillation and heart rate nearing the therapy zone of his implantable cardioverter defibrillator, yielding 25 patients with adequate baseline and follow-up CPX tests. Of the 4 patients with unsuccessful PCI or restenosis, 1 patient was not able to undergo CPX testing due to tracheostomy and 1 patient refused to undergo repeat CPX testing, yielding 2 patients with persistent CTO vessel who underwent baseline and follow-up CPX testing.

The study protocol was approved by the Institutional Review Board and all patients provided written informed consent.
Outcomes. The primary outcome of the study was improvement of peak V̇O2, as assessed by cardiopulmonary exercise testing at follow-up exam. Secondary outcomes included improvement in exercise capacity, angina, and perception of self health, as assessed by questionnaires. Additional outcomes included improvement in NYHA heart failure class, CCS angina class, and brain natriuretic peptide levels.
Cardiopulmonary exercise testing. Participants performed a progressive exercise test to exhaustion on a motorized treadmill. In order to individualize the protocol for each subject, the test was conducted in two parts. Part one of the test was to familiarize the subject with walking on the treadmill and to determine the pace for the subject’s test. After a baseline electrocardiogram and blood pressure, the subject started at a speed of 1.5 mph and 0% grade. Treadmill speed was gradually increased until the participant could walk briskly with a comfortable stride, with emphasis to swing arms as normal and not grab the hand rail. A cardiologist with training in exercise physiology and experience of over 800 CPX tests ran the protocol. The goal was to set a speed that when combined with increases in incline, would reach a max V̇O2 within 8-12 minutes of exercise. Once an appropriate speed was reached, and the subject verbalized an ability to walk at this speed for 15-20 minutes on flat ground, the treadmill speed was recorded, and the participant continued to walk at this speed for 2-3 minutes. The treadmill was then stopped and the subject was allowed to rest for a 5-10 minute period.
The second part of the protocol was the determination of peak V̇O2. Subjects used a nose clip and a mouthpiece connected to a TrueOne Cardiopulmonary Exercise System (Parvomedics) for breath-by-breath measurement of ventilatory and gas-exchange variables.
This system uses gas analyzers to measure oxygen and carbon dioxide levels in exhaled air and a pneumotach to measure air flow. The system was calibrated against known gas concentrations and volumes prior to each test. The protocol for the determination of peak V̇O2 consisted of a fixed speed, as determined in familiarization, starting from a flat position (0% grade) with an incremental 2% increase in grade every 2 minutes until exhaustion. Exhaustion was defined as an indication by the subject that he was unable to proceed despite encouragement to do so.
Blood pressure was measured and recorded during the second minute of each stage. Heart rate and rate of perceived exertion (RPE) were recorded during the final 15 seconds of each 2-minute stage. Maximal heart rate and RPE were defined as the highest values observed during the exercise test. Breath-by-breath gas-exchange variables (oxygen uptake [V̇O2], respiratory exchange ratio [RER], and the ratio of ventilatory exchange/carbon dioxide uptake [V̇E/V̇O2]) were averaged over running 30-second intervals, with peak values for each of the gas-exchange variables taken during the last minute of exercise. Estimated V̇O2 from treadmill speed and incline grade was calculated from the American College of Sports Medicine’s published guidelines using the equation V̇O2 (mL/kg/min) = [0.1 • speed (m/min)] + [1.8 • speed (m/min) • grade of incline (%)] + 3.5 mL/kg/min, and Metabolic Equivalents of Task (MET) was calculated using the equation METs = V̇O2 (mL/kg/min)/3.5.11
On follow-up cardiopulmonary exercise testing, the same speed was chosen as the baseline cardiopulmonary exercise test. On follow-up exam, the patient and study investigator responsible for conducting the test were blinded to the performance during the baseline CPX test.
Questionnaires. Participants were administered the following questionnaires during the baseline and follow-up visits.
Duke Activity Status Index (DASI). The DASI is a well-validated instrument to measure functional capacity and quality of life and has been demonstrated to correlate with peak oxygen uptake.12 The DASI is easy to administer, consists of 12 items, and has been used in multiple observational studies and large clinical trials to assess the effects of coronary intervention in patients with CAD.13-17 It is estimated that an improvement in 3 points of the 52.8 DASI scale is associated with a “clinically meaningful” change in functional status.13,15
Seattle Angina Questionnaire (SAQ). The SAQ is a validated tool assessing five clinical aspects of coronary artery disease: physical limitation, anginal stability, anginal frequency, treatment satisfaction, and disease perception.18 Similar to the DASI, it has been used to evaluate the effect of intervention on symptoms related to coronary disease in numerous studies and large clinical trials,19-21 and has been used to evaluate symptom improvement after PCI of CTO.8
SF-36. The SF-36 is a 36-question survey that is used to monitor the patients’ perceptions of pain and disease burden.22 The SF-36 has previously been used as a survey for study patients in multiple disease states, including coronary atherosclerosis.10,14,16
BNP assay. Blood was collected at baseline and follow-up visits in tubes containing ethylenediaminetetraacetic acid. Assays for BNP were performed using the Alere Triage BNP assay. The lower detection limit of the assay is 1 pg/mL and the upper limit is 5000 pg/mL. The intra- and inter-assay variation coefficients were below 3.1% and 6.6%, respectively.
Statistical analysis. Continuous variables are presented as mean and standard deviation and categorical variables as percentages. Improvements in outcome measures were assessed using paired t-tests and a 2-sided P-value <.05 was considered statistically significant. Patient baseline and follow-up NYHA and CCS classes were denoted as zero if congestive heart failure or angina symptoms, respectively, were absent. In order to determine which clinical and angiographic variables were associated with significant improvements in peak V̇O2, (≥1 mL/kg/min vs <1 mL/kg/min), categorical and continuous variables were compared using Fisher’s exact test and Wilcoxon rank sum test, respectively.
Results
Baseline characteristics. The patients’ baseline clinical characteristics are listed in Table 1. The mean age was 62 ± 6 years, all patients were men, and most were Caucasian, with frequent histories of prior coronary artery bypass surgery (28%) and myocardial infarction (69%). They were also highly symptomatic, with 75% CCS class II or higher and 94% NYHA class II or higher symptoms. All patients were on aspirin, 94% were on beta-blockers, 53% were on long-acting nitrates, 22% were on calcium-channel blockers, and 13% were on ranolazine.

The angiographic characteristics of the study CTOs are presented in Table 2. The right coronary artery was the CTO vessel in 47% and the left anterior descending artery was the CTO vessel in 44%. After CTO-PCI, all patients were offered and encouraged to enroll in a cardiac rehabilitation program; however, only 6 patients completed the program.

Changes in symptoms. Median follow-up was 4.9 months (interquartile range, 3.9-5.9 months). In the 28 patients without known occlusion of their CTO vessel at follow-up, angina improved from a mean CCS class of 1.8 at baseline to 0.6 at follow-up (P<.001) (Figure 2). Similarly, congestive heart failure symptoms improved from a mean NYHA class of 2.2 to 1.4 (P<.001) (Figure 3). Four patients with occluded CTO vessel did not have a change in CCS or NYHA classification (Figures 2 and 3).

In the 28 patients with clinically patent CTO vessel at follow-up, a significant improvement was noted in DASI score, from a mean of 29.2 ± 13.7 at baseline to 37.5 ± 13.9 at follow-up (P<.01) (Table 3). Improvements were also noted in all domains of the SAQ (P<.05 for all) (Table 3). Statistically significant improvements were seen in SF-36 domains of Physical Functioning, Role Limitation due to Physical Health, Role Limitation due to Emotional Problems, Energy/Fatigue, Social Functioning, and Pain domains (P<.05 for all) (Table 3). No significant improvement was noted in the SF-36 domains of Emotional Well Being and General Health.

Cardiopulmonary exercise test results. In the 25 patients without known CTO occlusion at follow-up who underwent CPX testing, a significant improvement was noted in the primary outcome of peak V̇O2 adjusted for weight, increasing from a mean of 17.7 ± 4.3 mL/kg/min at baseline to 19.1 ± 4.0 mL/kg/min at follow-up (P=.02) (Figure 4). Significant improvements were also noted in peak V̇O2 (in L/min), improving from 1.70 ± 0.37 L/min at baseline to 1.85 ± 0.42 L/min at follow-up (P=.01), and in METS calculated from treadmill speed and incline, improving from 5.7 ± 2.0 to 6.4 ± 1.9 (P=.01) (Table 4). At baseline, chest pain was the reason given for limiting the test by 7 patients, while at follow-up only 1 patient stopped exercise due to chest pain. Peak V̇O2 did not increase in either of the 2 patients with known reoccluded CTO at follow-up (Figure 4). Although mean peak V̇O2 increased among the 25 patients without CTO reocclusion, clinically significant improvement (≥1 mL/kg/min) was observed in 16 patients. In order to evaluate whether improvement in peak V̇O2 was associated with any clinical or angiographic factors, univariable analysis was performed for significant improvement in peak V̇O2 (Table 5). However, no clinical factors were significantly associated with significant improvement in peak V̇O2.



 BNP. Mean BNP decreased from baseline to follow-up among the 28 patients without known occluded CTO (143 ± 138 pg/mL to 102 ± 123 pg/mL; P=.01) (Figure 5). Among the 4 patients with an occluded CTO vessel at follow-up, mean BNP did not decrease.
BNP. Mean BNP decreased from baseline to follow-up among the 28 patients without known occluded CTO (143 ± 138 pg/mL to 102 ± 123 pg/mL; P=.01) (Figure 5). Among the 4 patients with an occluded CTO vessel at follow-up, mean BNP did not decrease.
Discussion
The current study is the first to demonstrate a significant improvement in exercise capacity, as assessed by peak V̇O2, among patients who underwent successful CTO-PCI and did not develop 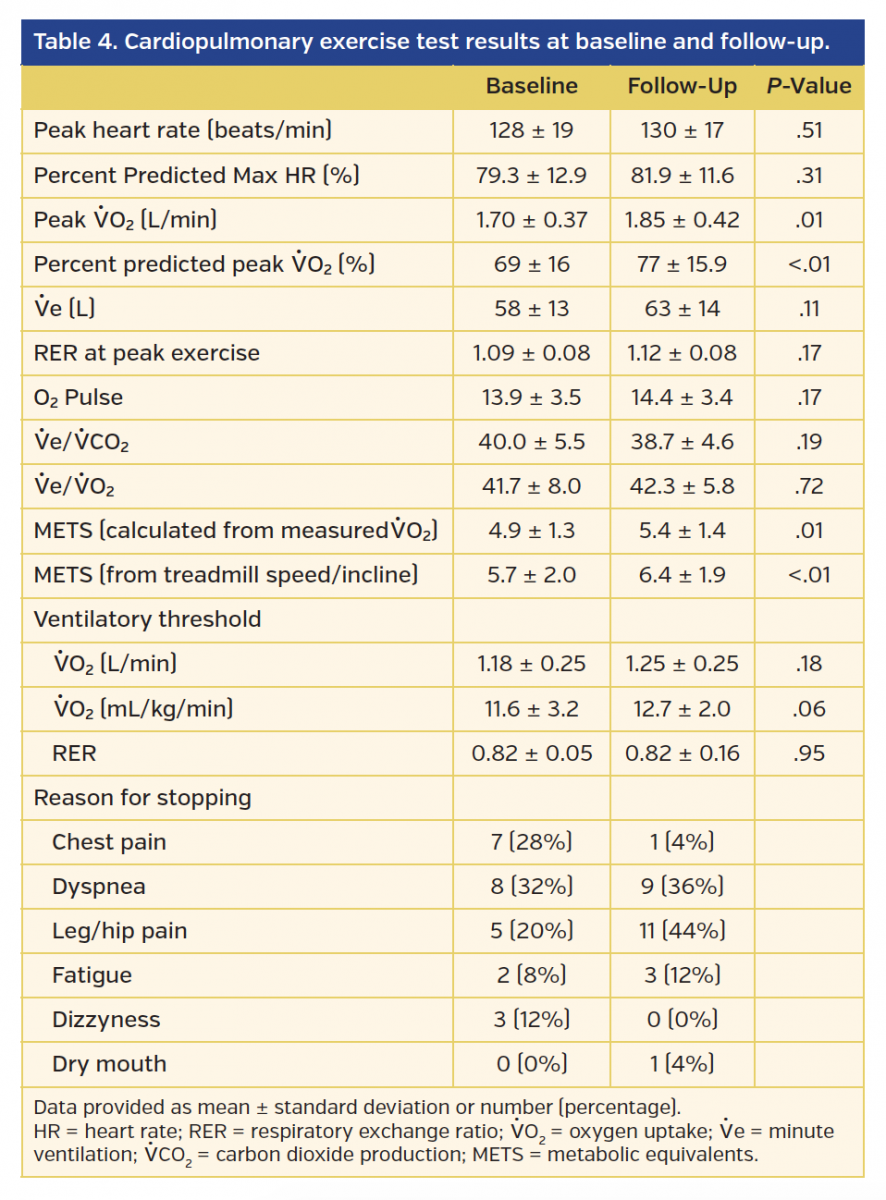 restenosis of the CTO target vessel. This study also demonstrates significant improvement in plasma BNP levels, as well as angina and congestive heart failure symptoms assessed by validated questionnaires.
restenosis of the CTO target vessel. This study also demonstrates significant improvement in plasma BNP levels, as well as angina and congestive heart failure symptoms assessed by validated questionnaires.
Previous studies on the benefits of CTO-PCI. In populations with high burden of atherosclerotic disease risk factors, CTOs have been demonstrated to be present in >25% of patients referred for coronary angiography.1,2 Despite the high prevalence of CTOs and poor associated prognosis,23 it is estimated that revascularization by PCI is attempted in <15% of CTOs.24 This is due to 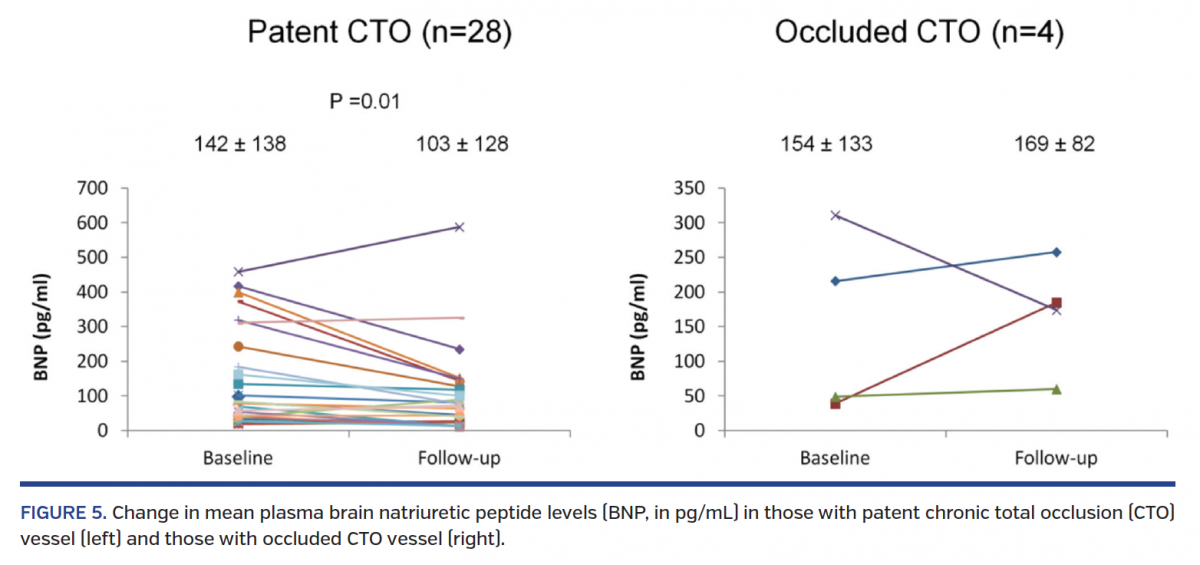 traditionally low success rates at many centers, long procedural times, increased risk for complications, and uncertainty regarding the clinical benefits of CTO-PCI.25,26 While several observational reports have suggested that compared with failed CTO-PCI, successful CTO-PCI may improve survival and left ventricular systolic function,25,27-31 randomized trial data are limited and may not be generalizable to the majority of patients with CTOs.
traditionally low success rates at many centers, long procedural times, increased risk for complications, and uncertainty regarding the clinical benefits of CTO-PCI.25,26 While several observational reports have suggested that compared with failed CTO-PCI, successful CTO-PCI may improve survival and left ventricular systolic function,25,27-31 randomized trial data are limited and may not be generalizable to the majority of patients with CTOs.
In addition, although symptomatic improvement is one of the main reasons for referral to CTO-PCI, data regarding improvement in symptoms in this subgroup of patients are also limited; the majority are derived from improvement in questionnaire parameters. In a substudy of the FlowCardia’s Approach to Chronic Total Occlusion Recanalization (FACTOR) trial, significant improvements were seen in 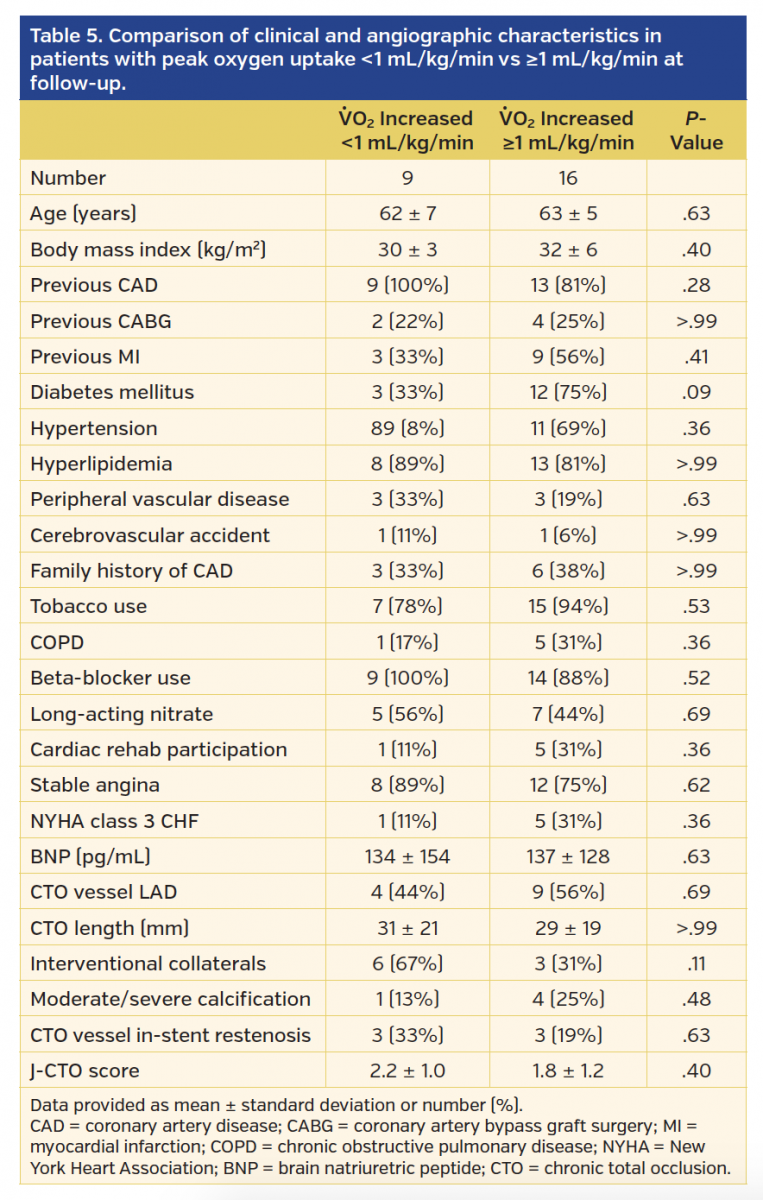 the angina frequency, physical limitation, and quality of life components of the SAQ in 64 of the 125 patients with successful revascularization 1 month post procedure, compared with patients in whom revascularization was not successful.8 Additional observational reports describe continued benefits in patients with longer duration of follow-up in these SAQ components, and also in the treatment satisfaction component.7,9 Rossello et al also recently demonstrated significant improvements in the SF-36 and 6-minute walk test from a mean of 417 m at baseline to 463 m at 6 months post PCI.10
the angina frequency, physical limitation, and quality of life components of the SAQ in 64 of the 125 patients with successful revascularization 1 month post procedure, compared with patients in whom revascularization was not successful.8 Additional observational reports describe continued benefits in patients with longer duration of follow-up in these SAQ components, and also in the treatment satisfaction component.7,9 Rossello et al also recently demonstrated significant improvements in the SF-36 and 6-minute walk test from a mean of 417 m at baseline to 463 m at 6 months post PCI.10
Improvement in peak V̇O2. The current study adds to the existing data by demonstrating for the first time an improvement in peak V̇O2, an objective measure of exercise capacity after successful CTO-PCI. While mean peak V̇O2 increased modestly by 1.4 mL/kg/min, previous studies have shown that this is a clinically meaningful improvement in both patients with congestive heart failure and coronary artery disease.32 In patients with coronary artery disease, Keteyian et al demonstrated that an increase in 1 mL/kg/min in peak V̇O2 was associated with a 15% decrease in all-cause and cardiovascular mortality.33 While currently there are no studies evaluating the association between outcomes and improvement in serial measurements of peak V̇O2 in patients with coronary artery disease, a 6% increase in peak V̇O2 at 6 months was associated with significant improvements in cardiovascular outcomes in congestive heart failure patients in the HF-ACTION (Heart Failure-A Controlled Trial Investigating Outcomes of Exercise Training) trial.32 In the current study, 16 of the 25 patients without a known occluded CTO who underwent baseline and follow-up CPX testing demonstrated a ≥1 mL/kg/min improvement in peak V̇O2. We did not perform repeat angiography as part of the study protocol at follow-up; therefore, it is possible that some patients may have developed restenosis. However, this would lead to an underestimation of the potential benefit of CTO-PCI. Further large studies assessing additional variables, such as severity of coronary ischemia and myocardial viability, are needed to determine which patients may benefit most from CTO-PCI.10
There are several potential explanations for the improvement in peak V̇O2 after CTO-PCI. Since the number of patients in whom the test was terminated due to chest pain decreased from 7 patients at baseline to 1 patient at follow-up, one explanation is that before CTO-PCI, patients were not able to exercise to their full capacity due to angina. This is supported by the observation that METS calculated from the treadmill speed and incline significantly increased at follow-up from baseline, as patients were able to advance to further stages. Another explanation is that myocardial ischemia at peak stress may lead to an inability to augment cardiac output, which is directly proportional to V̇O2, during the pre-CTO-PCI CPX but not during the post-CTO-PCI CPX. Alternatively, without ischemia limiting aerobic activity, patients who were significantly symptomatic prior to their CTO-PCI were able to train over the 5-month period to improve their performance on follow-up CPX. Finally, due to familiarity with the CPX test and placebo effect from the PCI procedure, patients may have been driven to exert themselves more on the follow-up test. Although we are not able to rule out this mechanism with this study, there was a lack of improvement in peak V̇O2 in both patients with known occluded CTO vessels.
Improvement in patient symptoms. The current study also demonstrated an improvement in patient symptoms, assessed both by physician-obtained history and validated questionnaires. Improvement was seen in both physician-assessed NYHA congestive heart failure class and CCS angina class. In addition to improvement in angina frequency, physical limitation, and quality of life, as well as treatment satisfaction components of the SAQ reported in previous studies,7-9 an improvement in angina stability was also found. Also, similar to previous reports,10 an improvement was seen in several components of the SF-36, with the improvements in the components associated with physical health being greater than components associated with emotional health. Finally, an improvement in DASI scores was seen, for the first time post CTO-PCI. The DASI score results complement our CPX findings of improvement in peak V̇O2, although the improvement in DASI scores was slightly greater than what is suggested by the improvement in peak V̇O2. One possible explanation for this is that additional co-morbidities, such as the higher frequency of hip and leg pain at follow-up test compared with baseline test, may limit maximal exercise on a treadmill but not interfere with daily vigorous activity.
Improvement in BNP levels. Our study demonstrated for the first time a decrease in plasma BNP levels after CTO-PCIs. There are many potential mechanisms for this, including improvement in LV systolic function, which has previously been demonstrated after successful CTO-PCI.31 In addition, coronary ischemia and coronary atherosclerosis itself may lead to elevated BNP levels,34 and treatment directed at these factors may lead to improvement in BNP levels. Elevated plasma BNPs have been associated with poor prognosis in stable coronary artery disease patients,35 and this surrogate marker, along with peak V̇O2, may be related to the improved prognosis reported in patients who undergo successful CTO-PCI as compared with patients in whom CTO-PCI fails.36
Study limitations. Our study has important limitations. First, although we found improvement in multiple objective measures, due to the lack of a control group, a placebo effect of CTO-PCI cannot be entirely eliminated. Future randomized studies using sham control are required to firmly establish the benefits of CTO-PCI. Second, the current study was underpowered to discern which patients who underwent CTO-PCI benefited the most and to make comparisons with those patients who either had an unsuccessful CTO-PCI attempt or developed restenosis. In addition, although some patients underwent repeat angiography as part of their clinical evaluation, most patients in the current study did not undergo repeat coronary angiography to detect restenosis of the CTO vessel as part of the study protocol. Therefore, some of the patients in whom the CTO target vessel was considered to be patent could have developed restenosis. Finally, although improvements were seen in several surrogate prognostic markers, such as peak V̇O2 and BNP, they may not translate into improvement in hard cardiac outcomes.
Conclusion
The current study demonstrates a significant improvement in exercise capacity, as assessed by peak V̇O2 on cardiopulmonary exercise test. Improvements were also seen in patient-reported exercise tolerance, anginal symptoms, and cardiac neurohormonal markers. These findings support CTO-PCI as a beneficial treatment option in patients with CTOs and angina or heart failure symptoms.
References
1. Christofferson RD, Lehmann KG, Martin GV, Every N, Caldwell JH, Kapadia SR. Effect of chronic total coronary occlusion on treatment strategy. Am J Cardiol. 2005;95:1088-1091.
2. Jeroudi OM, Alomar ME, Michael TT, et al. Prevalence and management of coronary chronic total occlusions in a tertiary Veterans Affairs hospital. Catheter Cardiovasc Interv. 2014;84:637-643.
3. Brilakis ES, Banerjee S, Karmpaliotis D, et al. Procedural outcomes of chronic total occlusion percutaneous coronary intervention: a report from the NCDR (National Cardiovascular Data Registry). JACC Cardiovasc Interv. 2015;8:245-253.
4. Patel VG, Brayton KM, Tamayo A, et al. Angiographic success and procedural complications in patients undergoing percutaneous coronary chronic total occlusion interventions: a weighted meta-analysis of 18,061 patients from 65 studies. JACC Cardiovasc Interv. 2013;6:128-136.
5. Christopoulos G, Menon RV, Karmpaliotis D, et al. The efficacy and safety of the “hybrid” approach to coronary chronic total occlusions: insights from a contemporary multicenter US registry and comparison with prior studies. J Invasive Cardiol. 2014;26:427-432.
6. Levine GN, Bates ER, Blankenship JC, et al. 2011 ACCF/AHA/SCAI guideline for percutaneous coronary intervention. A report of the American College of Cardiology Foundation/American Heart Association Task Force on Practice Guidelines and the Society for Cardiovascular Angiography and Interventions. J Am Coll Cardiol. 2011;58:e44-e122.
7. Borgia F, Viceconte N, Ali O, et al. Improved cardiac survival, freedom from MACE and angina-related quality of life after successful percutaneous recanalization of coronary artery chronic total occlusions. Int J Cardiol. 2012;161:31-38.
8. Grantham JA, Jones PG, Cannon L, Spertus JA. Quantifying the early health status benefits of successful chronic total occlusion recanalization: results from the FlowCardia’s Approach to Chronic Total Occlusion Recanalization (FACTOR) trial. Circ Cardiovasc Qual Outcomes. 2010;3:284-290.
9. Safley DM, Grantham JA, Hatch J, Jones PG, Spertus JA. Quality of life benefits of percutaneous coronary intervention for chronic occlusions. Catheter Cardiovasc Interv. 2014;84:629-634.
10. Rossello X, Pujadas S, Serra A, et al. Assessment of inducible myocardial ischemia, quality of life, and functional status after successful percutaneous revascularization in patients with chronic total coronary occlusion. Am J Cardiol. 2016;117:720-726.
11. Glass S, Gregory B. ACSM’s Metabolic Calculations Handbook. Baltimore: Lippincott Williams & Wilkins; 2007.
12. Hlatky MA, Boineau RE, Higginbotham MB, et al. A brief self-administered questionnaire to determine functional capacity (the Duke Activity Status Index). Am J Cardiol. 1989;64:651-654.
13. Brooks MM, Chung SC, Helmy T, et al. Health status after treatment for coronary artery disease and type 2 diabetes mellitus in the Bypass Angioplasty Revascularization Investigation 2 Diabetes trial. Circulation. 2010;122:1690-1699.
14. Eisenberg MJ, Wilson B, Lauzon C, et al. Routine functional testing after percutaneous coronary intervention: results of the aggressive diagnosis of restenosis in high-risk patients (ADORE II) trial. Acta Cardiol. 2007;62:143-150.
15. Hlatky MA, Rogers WJ, Johnstone I, et al. Medical care costs and quality of life after randomization to coronary angioplasty or coronary bypass surgery. Bypass Angioplasty Revascularization Investigation (BARI) Investigators. N Engl J Med. 1997;336:92-99.
16. Mark DB, Pan W, Clapp-Channing NE, et al. Quality of life after late invasive therapy for occluded arteries. N Engl J Med. 2009;360:774-783.
17. Nelson CL, Herndon JE, Mark DB, Pryor DB, Califf RM, Hlatky MA. Relation of clinical and angiographic factors to functional capacity as measured by the Duke Activity Status Index. Am J Cardiol. 1991;68:973-975.
18. Spertus JA, Winder JA, Dewhurst TA, et al. Development and evaluation of the Seattle Angina Questionnaire: a new functional status measure for coronary artery disease. J Am Coll Cardiol. 1995;25:333-341.
19. Spertus JA, Jones P, McDonell M, Fan V, Fihn SD. Health status predicts long-term outcome in outpatients with coronary disease. Circulation. 2002;106:43-49.
20. Spertus JA, Salisbury AC, Jones PG, Conaway DG, Thompson RC. Predictors of quality-of-life benefit after percutaneous coronary intervention. Circulation. 2004;110:3789-3794.
21. Weintraub WS, Spertus JA, Kolm P, et al. Effect of PCI on quality of life in patients with stable coronary disease. N Engl J Med. 2008;359:677-687.
22. McHorney CA, Ware JE Jr, Rogers W, Raczek AE, Lu JF. The validity and relative precision of MOS short- and long-form health status scales and Dartmouth COOP charts. Results from the Medical Outcomes Study. Med Care. 1992;30(5 Suppl):MS253-MS265.
23. van der Schaaf RJ, Vis MM, Sjauw KD, et al. Impact of multivessel coronary disease on long-term mortality in patients with ST-elevation myocardial infarction is due to the presence of a chronic total occlusion. Am J Cardiol. 2006;98:1165-1169.
24. Abbott JD, Kip KE, Vlachos HA, et al. Recent trends in the percutaneous treatment of chronic total coronary occlusions. Am J Cardiol. 2006;97:1691-1696.
25. Suero JA, Marso SP, Jones PG, et al. Procedural outcomes and long-term survival among patients undergoing percutaneous coronary intervention of a chronic total occlusion in native coronary arteries: a 20-year experience. J Am Coll Cardiol. 2001;38:409-414.
26. Grantham JA, Marso SP, Spertus J, House J, Holmes DR Jr, Rutherford BD. Chronic total occlusion angioplasty in the United States. JACC Cardiovasc Interv. 2009;2:479-486.
27. Hoye A, van Domburg RT, Sonnenschein K, Serruys PW. Percutaneous coronary intervention for chronic total occlusions: the Thoraxcenter experience 1992-2002. Eur Heart J. 2005;26:2630-2636.
28. Olivari Z, Rubartelli P, Piscione F, et al. Immediate results and one-year clinical outcome after percutaneous coronary interventions in chronic total occlusions: data from a multicenter, prospective, observational study (TOAST-GISE). J Am Coll Cardiol. 2003;41:1672-1678.
29. Prasad A, Rihal CS, Lennon RJ, Wiste HJ, Singh M, Holmes DR Jr. Trends in outcomes after percutaneous coronary intervention for chronic total occlusions: a 25-year experience from the Mayo Clinic. J Am Coll Cardiol. 2007;49:1611-1618.
30. Tomasello SD, Boukhris M, Giubilato S, et al. Management strategies in patients affected by chronic total occlusions: results from the Italian Registry of Chronic Total Occlusions. Eur Heart J. 2015;36:3189-3198.
31. Piscione F, Galasso G, De Luca G, et al. Late reopening of an occluded infarct related artery improves left ventricular function and long term clinical outcome. Heart. 2005;91:646-651.
32. Swank AM, Horton J, Fleg JL, et al. Modest increase in peak VO2 is related to better clinical outcomes in chronic heart failure patients: results from heart failure and a controlled trial to investigate outcomes of exercise training. Circ Heart Fail. 2012;5:579-585.
33. Keteyian SJ, Brawner CA, Savage PD, et al. Peak aerobic capacity predicts prognosis in patients with coronary heart disease. Am Heart J. 2008;156:292-300.
34. Abdullah SM, Khera A, Das SR, et al. Relation of coronary atherosclerosis determined by electron beam computed tomography and plasma levels of n-terminal pro-brain natriuretic peptide in a multiethnic population-based sample (the Dallas Heart Study). Am J Cardiol. 2005;96:1284-1289.
35. Omland T, Sabatine MS, Jablonski KA, et al. Prognostic value of B-type natriuretic peptides in patients with stable coronary artery disease: the PEACE Trial. J Am Coll Cardiol. 2007;50:205-214.
36. Christakopoulos GE, Christopoulos G, Carlino M, et al. Meta-analysis of clinical outcomes of patients who underwent percutaneous coronary interventions for chronic total occlusions. Am J Cardiol. 2015;115:1367-1375.
From the 1Department of Internal Medicine and 2Department of Radiology, VA North Texas Healthcare System, Dallas, Texas; and 3University of Texas-Southwestern Medical Center, Dallas, Texas.
Funding: This work was supported by a Dallas VA Research Corporation Start-up Grant and with resources and the use of facilities at the VA North Texas Health Care System.
Disclosure: The authors have completed and returned the ICMJE Form for Disclosure of Potential Conflicts of Interest. Dr Abdullah reports a grant from the Dallas VA Research Cooperation and a VA VISN 17 Start-Up grant. Dr Rangan reports grants from Spectranetics Corporation and InfraRedX, Inc. Dr Banerjee reports research grants from Gilead and the Medicines Company; consultant/speaker honoraria from Covidien, Merck, and Medtronic; ownership in MDCare Global (spouse); intellectual property in HygeiaTel; educational grant from Boston Scientific (spouse). Dr Brilakis reports consulting/speaker honoraria from Abbott Vascular, Asahi Intecc, Boston Scientific, Elsevier, Somahlution, St Jude Medical, and Terumo; research support from Boston Scientific and InfraRedx; spouse is employee of Medtronic. The remaining authors report no conflicts of interest regarding the content herein.
Manuscript submitted September 2, 2016, provisional acceptance given September 13, 2016, final version accepted October 25, 2016.
Address for correspondence: Shuaib Abdullah, MD, MSCs, Dallas VA Medical Center (111A), 4500 South Lancaster Road, Dallas, TX 75216. Email: shuaib.abdullah@va.gov







