

Optical Coherence Tomography for Guiding Plaque Stabilization in a Patient With Myocardial Infarction and Massive Coronary Thrombosis
J INVASIVE CARDIOL 2018;30(7):E59-E60.
Key words: medical therapy, cardiac imaging, early coronary artery disease
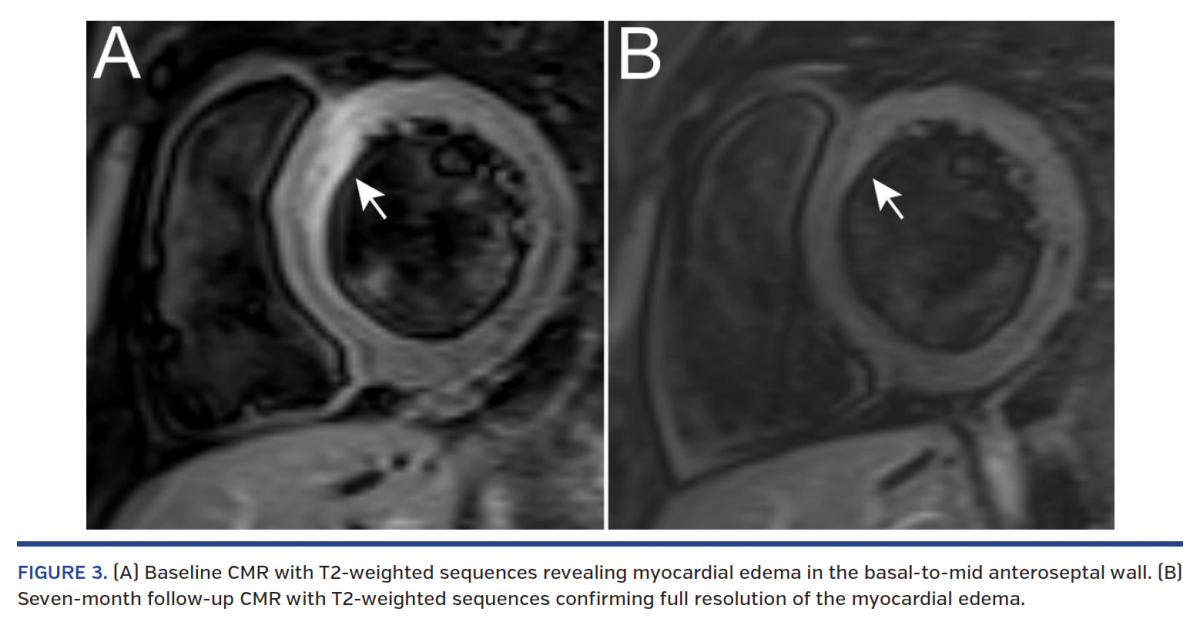
A 22-year-old, obese male smoker with untreated hyperlipidemia and family history of coronary artery disease presented with chest pain and ST-segment elevation in anterolateral leads at ECG following heavy marijuana and alcohol abuse. Coronary angiography showed a moderate stenosis in the proximal left anterior descending (LAD) coronary artery along with distal embolization (Figure 1A; Video 1). No concomitant coronary stenoses were noted, and TIMI 3 flow was present in the LAD. Optical coherence tomography (OCT) revealed plaque erosion with massive thrombi involving the distal left main coronary artery (LMCA) and ostial to mid LAD (Figure 1A; Video 2), along with preserved lumen area of the LAD. Given the diffuse extent of non-obstructive CAD involving the LMCA on OCT, aggressive medical thera-py with glycoprotein IIb/IIIa blocker, aspirin, ticagrelor, and high-dose statin was initiated. At discharge, cardiac magnetic resonance (CMR) imaging showed subendocardial infarction in the basal anteroseptal and lateral walls, and transmural infarction in the apex (Figure 2). After 3 months, repeat angiography with OCT demonstrated a non-obstructive lesion with fully healed fibroatheroma (Figure 1B; Videos 3 and 4). At 7 months, the patient was asymptomatic and control CMR showed preserved left ventricular function with resolution of myocardial edema (Figure 3; Video 5).



Data are limited on the treatment options for myocardial infarction with eroded coronary plaque. Herein, we present the favorable outcome of an OCT-guided watchful-waiting strategy to avoid the invasive treatment of the LMCA in a very young patient with massive coronary thrombosis.
 View the accompanying Video Series here.
View the accompanying Video Series here.
From 1the Department of Interventional Cardiology and Angiology, Institute of Cardiology, Warsaw, Poland; 2First Department of Cardiology, Medical University of Gdansk, Gdansk, Poland; 3Department of Coronary and Structural Heart Diseases, Institute of Cardiology, Warsaw, Poland.
Funding: This work was supported by research grant “Iuventus Plus” from the Polish Ministry of Science and Higher Education (IP2014 034073).
Disclosure: The authors have completed and returned the ICMJE Form for Disclosure of Potential Conflicts of Interest. The authors report no conflicts of interest regarding the content herein.
Manuscript accepted March 2, 2018.
Address for correspondence: Dr Maksymilian P. Opolski, Department of Interventional Cardiology and Angiology, Institute of Cardiology, Alpejska 42, 04-628 Warsaw, Poland. Email: opolski.mp@gmail.com







