

Intracoronary Dehiscence of Radiopaque Ring of a Guiding Catheter and its Retrieval
ABSTRACT: Intracoronary dehiscence of the radiopaque ring of a guiding catheter is a rare complication, which could lead to myocardial infarction, emergency surgery, or even death. We describe the percutaneous retrieval of the catheter material from the right coronary artery, thus avoiding surgery and related complications.
J INVASIVE CARDIOL 2012;24(9):E182-E184
Key words: complications, coronary angioplasty, radiopaque ring retrieval
_________________________________________________________
 The technique of coronary angioplasty described by Gruntzig,1 a valuable therapeutic modality for coronary disease is associated with complications related to the lesion characteristics, operator experience and also those related to the catheter system. The complications related to the catheter system during Percutaneous Coronary Angioplasty (PTCA) maybe a fractured guide wire, balloon leak, catheter breakage or loss of the stent within the coronary artery. This may lead to coronary dissection, thrombus formation, distal embolization, or perforation.2-4 Transcatheter retrieval is the quickest and the least invasive method which can also prevent surgery and related complications.5,6 About 15%-20% of patients with failed percutaneous retrieval of misplaced catheter remnants are referred to emergent cardiac surgery.6,7
The technique of coronary angioplasty described by Gruntzig,1 a valuable therapeutic modality for coronary disease is associated with complications related to the lesion characteristics, operator experience and also those related to the catheter system. The complications related to the catheter system during Percutaneous Coronary Angioplasty (PTCA) maybe a fractured guide wire, balloon leak, catheter breakage or loss of the stent within the coronary artery. This may lead to coronary dissection, thrombus formation, distal embolization, or perforation.2-4 Transcatheter retrieval is the quickest and the least invasive method which can also prevent surgery and related complications.5,6 About 15%-20% of patients with failed percutaneous retrieval of misplaced catheter remnants are referred to emergent cardiac surgery.6,7
Case Report. A 62-year-old female patient with a history of type 2 diabetes and essential hypertension presented with acute chest pain suggestive of angina. She was hemodynamically stable with the electrocardiogram showing significant ST elevations in the inferior leads. She was immediately moved to the cath lab for a coronary angiogram to decide the course of treatment.
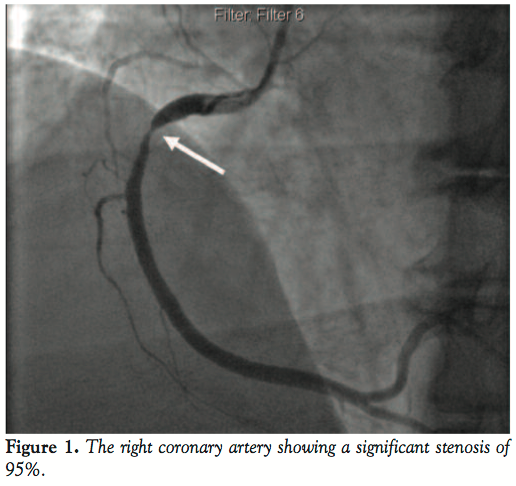
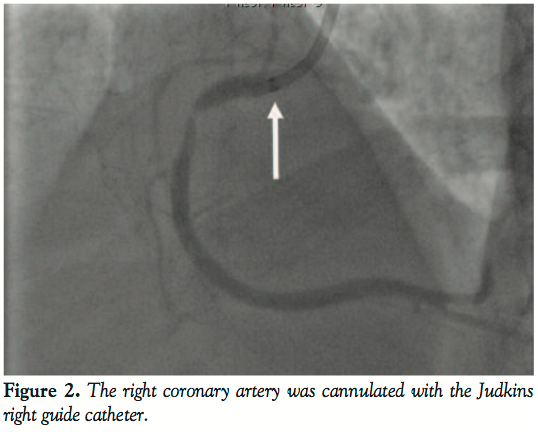 Coronary angiogram revealed a significantly tight stenosis of 95% in the proximal segment of the right coronary artery (RCA) with the other vessels having no significant disease (Figure 1). We treated the culprit vessel percutaneously by cannulating the RCA with a 7 Fr Judkins right guiding catheter (Figure 2) and using a 0.014” Galeo wire (Biotronik) to cross the lesion. The lesion was predilated with 3 mm x 10 mm Sprinter balloon (Medtronic) at 10 atm (Figure 3). However, just after withdrawing the balloon into the
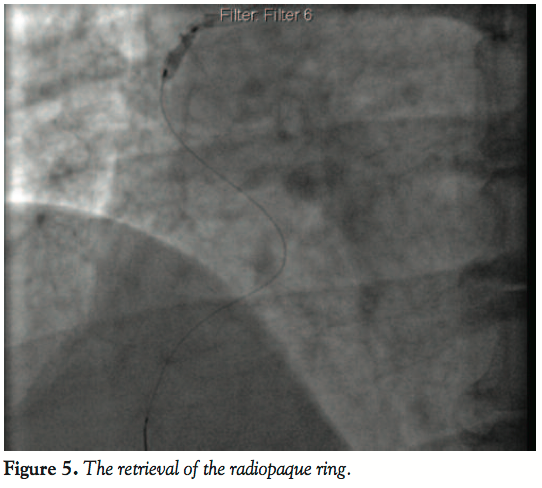
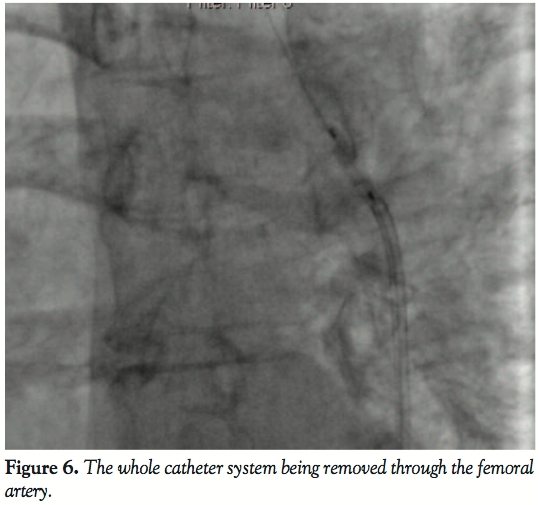
Coronary angiogram revealed a significantly tight stenosis of 95% in the proximal segment of the right coronary artery (RCA) with the other vessels having no significant disease (Figure 1). We treated the culprit vessel percutaneously by cannulating the RCA with a 7 Fr Judkins right guiding catheter (Figure 2) and using a 0.014” Galeo wire (Biotronik) to cross the lesion. The lesion was predilated with 3 mm x 10 mm Sprinter balloon (Medtronic) at 10 atm (Figure 3). However, just after withdrawing the balloon into the  catheter, we noticed that the radiopaque rubber ring, which is attached to the distal end of the guide catheter, was cut off from the catheter (Figure 4). Almost immediately, the same balloon was advanced further beyond the radiopaque ring, inflated to 4 atm to trap the ring, and the whole catheter system was removed through the femoral artery (Figures 5 and 6). The RCA was recannulated and a 3.5 mm x 24 mm Biomatrix stent (Biosensors International) deployed at 16 atm (Figure 7). This was followed by postdilatation of the stented segment with 3.5 mm x 10 mm NC Mercury balloon (Abbott). The procedure was completed successfully without any adverse event. The impending complications related to the remnants of the catheter system were prevented by early recognition of the dehisced radiopaque ring of the guide catheter, which could have caused myocardial infarction, arrhythmias, or sudden death.
catheter, we noticed that the radiopaque rubber ring, which is attached to the distal end of the guide catheter, was cut off from the catheter (Figure 4). Almost immediately, the same balloon was advanced further beyond the radiopaque ring, inflated to 4 atm to trap the ring, and the whole catheter system was removed through the femoral artery (Figures 5 and 6). The RCA was recannulated and a 3.5 mm x 24 mm Biomatrix stent (Biosensors International) deployed at 16 atm (Figure 7). This was followed by postdilatation of the stented segment with 3.5 mm x 10 mm NC Mercury balloon (Abbott). The procedure was completed successfully without any adverse event. The impending complications related to the remnants of the catheter system were prevented by early recognition of the dehisced radiopaque ring of the guide catheter, which could have caused myocardial infarction, arrhythmias, or sudden death.
 Discussion. Complications related to the catheter delivery system are very rare. One series of 5,400 consecutive PTCA procedures reported 12 patients (0.2%) who had complications resulting in retention of PTCA equipment components.4 The components were composed of twisted catheter tips,6 broken wires,5 entrapped balloons, or undeployed stents,10 all of which were subjected to immediate removal. The following methods, including snares, baskets, forceps, cardiac bioptome, balloon catheters, and 2-wire technique, can be used to retrieve the objects.
Discussion. Complications related to the catheter delivery system are very rare. One series of 5,400 consecutive PTCA procedures reported 12 patients (0.2%) who had complications resulting in retention of PTCA equipment components.4 The components were composed of twisted catheter tips,6 broken wires,5 entrapped balloons, or undeployed stents,10 all of which were subjected to immediate removal. The following methods, including snares, baskets, forceps, cardiac bioptome, balloon catheters, and 2-wire technique, can be used to retrieve the objects.
 Trehan et al described the retrieval of an embolized coronary angioplasty balloon catheter, which happened due to the breakage of the shaft of the balloon catheter system.10 The complications such as failure to deflate the balloon, migration of the distal end of the guidewires into the distal segments of the coronary arteries, ruptured balloons and fractured shafts of the catheters are also known.
Trehan et al described the retrieval of an embolized coronary angioplasty balloon catheter, which happened due to the breakage of the shaft of the balloon catheter system.10 The complications such as failure to deflate the balloon, migration of the distal end of the guidewires into the distal segments of the coronary arteries, ruptured balloons and fractured shafts of the catheters are also known.
 Chen et al9 had retrieved the missing radiopaque ring of the Amplatz guiding catheter during the PTCA of the RCA. The dehiscence of the ring was noted after completing the procedure. They used a Magnum guidewire because it had a large and blunt tip, which did not allow it to slide between the ring and the vessel wall. A balloon was passed through the ring, inflated at low pressures, and the dehisced radiopaque ring was removed.
Chen et al9 had retrieved the missing radiopaque ring of the Amplatz guiding catheter during the PTCA of the RCA. The dehiscence of the ring was noted after completing the procedure. They used a Magnum guidewire because it had a large and blunt tip, which did not allow it to slide between the ring and the vessel wall. A balloon was passed through the ring, inflated at low pressures, and the dehisced radiopaque ring was removed.
 In our case, we noticed the dehiscence of the ring very early during the procedure just after the balloon inflation to predilate the lesion in the proximal segment of the RCA. The guidewire was still in place so we just re-entered the ring through the same balloon, which was still within the catheter, inflated it at low pressures, and retrieved the ring of the right Judkins guiding catheter. However, one has to be careful enough not to push the ring further into the vessel, which can make the retrieval more difficult and may necessitate surgery. This complication can rarely occur while amplatzing the Judkins right guide catheter to get a better support during PTCA to RCA.8 It is noteworthy that this complication occurred even though we did not attempt to amplatz the JR or push balloons, stents, or hardwires. There was absolutely no aggressiveness on the part of the operator to anticipate any complications that were related to the catheter system.
In our case, we noticed the dehiscence of the ring very early during the procedure just after the balloon inflation to predilate the lesion in the proximal segment of the RCA. The guidewire was still in place so we just re-entered the ring through the same balloon, which was still within the catheter, inflated it at low pressures, and retrieved the ring of the right Judkins guiding catheter. However, one has to be careful enough not to push the ring further into the vessel, which can make the retrieval more difficult and may necessitate surgery. This complication can rarely occur while amplatzing the Judkins right guide catheter to get a better support during PTCA to RCA.8 It is noteworthy that this complication occurred even though we did not attempt to amplatz the JR or push balloons, stents, or hardwires. There was absolutely no aggressiveness on the part of the operator to anticipate any complications that were related to the catheter system.
To our knowledge this is only the second report of dehisced ring during PTCA and the first with Judkins right guide catheter. The dehisced ring could have been a nidus for thrombus formation, acute occlusion of the RCA, myocardial infarction, arrhythmias, and even death.
References
- Grüntzig AR, Senning A, Siegenthaler WE. Nonoperative dilatation of coronary-artery stenosis: percutaneous transluminal coronary angioplasty. N Engl J Med. 1979;301(2):61-68.
- Cowley MJ, Dorros G, Kelsey SF, Van Raden M, Detre KM. Acute coronary events associated with percutaneous transluminal coronary angioplasty. Am J Cardiol. 1984;53(12):12C-16C.
- Bredlau CE, Roubin GS, Leimgruber PP, Douglas JS Jr, King SB 3rd, Gruentzig AR. In-hospital morbidity and mortality in patients undergoing elective coronary angioplasty. Circulation. 1985;72(5):1044-1052.
- Hartzler GO, Rutherford BD, McConahay DR. Retained percutaneous transluminal coronary angioplasty equipment components and their management. Am J Cardiol. 1987;60(6):1260-1264.
- Ghosh PK, Alber G, Schistek R, Unger F. Rupture of guide wire during percutaneous transluminal coronary angioplasty. Mechanics and management. J Thorac Cardiovasc Surg. 1989;97(3):467-469.
- Rosario PG, Donahoo JS. Coronary artery endarterectomy for retrieval of entrapped percutaneous angioplasty catheter. Ann Thorac Surg. 1996;61(1):218-219.
- Reidemeister JC, Wolfhard U. Direct coronary bypass operation in complicated coronary dissection [in German]. Z Kardiol. 1996;85 Suppl 1:67-72.
- Abhaichand RK, Lefèvre T, Louvard Y, Morice MC. Amplatzing a 6 Fr Judkins right guiding catheter for increased success in complex right coronary artery anatomy. Catheter Cardiovasc Interv. 2001;53(3):405-409.
- Chen Y, Fang CC, Yu CL, Jao YT, Wang SP. Intracoronary retrieval of the dehisced radiopaque ring of a guiding catheter: an unusual complication of coronary angioplasty. Catheter Cardiovasc Interv. 2002;55(2):262-264.
- Trehan V, Mukhopadhyay S, Yusuf J, C Ramgasetty U, Mukherjee S, Arora R. Intracoronary fracture and embolization of a coronary angioplasty balloon catheter: retrieval by a simple technique. Catheter Cardiovasc Interv. 2003;58(4):473-477.
_________________________________________________________
From the Sri Jayadeva Institute of Cardiovascular Sciences and Research, Bangelore, India.
Disclosure: The authors have completed and returned the ICMJE Form for Disclosure of Potential Conflicts of Interest. The authors report no conflicts of interest regarding the content herein.
Manuscript submitted March 12, 2012, provisional acceptance given March 21, 2012, final version accepted March 30, 2012.
Address for correspondence: Dr Jayashree Kharge, Sri Jayadeva Institute of Cardiovascular Sciences and Research, Jaya Nagar 9th Block, BG Road, Bangelore 560069, India. Email: jrad2can@yahoo.co.in





