

High-Risk Percutaneous Coronary Intervention with the Tandem Heart and Impella Devices: A Single-Center Experience
 Abstract: Background. Intra-aortic balloon pumps (IABPs) are indicated during high-risk percutaneous coronary intervention (HR-PCI) to reduce major procedural complications. The clinical utility of the newer Impella and TandemHeart devices is not clear. This study determined the baseline characteristics, hemodynamics, and outcomes of patients treated with prophylactic percutaneous left ventricular assist devices (PLVADs) during HR-PCI. Methods. A retrospective analysis at a private, tertiary referral hospital was conducted of all cases involving prophylactic PLVAD during HR-PCI between January 1, 2008 and June 30, 2010. General practice in this institution involves a tiered approach to PLVAD whereby patients with the least, intermediate, and highest risk of left ventricular failure are treated with an IABP, Impella, or TandemHeart, respectively. Results. Fifty cases were identified (5 IABP, 13 Impella, 32 TandemHeart). Mean ejection fraction was 31 ± 17%. All devices (100%) were initiated successfully. Angiographic success was achieved in 96% (80% IABP, 100% Impella, 97% TandemHeart). Of the 38 patients not in cardiogenic shock, death occurred in 1 (2.6%), recurrent ischemia in 3 (8%), and stroke in 0%. Shortly after device removal, systolic blood pressure (mean increase, +5 ± 22 mmHg) and ejection fraction (mean increase, +7.4 ± 11%; p = 0.0006) increased in all 3 groups, suggesting a beneficial effect on the myocardium. Conclusions. In patients undergoing HR-PCI with Impella and TandemHeart support, angiographic success was high and major complication rates were low. A tiered approach where patients with the least, intermediate, and highest risk of left ventricular failure are treated with an IABP, Impella, or TandemHeart, respectively, theoretically maximizes appropriate hemodynamic support and minimizes complications. Further studies are warranted.
Abstract: Background. Intra-aortic balloon pumps (IABPs) are indicated during high-risk percutaneous coronary intervention (HR-PCI) to reduce major procedural complications. The clinical utility of the newer Impella and TandemHeart devices is not clear. This study determined the baseline characteristics, hemodynamics, and outcomes of patients treated with prophylactic percutaneous left ventricular assist devices (PLVADs) during HR-PCI. Methods. A retrospective analysis at a private, tertiary referral hospital was conducted of all cases involving prophylactic PLVAD during HR-PCI between January 1, 2008 and June 30, 2010. General practice in this institution involves a tiered approach to PLVAD whereby patients with the least, intermediate, and highest risk of left ventricular failure are treated with an IABP, Impella, or TandemHeart, respectively. Results. Fifty cases were identified (5 IABP, 13 Impella, 32 TandemHeart). Mean ejection fraction was 31 ± 17%. All devices (100%) were initiated successfully. Angiographic success was achieved in 96% (80% IABP, 100% Impella, 97% TandemHeart). Of the 38 patients not in cardiogenic shock, death occurred in 1 (2.6%), recurrent ischemia in 3 (8%), and stroke in 0%. Shortly after device removal, systolic blood pressure (mean increase, +5 ± 22 mmHg) and ejection fraction (mean increase, +7.4 ± 11%; p = 0.0006) increased in all 3 groups, suggesting a beneficial effect on the myocardium. Conclusions. In patients undergoing HR-PCI with Impella and TandemHeart support, angiographic success was high and major complication rates were low. A tiered approach where patients with the least, intermediate, and highest risk of left ventricular failure are treated with an IABP, Impella, or TandemHeart, respectively, theoretically maximizes appropriate hemodynamic support and minimizes complications. Further studies are warranted.
J INVASIVE CARDIOL 2011;23(10):417–424
Key words: interventional cardiology, hemodynamics, high-risk PTCA, new devices
____________________________________________
 Percutaneous coronary intervention (PCI) may carry a risk of procedural complications, including coronary dissection (5–12%), sidebranch occlusion (3%), and abrupt vessel closure (2%).1,2 Major complications, including death, Q-wave myocardial infarction (MI), or the need for emergency bypass surgery, occur in 3–5% of all PCIs.1-3 Procedural complications are more likely to precipitate major clinical complications during interventions involving vessels that supply a large portion of viable myocardium, including interventions on the left main coronary artery, on the last remaining non-occluded vessel, and multivessel interventions in patients with severely reduced ejections fractions (EF). For patients with high-risk features, prophylactic use of an intra-aortic balloon pump (IABP) reduced intraprocedural complications,4-7 but has failed to demonstrate a clear mortality benefit. Recent guidelines3 do not provide formal recommendations on the use of elective IABP during high-risk PCI (HR-PCI), but defer the decision to the physician’s clinical judgment based on the patient’s overall status and coronary anatomy.
Percutaneous coronary intervention (PCI) may carry a risk of procedural complications, including coronary dissection (5–12%), sidebranch occlusion (3%), and abrupt vessel closure (2%).1,2 Major complications, including death, Q-wave myocardial infarction (MI), or the need for emergency bypass surgery, occur in 3–5% of all PCIs.1-3 Procedural complications are more likely to precipitate major clinical complications during interventions involving vessels that supply a large portion of viable myocardium, including interventions on the left main coronary artery, on the last remaining non-occluded vessel, and multivessel interventions in patients with severely reduced ejections fractions (EF). For patients with high-risk features, prophylactic use of an intra-aortic balloon pump (IABP) reduced intraprocedural complications,4-7 but has failed to demonstrate a clear mortality benefit. Recent guidelines3 do not provide formal recommendations on the use of elective IABP during high-risk PCI (HR-PCI), but defer the decision to the physician’s clinical judgment based on the patient’s overall status and coronary anatomy.
Since 1968, the IABP has been the only widely used percutaneous left ventricular assist device (PLVAD) until the recent introduction of the TandemHeart (CardiacAssist, Inc.) and Impella Recover 2.5 (Abiomed, Inc.) devices. Compared with the IABP, the newer PLVADs provide increased hemodynamic support.8-10 Patients who suffer circulatory collapse during HR-PCI may benefit from increased hemodynamic support. However, these new PLVADs also increased the incidences of bleeding and leg ischemia compared with the IABP.9-11 Reports on these new PLVADs in patients undergoing HR-PCI are limited to small retrospective analyses,12-17 a limited registry,18 and a recent, small retrospective comparison,19 so their clinical utility is not clear. Therefore, the goal of this study is to investigate the baseline characteristics, hemodynamic parameters, and outcomes of patients treated with prophylactic PLVAD during HR-PCI in our facility to better define their use in contemporary practice.
Methods
Approval from the Western Institutional Review Board was obtained for this retrospective analysis at Good Samaritan Hospital, a private, tertiary referral hospital. The current study expands on a previous report on the TandemHeart device.16 In addition to more patients treated with a TandemHeart device, this report also includes patients treated with an IABP or Impella and additional endpoints that the previous report did not explore. The electronic medical record database was searched to identify all cases involving PLVAD (IABP, Impella, or TandemHeart) between January 1, 2008 and June 30, 2010, during which time each PLVAD was available. Cases were included if the device was used prophylactically during HR-PCI, defined as a patient with a severely reduced EF undergoing PCI on the left main coronary artery, PCI on the last remaining non-occluded vessel, PCI on a vessel supplying >50% of the remaining viable myocardium, complex PCI on multiple major vessels, or balloon aortic valvuloplasty. Patients who underwent emergent device placement for the treatment of cardiogenic shock were excluded because this represents a different disease state than patients undergoing HR-PCI (severe acute disease versus severe chronic disease) and two different clinical settings (emergent versus elective device placement). However, patients were included if they were already being treated for cardiogenic shock and had stabilized prior to undergoing elective insertion of a PLVAD for additional support during HR-PCI. The decision to use a device, the type of device, the type of PCI, and all other clinical decisions were at the discretion of the treating physicians. A comprehensive chart review was conducted to record patient demographics, medical history, procedural characteristics, and in-hospital outcomes.
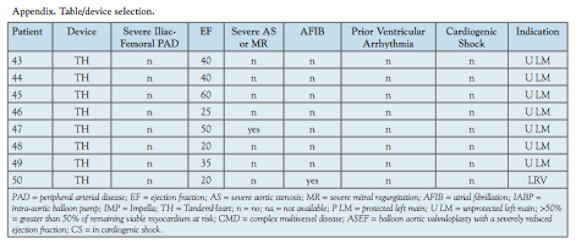
Device selection. All patients had severe disease prompting the use of a PLVAD. Patients with the lowest, intermediate, and highest risk of circulatory collapse were treated with IABP, Impella, or TandemHeart, respectively. This tiered approach relates to the potential quantity of hemodynamic support provided by each device (IABP 0.5 L/min; Impella 2.5 L/min; TandemHeart 3.5–5 L/min). Moreover, the TandemHeart device provides adequate hemodynamic support even in the complete absence of inherent left ventricular function, whereas the IABP and Impella require at least partial intrinsic cardiac output and blood flow.
The Impella device was avoided in patients with a left ventricular thombus or severe aortic stenosis. Use of the TandemHeart device required an operator with transeptal puncture skills. Both new PLVADs required the absence of severe bilateral femoral atherosclerosis because of their large sheath sizes. Severe bilateral iliac atherosclerosis or recent stenting was an absolute contraindication to the TandemHeart device, which utilizes a 15 (or 17) Fr inflow catheter positioned though the iliac artery (from the common femoral through the aorta), and was a relative contraindication to the Impella device. The 13 Fr Impella motor unit passes through the iliac artery, but once the motor unit has passed by, the catheter that remains in the iliac artery during the procedure is smaller. Thus, a lower threshold of disease in the iliac arteries precluded use of the TandemHeart compared with the Impella.
Severe femoral-iliac disease prohibited use of the TandemHeart in 5 patients, which accounts for some of the highest-risk patients treated with IABP and Impella devices. Other than the patients with severe femoral-iliac disease, zero IABP and Impella patients had severe valvular disease or atrial fibrillation and the mean EF was 42% with IABP, 32% with the Impella and 32% with the TandemHeart.
Several criteria were used to determine the risk of total circulatory collapse and identify patients to be treated with a TandemHeart device, including the severity of baseline left ventricular dysfunction, the presence of severe mitral regurgitation or aortic stenosis, the presence of cardiogenic shock, history of ventricular arrhythmias, the presence of atrial fibrillation, and the overall clinical status of the patient. High-risk coronary anatomy was also considered, including an intervention on the last remaining vessel, on an unprotected left main coronary artery, and the portion of remaining viable myocardium at risk during the procedure. Other than patients with severe femoral-iliac disease, patients treated with a TandemHeart device were more likely to have severe mitral regurgitation or aortic stenosis (7 versus 0 with an IABP or Impella) a history of ventricular arrhythmias or atrial fibrillation (6 versus 0), cardiogenic shock (7 versus 3), and HR-PCI on the last remaining vessel or an unprotected left main (18 versus 2).
Applying these criteria, patients at higher risk of total circulatory collapse were preferentially treated with a TandemHeart, patients at risk of major, subtotal hemodynamic compromise were treated with an Impella, and patients with lower risk were treated with an IABP. Thus, device selection was a measure of overall disease severity. This selection bias precludes direct comparisons between groups. See invasivecardiology.com (Schwartz; Appendix 1) for a detailed list of device selection specifics for each patient.
IABP insertion technique. Insertion of an 8 Fr, 40 cc Fidelity IABP (MAQUET Cardiovascular) was performed via either femoral artery using the retrograde guidewire technique. The tip of the IABP was placed inferior to the left subclavian artery. Support was maintained with one to one counterpulsation.
Impella insertion technique. The femoral artery was “preclosed” using two Perclose devices (Abbott Vascular), then upsized to a 13 Fr sheath. A 0.038˝ guidewire through a pigtail catheter was passed across the aortic valve. The guidewire was exchanged for a dedicated 0.018˝ Impella guidewire and the pigtail catheter was removed. The Impella device was then advanced retrogradely across the aortic valve and into the left ventricle. Proper positioning was confirmed by fluoroscopy. The Impella device was then activated at the lowest level (P1) and the setting was titrated to achieve approximately 2.5 L/min of hemodynamic support.
TandemHeart insertion technique. Transeptal puncture was performed via the right femoral vein using a Brockenbrough needle and a modified Mullins sheath. A stiff 0.035˝ guidewire was then placed in the left atrium and the Mullins sheath was exchanged for a 14/21 two-stage dilator, which was then exchanged for the 21 Fr TandemHeart transeptal cannula. The external end of the TandemHeart cannula was secured to the patient’s right thigh. The left femoral artery was “preclosed,” then upsized to a 15 (or 17) Fr TandemHeart arterial cannula. The arterial cannula was placed superior to the aortic bifurcation and the external end was secured to the patient’s left thigh. Air was removed from the system and the venous and arterial cannulae were attached to the external TandemHeart centrifugal pump. Heparinized saline was used to cool, lubricate, and anticoagulate the pump. The pump was attached to the control system. The speed was titrated to achieve approximately 3.5 L/min of hemodynamic support.
Definitions. Cardiogenic shock was defined as persistent hypotension (systolic blood pressure <90 mmHg for >20 minutes) or requiring vasopressor or PLVAD support to maintain a systolic blood pressure >90 mmHg. Clinical outcomes were documented during the index hospitalization and at 30 days, if available in the medical record. Recurrent ischemia was defined as new creatine kinase elevation 3 times above the upper limit of normal or, in patients who originally presented with a myocardial infarction, any second rise in a previously declining creatine kinase or cardiac troponin. ST-segment elevation myocardial infarction (STEMI) was defined as recurrent ischemia with new ST-segment elevations on electrocardiogram. Major adverse cardiac events (MACE) were defined as death, recurrent ischemia, STEMI, or cerebral vascular accident. Angiographic success was defined as <30% residual stenosis and TIMI grade 3 flow at the conclusion of the procedure. For aortic valvuloplasty, “angiographic” success was defined as a final aortic valve gradient of <25 mmHg or a ≥50% reduction in aortic valve gradient. Procedural success was defined as angiographic success with survival until the patient was transferred out of the catheterization laboratory. TIMI minor bleeding was defined as a decrease in hemoglobin of 3.0–4.9 g/dl and TIMI major bleeding as a decrease of ≥5.0 g/dl (counting each transfused unit of packed red blood cells as a decrease in hemoglobin of 1.0 g/dl).
For hemodynamic and laboratory data, the “before” value was defined as the most recent value prior to device insertion, the “during” value was defined as approximately 30 minutes after device insertion, and the “after” value was defined as 30–60 minutes after the device was removed (hemodynamic data) or the first available value after device removal (laboratory data and EF). For all data points, an effort was made to avoid outlier values by evaluating the surrounding data points and the overall trend. Measurements were chosen for inclusion that corresponded with the surrounding data and the overall trend. Before-during change was defined as the value during minus the before value. Before-after change was calculated by subtracting the before value from the after value. Before-during change and before-after change were calculated using only the patients with both values, before and during, or before and after, respectively. EF was routinely determined by echocardiography in these high-risk patients prior to HR-PCI. EF was measured prior to device placement and after device removal (not during device use). EF was determined by visual estimation, prospectively, without regard to this research project.
Statistics. Results are reported as the mean ± standard deviation or percentages of the total. Data are reported for all patients combined, in addition to groups based on the PLVAD used: IABP, Impella, or TandemHeart. Using Microsoft Office Excel, a paired t-test for means was used to identify changes in EF and systolic blood pressure measurements before and after the device was used. Statistical significance was considered a p-value <0.05.
Results
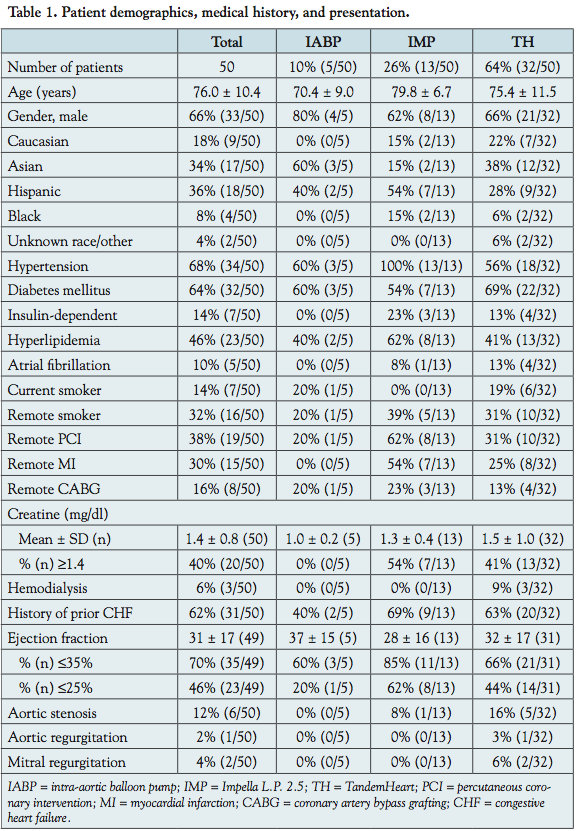 Fifty HR-PCI were performed with PLVADs. Five patients received an IABP, 13 received an Impella, and 32 received a TandemHeart (Table 1). Patients who underwent emergent device placement for cardiogenic shock will be reported separately (76 patients total; 50 IABP, 7 Impella, 19 TandemHeart). Patients undergoing HR-PCI were elderly (mean age, 76.0 ± 10.4 years) and comorbidities were common. Thirty-eight percent had undergone previous PCI, 30% had a previous MI, and 16% had prior coronary artery bypass graft surgery,
Fifty HR-PCI were performed with PLVADs. Five patients received an IABP, 13 received an Impella, and 32 received a TandemHeart (Table 1). Patients who underwent emergent device placement for cardiogenic shock will be reported separately (76 patients total; 50 IABP, 7 Impella, 19 TandemHeart). Patients undergoing HR-PCI were elderly (mean age, 76.0 ± 10.4 years) and comorbidities were common. Thirty-eight percent had undergone previous PCI, 30% had a previous MI, and 16% had prior coronary artery bypass graft surgery,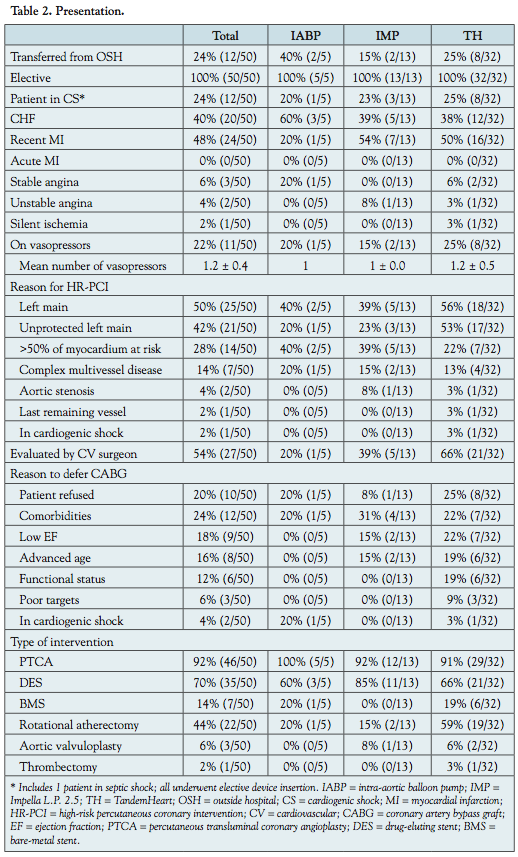 reflecting long-standing coronary artery disease. Mean EF was 31 ± 17%. All devices were placed electively prior to HR-PCI. Twelve patients (24%) underwent elective PLVAD support for HR-PCI while being treated for shock (11 cardiogenic, 1 septic shock), which was managed before and after the HR-PCI with vasopressors (Table 2). No patients had clinical cardiac tamponade or evidence of significant pericardial effusion on echocardiography. Most patients presented with decompensated congestive heart failure (40%) or a recent MI (48%).
reflecting long-standing coronary artery disease. Mean EF was 31 ± 17%. All devices were placed electively prior to HR-PCI. Twelve patients (24%) underwent elective PLVAD support for HR-PCI while being treated for shock (11 cardiogenic, 1 septic shock), which was managed before and after the HR-PCI with vasopressors (Table 2). No patients had clinical cardiac tamponade or evidence of significant pericardial effusion on echocardiography. Most patients presented with decompensated congestive heart failure (40%) or a recent MI (48%).
Indications for PLVAD use during HR-PCI included left main intervention (50%), >50% of viable myocardium at risk (28%), and complex multivessel disease (14%) (Table 2). The most common types of interventions included percutaneous transluminal coronary angioplasty (92%), drug-eluting stent implantation (70%), and rotational atherectomy (44%).
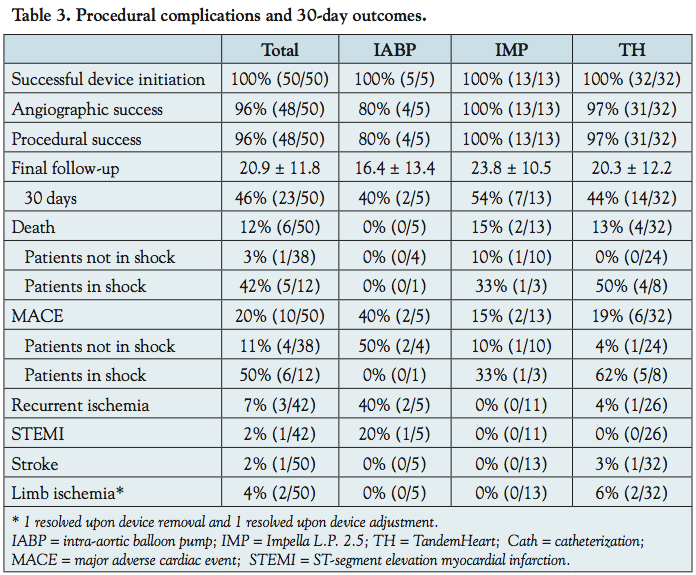 Outcomes. All devices were initiated successfully and without complication (Table 3). Despite complex coronary anatomy, angiographic success was achieved in 48 of 50 cases (96%). Procedural success was also 96%.
Outcomes. All devices were initiated successfully and without complication (Table 3). Despite complex coronary anatomy, angiographic success was achieved in 48 of 50 cases (96%). Procedural success was also 96%.
In-hospital outcomes were documented for all patients and 30-day outcomes were available for 23 patients (46%). Mean duration of follow-up was 20.9 ± 11.8 days. Overall, death occurred in 12% of patients, but was highly dependent on the presence of shock. Of the 38 patients not in shock, death occurred in 1 (2.6%), recurrent ischemia in 3 (8%), and stroke in 0 (0%), composing a total MACE rate of 11% (4 of 38). Of the 12 patients in shock, death occurred in 5 (42%), recurrent ischemia in 0%, and stroke in 1 (9%), totaling a MACE rate of 50% (6 of 12). The patient without shock who died was 87 years old, with a recent MI, pneumonia, severe mitral regurgitation, and peripheral arterial disease.
One patient was noted to have confusion and left-sided weakness in the recovery area following a TandemHeart-assisted HR-PCI. She was diagnosed with an embolic stroke attributed to severe aortic atheroma that was probably dislodged by the 0.035˝ wire or guide catheter, unrelated to the TandemHeart device. Each of the 2 instances of limb ischemia resolved upon device removal (1) or device adjustment (1). There were no episodes of limb ischemia causing persistent symptoms or requiring intervention. Two patients treated with the TandemHeart experienced transient hypotension during the procedure: one briefly required norepinephrine, the other occurred during the first attempt at transeptal puncture and resolved after brief cardiopulmonary resuscitation (second transeptal puncture attempt successful).
Device-related characteristics. PLVADs were used for a mean of 141 ± 325 minutes. The PLVAD was removed in <120 minutes in 88% of all cases, including in 92% of Impella and in 94% of TandemHeart cases. Twenty-nine of 32 TandemHeart cases (91%) utilized the 15 Fr catheter and the remainder used the 17 Fr catheter. The TandemHeart device was operated with a mean of 5864 ± 895 revolutions/min, which generated a mean device output of 3.1 ± 0.8 L/min. In 91–92% of the Impella and TandemHeart cases, hemostasis was achieved using the Perclose device (Abbott Vascular) with the “preclose” technique.
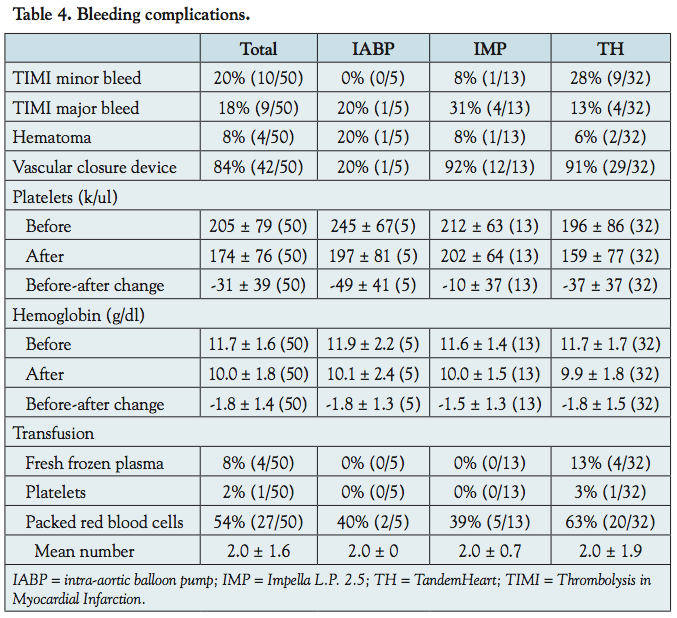 Bleeding complications. Bleeding complications were associated with all 3 PLVAD (Table 4). TIMI major bleeding occurred in 9 of 50 patients (18%). TIMI minor bleeding occurred in 10 of 50 patients (20%), primarily in the TandemHeart cases. There were no episodes of retroperitoneal bleeding or femoral artery bleeding that required surgical repair.
Bleeding complications. Bleeding complications were associated with all 3 PLVAD (Table 4). TIMI major bleeding occurred in 9 of 50 patients (18%). TIMI minor bleeding occurred in 10 of 50 patients (20%), primarily in the TandemHeart cases. There were no episodes of retroperitoneal bleeding or femoral artery bleeding that required surgical repair.
Hemoglobin and platelets decreased in each PLVAD group. Patients in each PLVAD group received transfusions of packed red blood cells, especially patients with the TandemHeart, who occasionally also received other blood products.
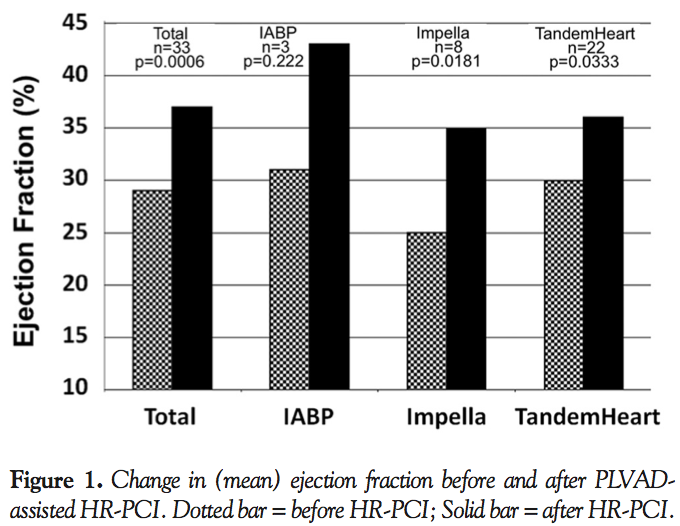
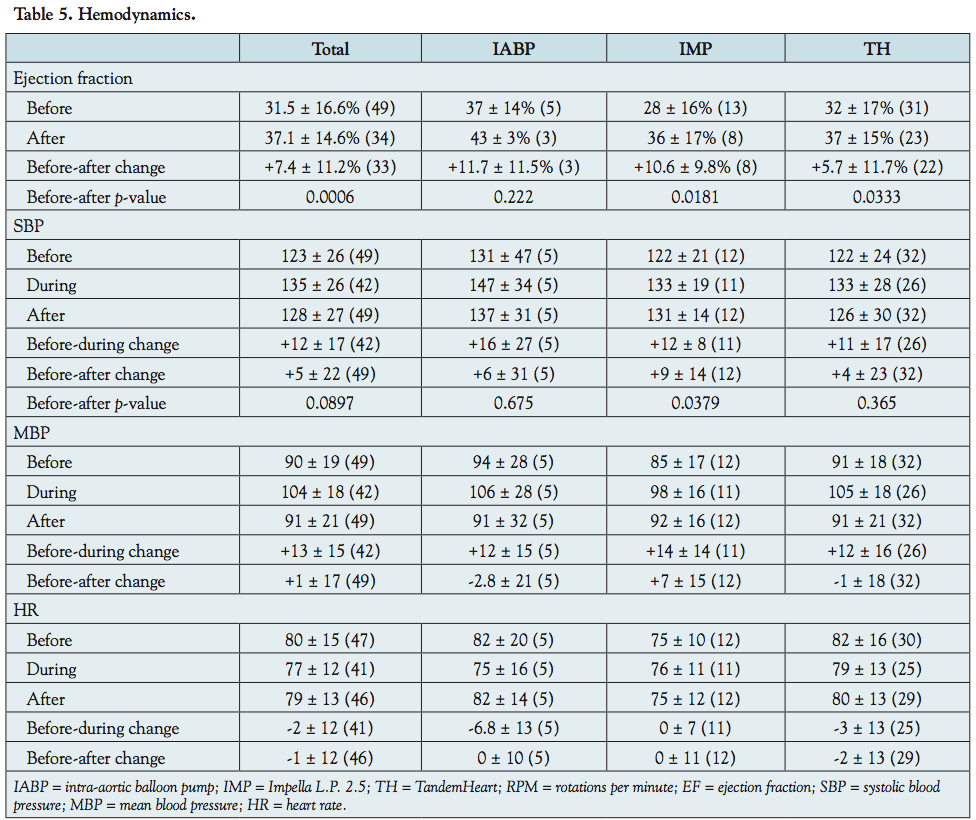 Hemodynamics. EF increased from before to after the HR-PCI in the total cohort (+7.4 ± 11.2%; p = 0.0006), and in each group (IABP, +11.7 ± 11.5%, p = 0.222, p-value limited by n = 3; Impella, +10.6 ± 9.8%, p = 0.0181; TandemHeart, +5.7 ± 11.7%, p = 0.0333), as shown in Table 5 and Figure 1. In addition, systolic blood pressure increased in each group from before to after device use and this change was significant for the Impella group (+9 ± 14 mmHg; p = 0.0379). Both systolic and mean blood pressure increased during device use with each PLVAD. Heart rate did not change appreciably during or after device use. Excluding the patients on vasopressors, the hemodynamic data was essentially unchanged (data not reported).
Hemodynamics. EF increased from before to after the HR-PCI in the total cohort (+7.4 ± 11.2%; p = 0.0006), and in each group (IABP, +11.7 ± 11.5%, p = 0.222, p-value limited by n = 3; Impella, +10.6 ± 9.8%, p = 0.0181; TandemHeart, +5.7 ± 11.7%, p = 0.0333), as shown in Table 5 and Figure 1. In addition, systolic blood pressure increased in each group from before to after device use and this change was significant for the Impella group (+9 ± 14 mmHg; p = 0.0379). Both systolic and mean blood pressure increased during device use with each PLVAD. Heart rate did not change appreciably during or after device use. Excluding the patients on vasopressors, the hemodynamic data was essentially unchanged (data not reported).
Discussion
 This study demonstrates that the Impella and TandemHeart devices can be used in patients with complex coronary disease and severe left ventricular dysfunction with minimal complications and with high rates of angiographic and procedural success. Also, a rapid increase in systolic blood pressure and EF after device removal suggests a protective effect of PLVADs on the myocardium.
This study demonstrates that the Impella and TandemHeart devices can be used in patients with complex coronary disease and severe left ventricular dysfunction with minimal complications and with high rates of angiographic and procedural success. Also, a rapid increase in systolic blood pressure and EF after device removal suggests a protective effect of PLVADs on the myocardium.
The ideal hemodynamic support device for prophylactic use in patients undergoing HR-PCI would be easy to insert, quick to initiate, provide reliable support, improve clinical outcomes, and would not impose a high risk of device-related complications. In this series, all 13 Impellas and 32 TandemHearts were initiated successfully, with only 1 transient device-related complication. Moreover, angiographic success was achieved in 96% of patients despite challenging coronary anatomy.
Major complications were minimal. Consistent with other reports,11 the TandemHeart device caused limb ischemia in 2 cases (6%), but each case resolved upon device adjustment or removal. One TandemHeart patient suffered a stroke, which was probably related to aortic atheroma, not the TandemHeart device. Also consistent with other reports,11 the Impella and TandemHeart devices increased the incidence of bleeding compared with the IABP. Blood transfusions were administered in approximately 40% of the IABP and Impella patients and in 63% of the TandemHeart patients. There were no major bleeding-related complications other than blood transfusions.
Use of the IABP during HR-PCI reduces the incidence of major procedural complications4-7 and tended to reduce the incidence of in-hospital MACE in a retrospective analysis,5 but not in a randomized trial.7 Hemodynamic support from the IABP, however, is limited and may be inadequate in patients with intraprocedural circulatory collapse or with significant arrhythmias. The IABP does not directly pump blood, but decreases afterload so that the left ventricle pumps more efficiently. IABPs increase cardiac output by a maximum of approximately 0.5 L/min.11 The Impella device provides up to 2.5 L/min of output, but requires intrinsic left ventricular function and blood flow to operate. In contrast, the TandemHeart device pumps blood independent of left ventricular function and can provide cardiac output up to 3.5–5 L/min (15–17 Fr). Compared with the IABP, the Impella and TandemHeart devices provide more cardiac output and blood pressure support,8-11 reduce cardiac work load more due to better unloading of the left ventricle,13 and decrease pulmonary capillary wedge pressure and pulmonary arterial pressure.8-11 In a study of 11 patients undergoing HR-PCI, the Impella device increased aortic pressure, coronary perfusion pressure, and hyperemic flow velocity, and decreased microvascular resistance.13 The Impella device also improved systemic microcirculation in patients with STEMI.20
The hemodynamic effects of these 3 devices may have beneficial effects on the myocardium, especially in the setting of MI. In animal studies, infarct size was reduced with the IABP and was reduced further with the TandemHeart.21,22 In this study, systolic blood pressure and EF improved shortly after the HR-PCI was concluded and the device removed. The PLVADs may have benefitted the myocardium, reflected in the improved EFs during the myocardial stunning period. The absolute increase in EF of 7.4% becomes more meaningful considering it correlates with a relative increase of 24% from the low baseline EF. This finding of a rapidly improved EF supports the utility of HR-PCI with PLVAD in patients with severely reduced EFs.
Initially, it appears that the death rate in this report is very high, but this is because patients with shock were included in this study, whereas they were excluded from other reports on patients undergoing HR-PCI.4-7,12,13,15,18,19 The death rate of 2.6% in patients without shock is in accordance with the literature (1–10%).4,5,7,12,18,19 The one patient without shock who died would have been excluded from other reports because of pneumonia, severe mitral regurgitation, and severe peripheral vascular disease.
A recent, retrospective comparison of the new PLVADs during HR-PCI reported no differences between the Impella and TandemHeart groups in short-term or long-term clinical outcomes.19 For patients undergoing HR-PCI in whom a PLVAD is indicated, it is the general approach in our institution to use an IABP in patients with the least severe disease, an Impella for patients at greater risk, and a TandemHeart for patients with the highest risk of circulatory collapse. IABPs may be inadequate if the patient were to suffer a major coronary complication that caused severe left ventricular collapse; the Impella and TandemHeart devices may improve survival in this setting. No study has yet reported a mortality benefit with PLVADs in patients undergoing HR-PCI. A study is warranted to analyze a tiered approach to PLVAD device selection, which theoretically maximizes hemodynamic support with the Impella and TandemHeart devices in those patients with the most severe disease while minimizing the risk of complications in patients who are lower risk by utilizing IABPs.
Limitations. This report is limited as a single-center, retrospective analysis. Selection bias precludes comparisons between groups (the TandemHeart group had the highest risk). Clinical follow-up was not available for some patients after hospital discharge, so final follow-up was at a mean of 20.9 ± 11.8 days. Consequently, 30-day event rates may be higher. However, in-hospital and 30-day event rates were nearly identical in 2 large series of patients undergoing HR-PCI.4,5 Vasopressors may have influenced the hemodynamic data. However, the hemodynamics were nearly identical when patients on vasopressors were excluded.
Conclusion
In summary, in this series of patients who underwent HR-PCI with Impella and TandemHeart support, angiographic success was high and acute complications were minimal. PLVADs may have beneficial effects on the myocardium during HR-PCI, especially in the setting of MI. A tiered approach in which patients with the least, intermediate, and highest risk of circulatory collapse are treated with an IABP, an Impella, or a TandemHeart device, respectively, warrants further investigation.
References
- Anderson HV, Shaw RE, Brindis RG, et al. A contemporary overview of percutaneous coronary interventions. The American College of Cardiology-National Cardiovascular Data Registry (ACC-NCDR). J Am Coll Cardiol. 2002;39(7):1096-1103.
- Williams DO, Holubkov R, Yeh W, et al. Percutaneous coronary intervention in the current era compared with 1985-1986: the National Heart, Lung, and Blood Institute Registries. Circulation. 2000;102(24):2945-2951.
- Smith SC Jr, Feldman TE, Hirshfeld JW Jr, et al. ACC/AHA/SCAI 2005 guideline update for percutaneous coronary intervention: a report of the American College of Cardiology/American Heart Association Task Force on Practice Guidelines (ACC/AHA/SCAI writing committee to update the 2001 guidelines for percutaneous coronary intervention). J Am Coll Cardiol. 2006;47(1):E1-E121.
- Mishra S, Chu WW, Torguson R, et al. Role of prophylactic intra-aortic balloon pump in high-risk patients undergoing percutaneous coronary intervention. Am J Cardiol. 2006;98(5):608-612.
- Briguori C, Airoldi F, Chieffo A, et al. Elective versus provisional intra-aortic balloon pumping in unprotected left main stenting. Am Heart J. 2006;152(3):565-572.
- Anwar A, Mooney MR, Stertzer SH, et al. Intra-aortic balloon counterpulsation support for elective coronary angioplasty in the setting of poor left ventricular function: a two center experience. J Invasive Cardiol. 1990;2(4):175-180.
- Perera D, Stables R, Thomas M, et al. Elective intra-aortic balloon counterpulsation during high-risk percutaneous coronary intervention: a randomized controlled trial. JAMA. 2010;304(8):867-874.
- Thiele H, Sick P, Boudriot E, et al. Randomized comparison of intra-aortic balloon support with a percutaneous left ventricular assist device in patients with revascularized acute myocardial infarction complicated by cardiogenic shock. Eur Heart J. 2005;26(13):1276-1283. Epub 2005 Feb 25.
- Burkhoff D, Cohen H, Brunckhorst C, O’Neill WW. A randomized multicenter clinical study to evaluate the safety and efficacy of the TandemHeart percutaneous ventricular assist device versus conventional therapy with intra-aortic balloon pumping for treatment of cardiogenic shock. Am Heart J. 2006;152(3):469.e1-468.e8.
- Seyfarth M, Sibbing D, Bauer I, et al. A randomized clinical trial to evaluate the safety and efficacy of a percutaneous left ventricular assist device versus intra-aortic balloon pumping for treatment of cardiogenic shock caused by myocardial infarction. J Am Coll Cardiol. 2008;52(19):1584-1588.
- Cheng JM, den Uil CA, Hoeks SE, et al. Percutaneous left ventricular assist devices vs. intra-aortic balloon pump counterpulsation for treatment of cardiogenic shock: a meta-analysis of controlled trials. Eur Heart J. 2009;30(17):2102-2108. Epub 2009 July 18.
- Dixon SR, Henriques JP, Mauri L, et al. A prospective feasibility trial investigating the use of the Impella 2.5 system in patients undergoing high-risk percutaneous coronary intervention (the PROTECT I trial): initial U.S. experience. JACC Cardiovasc Interv. 2009;2(2):91-96.
- Remmelink M, Sjauw KD, Henriques JP, et al. Effects of left ventricular unloading by Impella recover LP2.5 on coronary hemodynamics. Catheter Cardiovasc Interv. 2007;70(4):532-537.
- Henriques JP, Remmelink M, Baan J Jr, et al. Safety and feasibility of elective high-risk percutaneous coronary intervention procedures with left ventricular support of the Impella Recover LP 2.5. Am J Cardiol. 2006;97(7):990-992. Epub 2006 Feb 13.
- Aragon J, Lee MS, Kar S, Makkar RR. Percutaneous left ventricular assist device: “TandemHeart” for high-risk coronary intervention. Catheter Cardiovasc Interv. 2005;65(3):346-352.
- Thomas JL, Al-Ameri H, Economides C, et al. Use of a percutaneous left ventricular assist device for high-risk cardiac interventions and cardiogenic shock. J Invasive Cardiol. 2010;22(8):360-364.
- Kar B, Adkins LE, Civitello AB, et al. Clinical experience with the TandemHeart percutaneous ventricular assist device. Tex Heart Inst J. 2006;33(2):111-115.
- Sjauw KD, Konorza T, Erbel R, et al. Supported high-risk percutaneous coronary intervention with the Impella 2.5 device the Europella registry. J Am Coll Cardiol. 2009;54(25):2430-2434.
- Kovacic JC, Nguyen HT, Karajgikar R, et al. The Impella recover 2.5 and TandemHeart ventricular assist devices are safe and associated with equivalent clinical outcomes in patients undergoing high-risk percutaneous coronary intervention. Catheter Cardiovasc Interv. 2011 Jan 13. Epub ahead of print.
- Lam K, Sjauw KD, Henriques JP, Ince C, de Mol BA. Improved microcirculation in patients with an acute ST-elevation myocardial infarction treated with the Impella LP2.5 percutaneous left ventricular assist device. Clin Res Cardiol. 2009;98(5):311-318.
- Fonger JD, Zhou Y, Matsuura H, Aldea GS, Shemin RJ. Enhanced preservation of acutely ischemic myocardium with transseptal left ventricular assist. Ann Thorac Surg. 1994;57(3):570-575.
- Laschinger JC, Grossi EA, Cunningham JN Jr, et al. Adjunctive left ventricular unloading during myocardial reperfusion plays a major role in minimizing myocardial infarct size. J Thorac Cardiovasc Surg. 1985;90(1):80-85.
____________________________________________
From 1the Heart Institute and 2the Department of Cardiology, Good Samaritan Hospital, Los Angeles, California, and 3the Department of Internal Medicine, Division of Cardiovascular Medicine, Keck School of Medicine at the University of Southern California, Los Angeles, California.
Disclosure: The authors have completed and returned the ICMJE Form for Disclosure of Potential Conflicts of Interest. The authors report no conflicts of interest regarding the content herein.
Manuscript submitted May 23, 2011, provisional acceptance given July 6, 2011, final version accepted July 26, 2011.
Address for correspondence: Bryan Schwartz, MD, Heart Institute, Good Samaritan Hospital, 1225 Wilshire Blvd., Los Angeles, CA 90017-2395. Email: bschwartz15@hotmail.com





