

Coronary to Pulmonary Artery Fistulas: An Incidental Finding with Challenging Therapeutic Options
ABSTRACT: We report the incidental finding of 2 coronary to pulmonary artery fistulas observed at coronary angiography performed in a 48-year-old man presenting with acute inferior ST-elevation myocardial infarction (STEMI). Coronary angiography revealed an acute thrombotic occlusion of the mid segment of the right coronary artery (RCA), which was treated with thromboaspiration and bare-metal stenting. Significant stenoses of the left anterior descending (LAD) and left circumflex (LCX) arteries were also observed during angiography, as well as the presence of 2 large coronary to pulmonary artery fistulas, one originating from the proximal LAD and the other from the ostial RCA. The clinical evolution was uneventful and the patient underwent successful coronary bypass grafting of the LAD and LCX lesions associated with ligation of the coronary artery fistulas 6 weeks later.
The fact that 2 large coronary to pulmonary artery fistulas were observed during an acute coronary syndrome in a previously asymptomatic patient with extensive coronary artery disease is of particular interest, because it allowed early surgical correction of this rare inborn coronary anomaly before the development of late and irreversible left ventricular dysfunction.
J INVASIVE CARDIOL 2011;23:E177–E180
Key words: bilateral coronary to pulmonary artery fistulas, acute myocardial infarction
_________________________________________
Coronary artery fistula is a connection between one or more coronary arteries and a cardiac chamber or great vessel, bypassing the myocardial capillary bed.1 Coronary artery fistulas are rare abnormalities first described by Krauss et al in 1865,2 and they constitute < 15% of all coronary artery anomalies, with an estimated incidence of < 1% in angiographic series.3 This anomaly is usually single, but fistulas arising from 2 coronary arteries occur in approximately 5% of all coronary artery fistula cases.4 When congenital, they result from abnormal embryological development of the myocardial vascular system. When acquired, they are seen after trauma, endovascular procedures (i.e., coronary angiography, endomyocardial biopsy, and pacemaker implantation) or cardiac transplantation. Patients with coronary artery fistula may become symptomatic secondary to myocardial ischemia or heart failure.5,6 In this setting, surgical or endovascular closure may be proposed as a safe and efficient treatment.7,8 When discovered as an incidental finding during coronary angiography or echocardiography, treatment of coronary artery fistulas remains debated.3,9
We report a case of double coronary to pulmonary artery fistula discovered during emergent coronary angiography for acute ST-elevation myocardial infarction (STEMI) in a patient with no prior cardiac symptoms. The different therapeutic options are discussed.
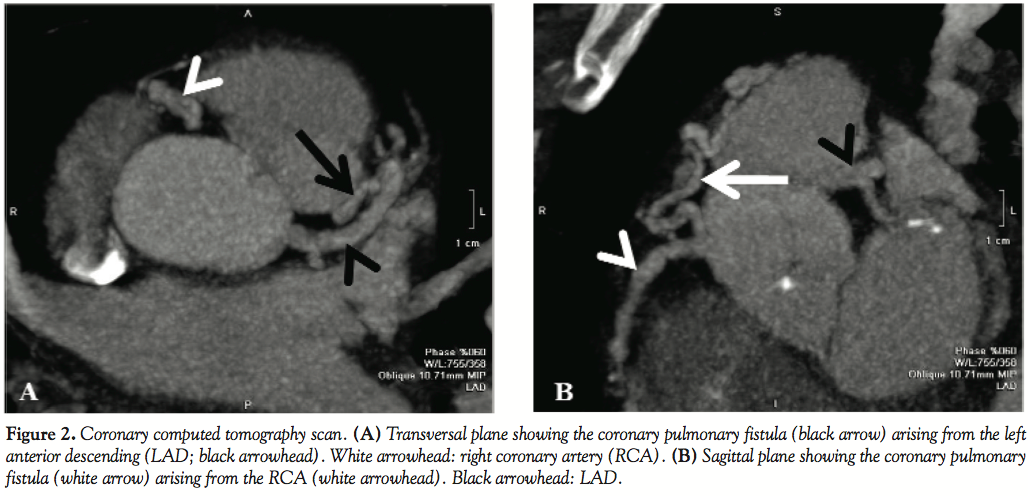
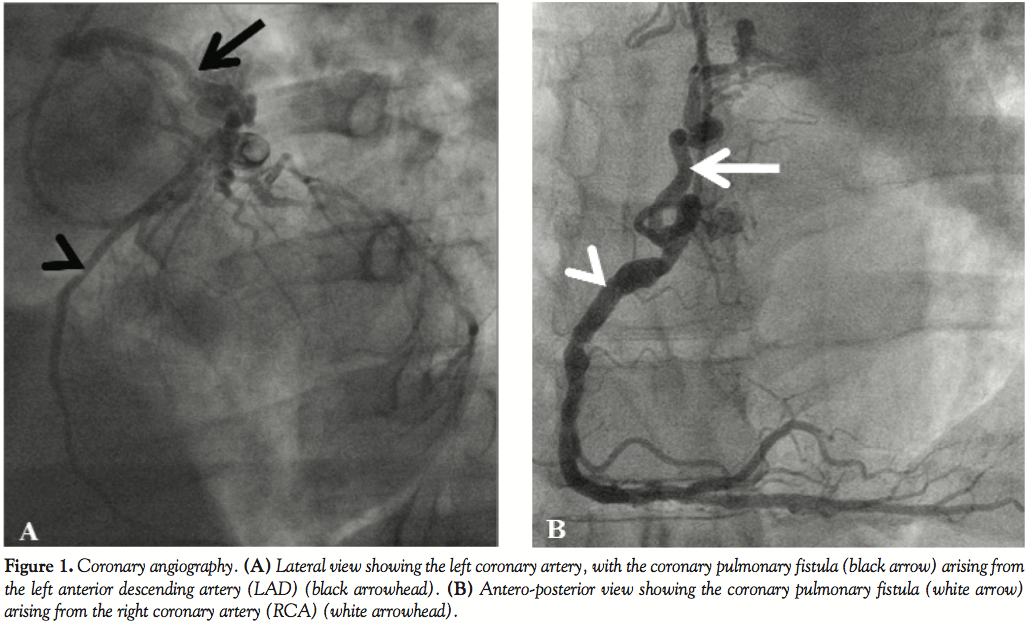 Case Report. A 48-year-old man with no past medical history was transferred to our institution with an acute inferior STEMI. He was directly transferred from the ambulance to the catheterization laboratory for a primary percutaneous coronary intervention (PCI). The coronary angiography revealed an acute thrombotic occlusion of the mid-portion of the RCA, which could be successfully treated by thromboaspiration and bare-metal stent placement. The coronary angiography also showed significant stenoses of the LAD and LCX arteries. Moreover, it revealed the presence of 2 large coronary artery fistulas, one originating from the proximal LAD (Figure 1A) and the other from the ostial RCA (Figure 1B), both draining into the pulmonary trunk at 2 different, but close, entry sites. In the acute setting, no right heart catheterization was performed. The fistulas were subsequently imaged by coronary computed tomography (CT) scan (Figures 2A–2B) and transthoracic echocardiography (TTE; Figure 3).The creatinine kinase level reached a maximum of 1,500 U/L, and the TTE performed before discharge showed a preserved ejection fraction (60%) with a mild inferior hypokinesis, normal size of the right atrium and right ventricle, and no pulmonary hypertension. After consideration of anatomy and extension of the remaining coronary stenoses and according to the wishes of the patient, the surgical treatment option (coronary bypass grafting and fistula ligation) was chosen. The clinical evolution was uneventful, and the patient was discharged on dual-antiplatelet therapy for 1 month. Following discontinuation of clopidogrel, the patient underwent coronary bypass grafting procedure for the LAD and LCX stenoses and ligation of the coronary artery fistulas 6 weeks after stent implantation.
Case Report. A 48-year-old man with no past medical history was transferred to our institution with an acute inferior STEMI. He was directly transferred from the ambulance to the catheterization laboratory for a primary percutaneous coronary intervention (PCI). The coronary angiography revealed an acute thrombotic occlusion of the mid-portion of the RCA, which could be successfully treated by thromboaspiration and bare-metal stent placement. The coronary angiography also showed significant stenoses of the LAD and LCX arteries. Moreover, it revealed the presence of 2 large coronary artery fistulas, one originating from the proximal LAD (Figure 1A) and the other from the ostial RCA (Figure 1B), both draining into the pulmonary trunk at 2 different, but close, entry sites. In the acute setting, no right heart catheterization was performed. The fistulas were subsequently imaged by coronary computed tomography (CT) scan (Figures 2A–2B) and transthoracic echocardiography (TTE; Figure 3).The creatinine kinase level reached a maximum of 1,500 U/L, and the TTE performed before discharge showed a preserved ejection fraction (60%) with a mild inferior hypokinesis, normal size of the right atrium and right ventricle, and no pulmonary hypertension. After consideration of anatomy and extension of the remaining coronary stenoses and according to the wishes of the patient, the surgical treatment option (coronary bypass grafting and fistula ligation) was chosen. The clinical evolution was uneventful, and the patient was discharged on dual-antiplatelet therapy for 1 month. Following discontinuation of clopidogrel, the patient underwent coronary bypass grafting procedure for the LAD and LCX stenoses and ligation of the coronary artery fistulas 6 weeks after stent implantation.
 The surgical intervention began with direct ligation of the right coronary to pulmonary artery fistula close to the RCA’s ostium. Under extracorporeal circulation, the left internal mammary artery was then implanted on the LAD and a venous graft on the LCX, and finally the draining orifice of the left coronary to pulmonary artery fistula at the pulmonary trunk level was sutured (pulmonary aortotomy). The intervention was uneventful, with a total aortic cross-clamping of 71 minutes and a total extracorporeal circulation time of 1 hour and 34 minutes. No complications were observed in the post-operative phase and the patient was discharged 8 days after surgery to join a rehabilitation program.
The surgical intervention began with direct ligation of the right coronary to pulmonary artery fistula close to the RCA’s ostium. Under extracorporeal circulation, the left internal mammary artery was then implanted on the LAD and a venous graft on the LCX, and finally the draining orifice of the left coronary to pulmonary artery fistula at the pulmonary trunk level was sutured (pulmonary aortotomy). The intervention was uneventful, with a total aortic cross-clamping of 71 minutes and a total extracorporeal circulation time of 1 hour and 34 minutes. No complications were observed in the post-operative phase and the patient was discharged 8 days after surgery to join a rehabilitation program.
 Discussion. Coronary artery fistulas are occasionally observed during coronary angiography (0.1–0.8%),3 and are reported to arise from the RCA in about 60% of cases, from the left coronary artery (LAD or LCX) in about 35% of cases, or bilaterally in about 5% of cases.4,10 They most often drain into the right heart chambers (i.e., > 66% into the right ventricle or right atrium, 17% into the pulmonary trunk), causing left-to-right shunting. The volume of the shunt, and thereby the risk of symptom development, depends on the size of the fistula and on the difference between the systemic and terminating vascular/chamber resistance. If sizable, this left-to-right shunt may lead to right ventricular volume overload and dysfunction already in childhood.1
Discussion. Coronary artery fistulas are occasionally observed during coronary angiography (0.1–0.8%),3 and are reported to arise from the RCA in about 60% of cases, from the left coronary artery (LAD or LCX) in about 35% of cases, or bilaterally in about 5% of cases.4,10 They most often drain into the right heart chambers (i.e., > 66% into the right ventricle or right atrium, 17% into the pulmonary trunk), causing left-to-right shunting. The volume of the shunt, and thereby the risk of symptom development, depends on the size of the fistula and on the difference between the systemic and terminating vascular/chamber resistance. If sizable, this left-to-right shunt may lead to right ventricular volume overload and dysfunction already in childhood.1
As in our case, the presence of multiple fistulas is more frequently associated with drainage directly into the pulmonary trunk (56% versus 17% if single fistula),11,12 thus avoiding right chamber volume overload, but potentially leading to an isolated left ventricular dysfunction. In this particular setting, estimation of the hemodynamic relevance of the shunt may be difficult, because shunt assessment and precocious left ventricular overload evaluation remain challenging without invasive cardiac catheterization measurements. Indeed, the invasive staged oxygen measurements in all cardiac chambers during cardiac catheterization, in the aorta and in both the inferior and superior vena cavas, remains the gold-standard exam for an accurate left-to-right shunt evaluation, especially where other noninvasive shunt evaluations are inconclusive.
In our case, we did not perform any invasive shunt measurements because of the acute STEMI presentation. Since the patient was to undergo surgical revascularization regardless of the degree of shunting, we decided not to perform a second cardiac catheterization for diagnostic purposes. Had the indication for fistula closure exclusively depended on the degree of shunting, a second cardiac catheterization or a cardiac MRI would have been valuable.13 Contrary to what was observed in our case, most coronary artery fistulas, especially those discovered in adult patients and particularly those draining into the pulmonary trunk, are small with no significant shunting.14 Inherent to those characteristics, these tiny fistulas rarely give rise to symptoms and thus seldom require intervention. Their anatomic characterization can be completed by several imaging methods, such as echocardiography (especially in children), cardiac magnetic resonance imaging, or CT-scan.15,16
In the presence of significant shunting, the clinical presentation varies from congestive heart failure due to volume overload, more often observed among infants and children, to angina or exertional dyspnea, which more frequently occur among adults. The pathophysiology of angina development in coronary to pulmonary artery fistulas may be attributed to a “coronary artery steal” phenomenon, which, especially in the presence of significant atherosclerosis, favors blood flow through the less resistant vascular system (i.e., the fistula). When becoming symptomatic, coronary artery fistulas are associated with poor outcomes,9 and in order to prevent complications, closure is recommended at all ages.7 Surgical ligation of coronary artery fistulas is the first-line treatment because it is safe and effective, and is associated with an acceptable peri-procedural mortality rate (1.4%) and a virtually 100% regression of symptoms. This complete symptom regression was reported in several series, despite residual shunting observed at follow-up in up to 25%.8,17
Since its first report in 1983,18 catheter-based closure of coronary artery fistulas has progressively become an attractive alternative to surgery. Accordingly, numerous series have suggested satisfactory results in terms of safety and efficacy.8,19–21 In a recent report reviewing 45 transcatheter closures of coronary artery fistulas, Armsby et al reported a 2% peri-procedural mortality (i.e., due to coil embolization in the LAD with subsequent occlusion).8 In this series, no further late complications or late deaths were reported at 1 year, and complete closure of the fistulas was observed in 91% of analyzed patients.
In the case of a percutaneous approach, different closure techniques may be used, including different types of coils, detachable balloons, umbrella devices, covered stents, and dedicated vascular plugs.8,14,21 Due to scarcity of the reported cases, the disparity of follow-up imaging and the lack of randomized trials, it is difficult to confront efficacy and safety of surgical versus endovascular closure techniques. However, the early and late complication rates, and especially the efficacy in terms of closure rate, of both techniques seem comparable. It should nevertheless be underlined that certain anatomic conditions of the fistula may contraindicate a catheter-based approach (i.e., extreme tortuosity of the vessels, multiple draining sites, coronary branches at the site of the fistula).8
Finally, it remains a source of debate whether asymptomatic patients should undergo fistula closure, especially given that spontaneous closure of the fistula is described. Different authors reporting on follow-up of such asymptomatic patients recommend different strategies, from elective closure regardless of symptoms,17 especially in childhood, to conservative management,9 particularly in presence of small fistulas, which is most often the case when they drain into the pulmonary trunk.8
In our case, both fistulas were considered asymptomatic, because the patient presented with acute myocardial infarction with no apparent relation to his coronary to pulmonary artery fistulas, and especially because the patient did not mention any prior symptoms that could be correlated to the presence of this double fistula. Because triple-vessel disease and 2 large coronary to pulmonary artery fistulas were present, we decided to treat the occluded RCA with implantation of 2 bare-metal stents, thus allowing complete surgical revascularization associated with fistula ligation 6 weeks later (i.e., after clopidogrel discontinuation).
Conclusion. The presence of 2 large coronary to pulmonary artery fistulas, observed for the first time during an acute coronary syndrome in a young asymptomatic patient with extensive coronary artery disease, is of particular interest and has, to the best of our knowledge, only been reported once.22 The need for a subsequent bypass grafting facilitated the decision on how to manage this inborn condition before development of late and irreversible left ventricular dysfunction.
References
- Levin DC, Fellows KE, Abrams HL. Hemodynamically significant primary anomalies of the coronary arteries. Angiographic aspects. Circulation 1978;58:25–34.
- Dodge-Khatami A, Mavroudis C, Backer CL. Congenital heart surgery nomenclature and database project: Anomalies of the coronary arteries. Ann Thorac Surg 2000;69:S270–S297.
- Angelini P, Velasco JA, Flamm S. Coronary anomalies: Incidence, pathophysiology, and clinical relevance. Circulation 2002;105:2449–2454.
- Renard C, Chivot C, Jarry G, et al. Communicating bilateral coronary artery to pulmonary artery fistula with aneurysm in asymptomatic patient: Successful conservative management with selective coil embolization of the aneurysm. Int J Cardiol 2010 Mar 9 (Epub ahead of print).
- Raju MG, Goyal SK, Punnam SR, et al. Coronary artery fistula: A case series with review of the literature. J Cardiol 2009;53:467–472.
- Guo H, You B, Lee JD. Dilated cardiomyopathy caused by a coronary-pulmonary fistula treated successfully with coil embolization. Circ J 2006;70:1223–1225.
- Balanescu S, Sangiorgi G, Castelvecchio S, et al. Coronary artery fistulas: Clinical consequences and methods of closure. A literature review. Ital Heart J 2001;2:669–676.
- Armsby LR, Keane JF, Sherwood MC, et al. Management of coronary artery fistulae. Patient selection and results of transcatheter closure. J Am Coll Cardiol 2002;39:1026–1032.
- Sherwood MC, Rockenmacher S, Colan SD, Geva T. Prognostic significance of clinically silent coronary artery fistulas. Am J Cardiol 1999;83:407–411.
- Hoffman J. Congenital anomalies of the coronary vessels and the aortic root. In: Heart Disease in Infants, Children and Adolescents, 5th edition. Emmanoulides G, Reimenschneider TA, Allen HD, Gutgesell HP (eds). Williams and Wilkins, Baltimore 1995: p. 780.
- Baim DS, Kline H, Silverman JF. Bilateral coronary artery — Pulmonary artery fistulas. Report of five cases and review of the literature. Circulation 1982;65:810–815.
- Levy Praschker BG, Rama A, Gandjbakhch I, Pavie A. Congenital bilateral coronary artery to pulmonary artery fistulas associated with left main trunk stenosis. Interact Cardiovasc Thorac Surg 2008;7:360–361.
- Devos DG, Kilner PJ. Calculations of cardiovascular shunts and regurgitation using magnetic resonance ventricular volume and aortic and pulmonary flow measurements. Eur Radiol 2010;20:410–421.
- Gowda RM, Vasavada BC, Khan IA. Coronary artery fistulas: Clinical and therapeutic considerations. Int J Cardiol 2006;107:7–10.
- Taoka Y, Nomura M, Harada M, et al. Coronary-pulmonary artery fistulae depicted by multiplanar reconstruction using magnetic resonance imaging. Jpn Circ J 1998;62:455–457.
- Zeina AR, Blinder J, Rosenschein U, Barmeir E. Coronary-pulmonary artery fistula diagnosed by multidetector computed tomography. Postgrad Med J 2006;82:E15.
- Mavroudis C, Backer CL, Rocchini AP, et al. Coronary artery fistulas in infants and children: A surgical review and discussion of coil embolization. Ann Thorac Surg 1997;63:1235–1242.
- Reidy JF, Sowton E, Ross DN. Transcatheter occlusion of coronary to bronchial anastomosis by detachable balloon combined with coronary angioplasty at same procedure. Br Heart J 1983;49:284–287.
- Reidy JF, Anjos RT, Qureshi SA, et al. Transcatheter embolization in the treatment of coronary artery fistulas. J Am Coll Cardiol 1991;18:187–192.
- Perry SB, Rome J, Keane JF, et al. Transcatheter closure of coronary artery fistulas. J Am Coll Cardiol 1992;20:205–209.
- Qureshi SA, Tynan M. Catheter closure of coronary artery fistulas. J Interv Cardiol 2001;14:299–307.
- Aeba R, Ishikura Y, Odagiri S, et al. A simultaneous operation of closure of multiple congenital coronary artery-pulmonary artery fistulas and aortocoronary bypass grafting — A case report [in Japanese]. Nippon Kyobu Geka Gakkai Zasshi 1989;37:555–560.
_________________________________________
From the Cardiology Division, University Hospital, Geneva, Switzerland.
The authors report no conflicts of interest regarding the content herein.
Manuscript submitted October 26, 2010, provisional acceptance given November 24, 2010, final version accepted April 18, 2011.
Address for correspondence: Robert Francis Bonvini, MD, Division of Cardiology, University Hospital of Geneva, 4, rue Gabrielle-Perret-Gentil, 1211 Geneva 14/Switzerland. Email: Robert.Bonvini@hcuge.ch







