

Chronic Total Occlusion Intervention: A Novel Antegrade Guidewire Probing Technique
Abstract: We reported a case of successful recanalization of a left anterior descending (LAD) artery chronic total occlusion (CTO) with ‘antegrade guidewire probing technique.’ After we mistakenly deployed a stent at the proximal LAD from left main (LM) into a diagonal branch across the mid LAD, this mid LAD CTO became further jailed under the stent. Antegrade wiring of this CTO lesion became exceptionally difficult. After several unsuccessful attempts with different guidewires and interventional techniques, we placed a retrograde microcatheter into the CTO lesion with its tip just situated at the stent strut. An antegrade guidewire supported by another microcatheter was targeted at the tip of the retrograde microcatheter and successfully crossed the CTO lesion. The LAD was successfully recanalized. This technique appeared to be feasible and safe to facilitate antegrade wire crossing of the CTO lesion.
J INVASIVE CARDIOL 2012;24(5):242-244
Key words: percutaneous coronary intervention, chronic total occlusion, retrograde, collaterals
_____________________________________________
The use of retrograde approach has increased the successful rate of CTO coronary intervention.1 Despite the development of new intervention techniques including parallel wire, kissing wire, knuckle wire, CART, or reverse CART,1,2 wire crossing of CTO lesions remains technically challenging and time consuming. We describe an antegrade guidewire probing technique by advancing the antegrade wire into the retrograde microcatheter already placed in the CTO lesion.
Case Report
 A 44-year-old male presented with acute coronary syndrome. He had been having exertional chest discomfort for a few months but developed rest angina on the day of admission. His only coronary risk factor was chronic smoking. His electrocardiogram on admission showed 4 mm ST depression over leads II, II, aVF, V2-V6, and ST elevation over aVR. Troponin T level was 4.71 µg/L (normal <0.03 µg/L). Echocardiogram revealed satisfactory left ventricular function with ejection fraction of 55%. Initial coronary angiogram was mistakenly interpreted
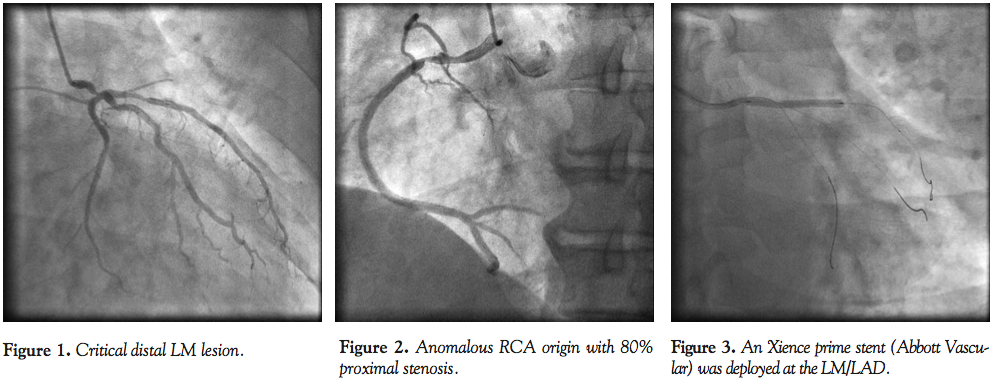
A 44-year-old male presented with acute coronary syndrome. He had been having exertional chest discomfort for a few months but developed rest angina on the day of admission. His only coronary risk factor was chronic smoking. His electrocardiogram on admission showed 4 mm ST depression over leads II, II, aVF, V2-V6, and ST elevation over aVR. Troponin T level was 4.71 µg/L (normal <0.03 µg/L). Echocardiogram revealed satisfactory left ventricular function with ejection fraction of 55%. Initial coronary angiogram was mistakenly interpreted 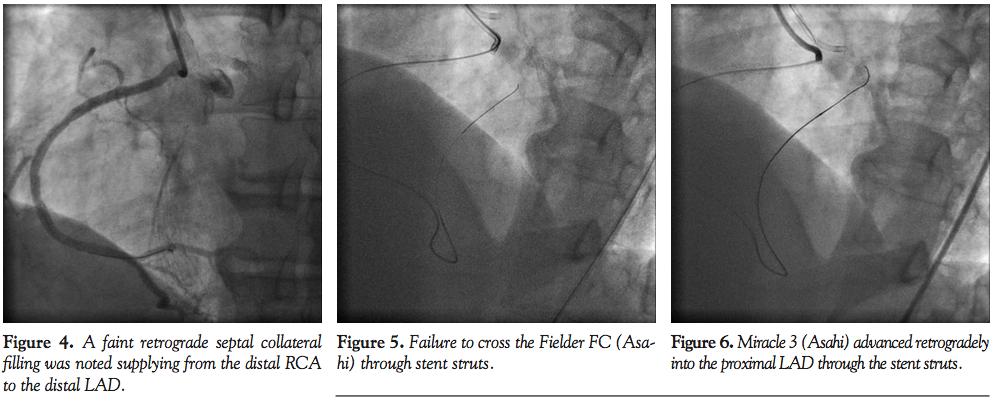 as a focal 80% stenosis at the distal left main (LM). The right coronary artery (RCA) had an anomalous origin arising from the anterior aortic wall and there was a 70% stenosis at its mid segment (Figures 1 and 2). The patient refused coronary artery bypass grafting as the treatment of choice. We then proceeded to coronary angioplasty. A 6 Fr Judkins left 3.5 guiding catheter (Medtronic) was placed in the left coronary artery (LCA) via the right radial approach. LAD, left circumflex (LCX) and ramus arteries were wired with
as a focal 80% stenosis at the distal left main (LM). The right coronary artery (RCA) had an anomalous origin arising from the anterior aortic wall and there was a 70% stenosis at its mid segment (Figures 1 and 2). The patient refused coronary artery bypass grafting as the treatment of choice. We then proceeded to coronary angioplasty. A 6 Fr Judkins left 3.5 guiding catheter (Medtronic) was placed in the left coronary artery (LCA) via the right radial approach. LAD, left circumflex (LCX) and ramus arteries were wired with  RunthroughNS Floppy (Terumo), Rinato (Asahi), and Balanced Middleweight Universal (Abbott Vascular), respectively. A 2.5 x 15 mm balloon was delivered to dilate along the LM and LAD. After intravascular ultrasound (IVUS) examination, a 3.0 x 33 mm Xience Prime stent (Abbott Vascular) was deployed from LM into LAD across the ramus and LCX. Ramus wire was removed (Figure 3). LCX wire was removed and re-crossed. The stent was postdilated with a 3.5 x 15 mm non-compliant balloon. Finally, kissing balloon inflation was performed with a 3.5 x 15 mm balloon and a 2.5 x 15 mm balloon inflated at 12 atm and 10 atm, respectively. A 6 Fr Judkins Right 4 guiding catheter was used to engage the anomalous RCA. A 3.5 x 23 mm Xience V stent (Abbott Vascular) was deployed at the mid RCA lesion and postdilated with a 4.0 non-compliant balloon. However, a faint retrograde septal collateral filling was noted going from distal RCA to distal LAD (Figure 4). What was thought to be the distal LAD was in fact a large diagonal branch. Effectively, we had deployed our stent across a LAD CTO from LM to diagonal. Therefore, the original LAD CTO became jailed under this stent. Multiple attempts were made to wire the totally occluded lesion antegradely, but were unsuccessful. Retrograde approach was attempted. The right femoral artery was accessed. A 6 Fr Amplatz left 1.0 guiding catheter (Medtronic) was introduced through the right femoral sheath and engaged into the RCA. The septal collateral was wired with Fielder FC (Asahi) supported by Corsair (Asahi) catheter. The Fielder FC was successfully advanced into the mid LAD but was unable to advance into the proximal LAD through the stent struts (Figure 5). It was then switched to Miracle 3 wire (Asahi) which successfully punctured through the jailed LAD stent strut and could reach the proximal LAD (Figure 6). The Corsair was tracked into the CTO (Figure 7). However, only the very tip of the Corsair could get through the stent strut and was stopped from advancing any further by the stent struts. Without enough support from the Corsair, we failed to externalize any of the retrograde guidewire despite sequentially changing to Fielder FC, Whisper (Abbott Vascular) and Rotawire (Boston Scientific). We decided at this stage to attempt a new method. The retrograde wire was withdrawn back into the Corsair and PT2 (Boston Scientific) was used as the antegrade wire to probe at the tip of the Corsair, which was situated just distal to the LAD stent strut. This antegrade wire probing technique was successful (Figures 8 and 9). The PT2 was manipulated into the Corsair. The retrograde system was removed and the PT2 was further advanced into the distal LAD (Figure 10). It was very difficult to track a balloon through the LAD stent strut into the mid LAD. A 1.25 mm balloon could cross the stent strut and was dilated up to 12 atm. But when we upsized the balloon to 1.5 mm, the balloon ruptured, causing extensive dissection with intramural hematoma down the mid
RunthroughNS Floppy (Terumo), Rinato (Asahi), and Balanced Middleweight Universal (Abbott Vascular), respectively. A 2.5 x 15 mm balloon was delivered to dilate along the LM and LAD. After intravascular ultrasound (IVUS) examination, a 3.0 x 33 mm Xience Prime stent (Abbott Vascular) was deployed from LM into LAD across the ramus and LCX. Ramus wire was removed (Figure 3). LCX wire was removed and re-crossed. The stent was postdilated with a 3.5 x 15 mm non-compliant balloon. Finally, kissing balloon inflation was performed with a 3.5 x 15 mm balloon and a 2.5 x 15 mm balloon inflated at 12 atm and 10 atm, respectively. A 6 Fr Judkins Right 4 guiding catheter was used to engage the anomalous RCA. A 3.5 x 23 mm Xience V stent (Abbott Vascular) was deployed at the mid RCA lesion and postdilated with a 4.0 non-compliant balloon. However, a faint retrograde septal collateral filling was noted going from distal RCA to distal LAD (Figure 4). What was thought to be the distal LAD was in fact a large diagonal branch. Effectively, we had deployed our stent across a LAD CTO from LM to diagonal. Therefore, the original LAD CTO became jailed under this stent. Multiple attempts were made to wire the totally occluded lesion antegradely, but were unsuccessful. Retrograde approach was attempted. The right femoral artery was accessed. A 6 Fr Amplatz left 1.0 guiding catheter (Medtronic) was introduced through the right femoral sheath and engaged into the RCA. The septal collateral was wired with Fielder FC (Asahi) supported by Corsair (Asahi) catheter. The Fielder FC was successfully advanced into the mid LAD but was unable to advance into the proximal LAD through the stent struts (Figure 5). It was then switched to Miracle 3 wire (Asahi) which successfully punctured through the jailed LAD stent strut and could reach the proximal LAD (Figure 6). The Corsair was tracked into the CTO (Figure 7). However, only the very tip of the Corsair could get through the stent strut and was stopped from advancing any further by the stent struts. Without enough support from the Corsair, we failed to externalize any of the retrograde guidewire despite sequentially changing to Fielder FC, Whisper (Abbott Vascular) and Rotawire (Boston Scientific). We decided at this stage to attempt a new method. The retrograde wire was withdrawn back into the Corsair and PT2 (Boston Scientific) was used as the antegrade wire to probe at the tip of the Corsair, which was situated just distal to the LAD stent strut. This antegrade wire probing technique was successful (Figures 8 and 9). The PT2 was manipulated into the Corsair. The retrograde system was removed and the PT2 was further advanced into the distal LAD (Figure 10). It was very difficult to track a balloon through the LAD stent strut into the mid LAD. A 1.25 mm balloon could cross the stent strut and was dilated up to 12 atm. But when we upsized the balloon to 1.5 mm, the balloon ruptured, causing extensive dissection with intramural hematoma down the mid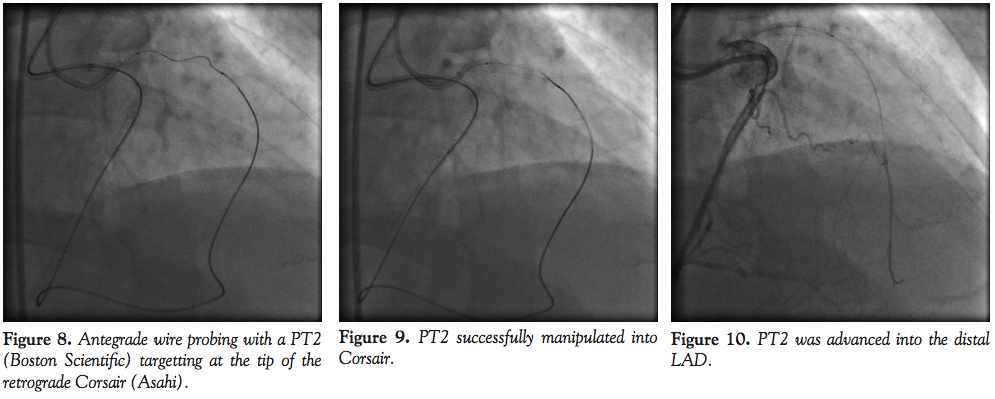 and distal LAD (Figure 11). We performed prolonged balloon angioplasty with a 2.0 mm balloon, resulting in TIMI 2 antegrade flow (Figure 12). Because of the extensive dissection and hematoma, true vessel size and lesion length could not be estimated from the angiogram alone. We also attempted to pass the Eagle Eye IVUS catheter (Volcano) to check the distal reference diameter and define
and distal LAD (Figure 11). We performed prolonged balloon angioplasty with a 2.0 mm balloon, resulting in TIMI 2 antegrade flow (Figure 12). Because of the extensive dissection and hematoma, true vessel size and lesion length could not be estimated from the angiogram alone. We also attempted to pass the Eagle Eye IVUS catheter (Volcano) to check the distal reference diameter and define 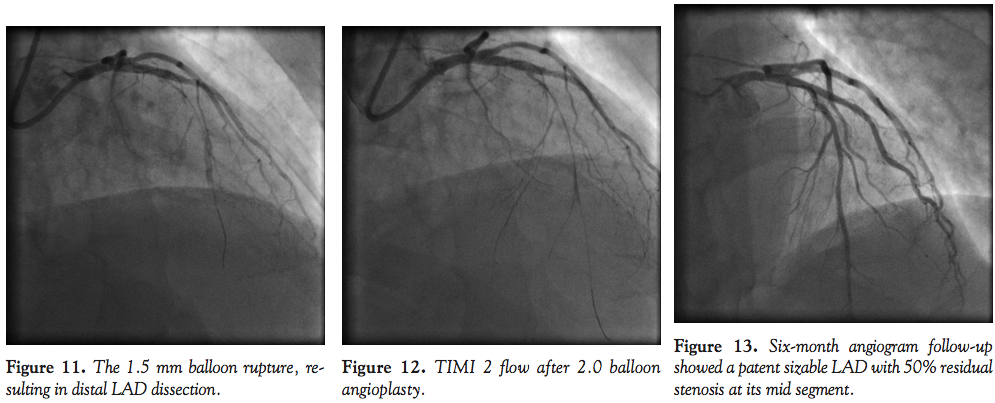 the extent of disease and dissection, but this IVUS catheter could not get through the stent strut. The procedure was adjourned and the LAD was left with TIMI 2 flow. The patient reported much improvement in terms of his angina status and repeat angiogram at 6 months showed patent LAD stent with resolution and healing of the hematoma and dissection. There was a focal 50%-60% stenosis in the mid LAD just distal to the dilated LAD stent strut (Figure 13). The patient did not have further chest pain after the first procedure and did not want to have another intervention to treat his LAD.
the extent of disease and dissection, but this IVUS catheter could not get through the stent strut. The procedure was adjourned and the LAD was left with TIMI 2 flow. The patient reported much improvement in terms of his angina status and repeat angiogram at 6 months showed patent LAD stent with resolution and healing of the hematoma and dissection. There was a focal 50%-60% stenosis in the mid LAD just distal to the dilated LAD stent strut (Figure 13). The patient did not have further chest pain after the first procedure and did not want to have another intervention to treat his LAD.
Discussion
Over the past decade, a number of important CTO interventional techniques and devices have been developed and have greatly improved the successful rate of CTO intervention. Yet, many of these techniques are still complex and highly dependant on the technique and competency of the operators. Occasionally, they may also induce major complications. For example, septal hematoma3,4 has been reported with the use of the CART technique. New techniques that are safe and easy to use should always be given consideration. In this case, we reported a novel method called antegrade wire probing technique, which seems to fulfill the need.
In this case, the intervention was iatrogenically made even more challenging due to the jailing of LAD CTO by the deployed stent. From the antegrade route, it has become almost impossible to wire through the stent strut blindly to get into the distal LAD. Collateral filling of the distal LAD could only go up to the mid to distal LAD segment so that it left no traces for the antegrade wire to aim at. Switching to the retrograde approach would then become a wise choice. In this case, septal channel crossing was easy with the Fielder FC wire supported by the Corsair microcatheter. However, the real difficulty set in when the tip of the Corsair was stuck by the LAD stent strut. We have been able to pass several retrograde wires into the antegrade guiding catheter, but were not able to externalize any of these wires as a result of the lack of further support from the Corsair. Added to the difficulty was that support from the retrograde guiding catheter was also poor due to the anomalous take-off of the RCA. The course of the antegrade guiding catheter from the radial route was also tortuous along the subclavian artery region. At this stage, several other techniques might also be considered to overcome the situation. Probably, the simplest approach would be the use of a designated wire for externalization, ie, the RG3 (Asahi). Unfortunately, this wire was not widely available across the globe. We might try to snare the retrograde guidewire from the antegrade guide to facilitate externalization. Or we could use a trapping balloon to trap the retrograde guidewire inside the antegrade guiding catheter to help advance the Corsair across the stent strut to the LM. However, the principle of “difficult in and difficult out” might apply here when it might not be possible to withdraw the Corsair back. Finally, we might exchange our Corsair with an over-the-wire balloon to dilate the stent strut and then track the balloon across the stent strut. This seemed to be a feasible method, although it involved a number of complicated steps. Our technique was worth trying at this stage. The antegrade wire could in fact be quite easily manipulated to probe for the mouth of the Corsair. Once the antegrade wire got into the Corsair, the rest of the procedure became very simple and standard. The beauty of this technique is that it is simple, fast, and safe. We can still move on to other more complicated techniques such as the above-mentioned ones if we fail to get the antegrade wire across. Similar techniques by using a microcatheter for guidewire crossing have been described in previous literature, but they were used in different scenerios.5-8 This antegrade guidewire probing technique is feasible and safe. It can be an alternative strategy for CTO intervention.
References
- Sianos G, Barlis P, Di Mario C, et al. European experience with the retrograde approach for the recanalisation of coronary artery chronic total occlusion. A report on behalf of the EuroCTO club. Eur Interv. 2008;4(1):84-92.
- Saito S. Different strategies of retrograde approach in coronary angioplasty for chronic total occlusion. Catheter Cardiovasc Interv. 2008;71(1):8-19.
- Kimura M, Katoh O, Tsuchikane E, et al. The efficacy of a bilateral approach for treating lesions with chronic total occlusions: the CART (controlled antegrade and retrograde subintimal tracking) registry. JACC Cardiovasc Interv. 2009;2(11):1135-1141.
- Matsumi J, Adachi K, Saito S. A unique complication of the retrograde approach in angioplasty for chronic total occlusion of the coronary artery. Catheter Cardiovasc Interv. 2008;72(3):371-378.
- Christ G, Glogar D. Successful recanalization of a chronic occluded left anterior descending coronary artery with a modification of the retrograde proximal true lumen puncture technique: the antegrade microcatheter probing technique. Catheter Cardiovasc Interv. 2009;73(2):272-275.
- Kim MH, Yu LH, Mitsudo K. A new retrograde wiring technique for chronic total occlusion. Catheter Cardiovasc Interv. 2010;75(1):117-119.
- Liu W, Wagatsuma K. A novel technique of chronic total occlusion retrograde wire crossing by wiring into the antegrade microcatheter. Catheter Cardiovasc Interv. 2010;76(6):847-849.
- Muramatsu T, Tsukahara R, Ito Y. “Rendezvous in coronary” technique with the retrograde approach for chronic total occlusion. J Invasive Cardiol. 2010;22(9):E179-E182.
_____________________________________________
From the Division of Cardiology, Department of Medicine and Geriatrics, United Christian Hospital, Hong Kong, People’s Republic of China.
Disclosure: The authors have completed and returned the ICMJE Form for Disclosure of Potential Conflicts of Interest. The authors report no conflicts of interest regarding the content herein.
Manuscript submitted September 19, 2011 and accepted October 11, 2011.
Address for correspondence: Dr Raymond Chi Yan Fung, MBBS, Division of Cardiology, Department of Medicine and Geriatrics, United Christian Hospital, 130 Hip Wo Street, Kwun Tong, Hong Kong, People’s Republic of China. Email: raymondfunghk@yahoo.com.hk





