

Antegrade Ballooning with Retrograde Approach for the Treatment of Long Restenotic Total Occlusion
ABSTRACT: A retrograde approach through collateral channels is thought to improve the success rate of percutaneous coronary intervention for chronic total coronary occlusion (CTO). Among CTO lesions, the in-stent chronic total reocclusion (ISR-CTO) is a subset with an unsatisfactory outcome despite repeated procedures. Various strategies and techniques are required to improve the success rate of this novel approach. We describe a case in which a long ISR-CTO was successfully recanalized by a drug-eluting balloon after antegrade ballooning of the proximal part of the lesion with retrograde wire crossing, and discuss the availability of this approach for the treatment of long ISR-CTO.
J INVASIVE CARDIOL 2011;23:E164–E167
Key words: balloon, chronic total occlusion, percutaneous coronary intervention, restenosis, retrograde approach
___________________________________________
Although the advent of drug-eluting stents (DES) has decreased the incidence of in-stent restenosis (ISR) with outstanding therapeutic effectiveness even in complex coronary lesions such as chronic total coronary occlusions (CTO),1–4 the percutaneous treatment of CTO remains one of the major challenges in interventional cardiology. However, the simultaneous development of various techniques has improved the success rate of percutaneous coronary intervention (PCI) for CTO. A retrograde approach through native collateral channels was recently proposed, and this technique is now considered to be one of the most promising current techniques for increasing the success rate of PCI for CTO.5,6
Another presentation of ISR is chronic total reocclusion within a stent (ISR-CTO), either as the result of a silent late thrombotic stent occlusion, or as the consequence of slow diffuse neointimal hyperplasia. The implantation of DES has recently been proposed as a therapeutic option for ISR,7 but the best approach to ISR-CTO is not well understood. These lesions represent a specific problem for intervention, because the technical success rate in reocclusive lesions is lower than in non-occluded ISR, and because PCI with DES requires extensive secondary coverage beyond the primary stented area, with potentially higher lesion recurrence and late stent thrombosis risk.2,8
We present a case of successful percutaneous treatment for a long lesion in ISR-CTO by using antegrade ballooning with retrograde approach similar to the reverse controlled antegrade and retrograde subintimal tracking (CART) technique that required the anchoring balloon technique to overcome the difficulty of retrograde wire catching and to reduce the burden of ultimate stent risk by using a drug-eluting balloon (DEB).
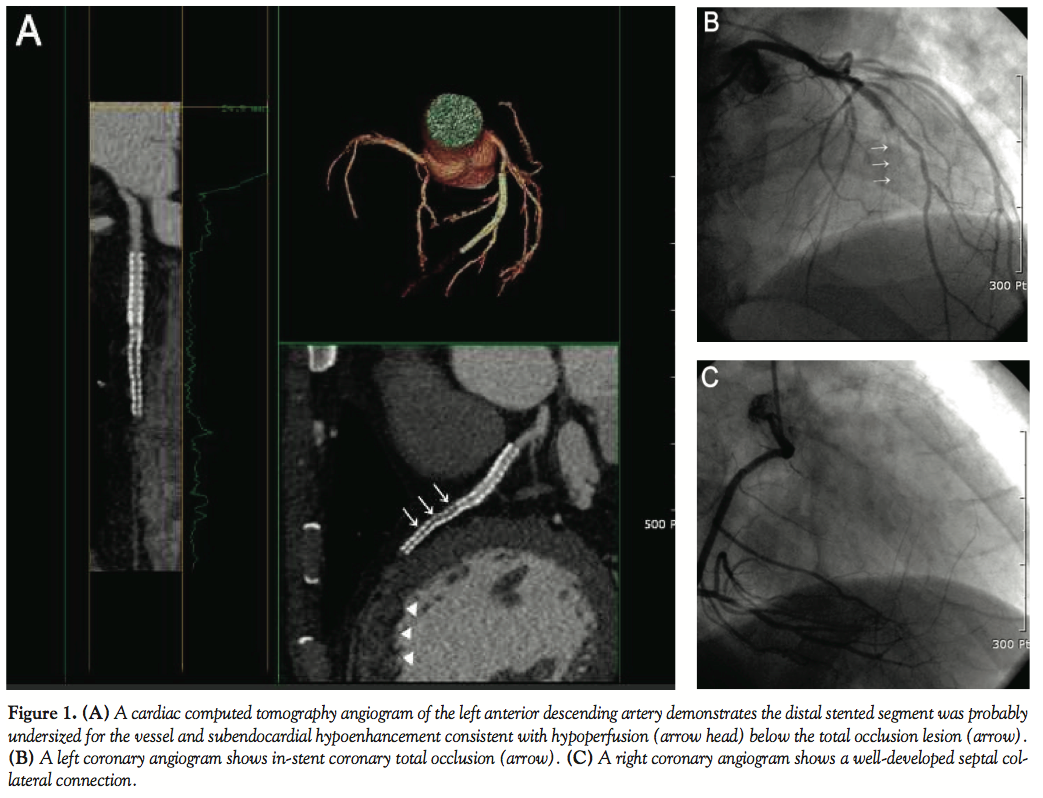 Case Report. A 56-year-old man presented at the outpatient cardiology clinic with atypical chest discomfort for several months. His coronary risk factors were hypertension and smoking. He had undergone PCI with 2 sirolimus-eluting Cypher stents (3.5 x 23 mm, 2.75 x 33 mm, consecutively; Cordis Corporation, Miami Lakes, Florida) from the proximal to the mid left anterior descending artery (LAD) in our hospital 6 years before. After intervention, he visited our laboratory regularly without chest pain and had a patent previous stent on a follow-up angiogram. The treadmill test showed ST-segment depression on stage IV. He underwent cardiac computed tomography angiography (CCTA) (Figure 1A) and repeat coronary angiography. A left coronary angiogram showed a Thrombolysis In Myocardial Infarction (TIMI) flow grade 0 with total reocclusion of the previous stent from the mid LAD (Figure 1B). The distal portion of the LAD was filled with a well-developed septal collateral connection from the posterior descending artery (PDA) on a right coronary angiogram (Figure 1C). Because the CTO had a large diagonal branch, well-visible collateral connection and a relatively long lesion, and because the approach to the septal connection was necessary to prevent harmful procedure complications such as tamponade, we planned the retrograde approach using this septal channel for PCI. The right coronary artery was first catheterized with a 7 Fr AL2 SH guiding catheter (Cordis Corporation) through the left femoral artery for retrograde access, and the left coronary artery with a 6 Fr XB 3.5 guiding catheter (Cordis Corporation) through the right radial artery. A 0.014˝, 2.8 Fr, 150 cm coronary microguide Corsair catheter (Asahi Intec, Nagoya, Japan) with a 0.014˝ Fielder FC wire (Asahi Intec) was used to negotitate the septal channel. After crossing over the septal collateral (Figure 2A), the Fielder FC wire for the retrograde approach was then changed sequentially to Miracle 3-g, Miracle 6-g and then Conquest-Pro 9-g wires (Asahi Intec) in order to cross the occluded site of the LAD. However, the hard wires could not be advanced further into the mid-LAD retrogradely. Miracle 6-g and 12-g wires were sequentially used for antegrade advancement. Since the wires could not pass the antegrade true lumen correctly, we decided to perform balloon dilatation in order to create a proximal intimal space of in-stent CTO by using 1.5 x 10 mm and 2.0 x 10 mm Sprinters (Medtronic Inc., Minneapolis, Minnesota) sequentially, with the reverse CART technique (Figure 2B). Thereafter, a retrograde Conquest-Pro 9-g wire (Asahi Intec) reached the proximal true lumen and could be advanced into the antegrade guiding catheter lumen. The retrograde wire was trapped there by a 2.5 x 15 mm Ryujin balloon (Terumo, Bangkok, Thailand), so that the microguide catheter could follow the left guiding catheter (Figures 2C and 2D). After the anchor balloon technique, the wire was changed to a 300 cm Rotawire (Boston Scientific Corporation, Natick, Massachusetts) that was inserted from the right retrograde guiding catheter to the left antegrade guiding catheter, forming a wire loop (retrograde wire externalization). From the guidewire tip outside the radial antegrade
Case Report. A 56-year-old man presented at the outpatient cardiology clinic with atypical chest discomfort for several months. His coronary risk factors were hypertension and smoking. He had undergone PCI with 2 sirolimus-eluting Cypher stents (3.5 x 23 mm, 2.75 x 33 mm, consecutively; Cordis Corporation, Miami Lakes, Florida) from the proximal to the mid left anterior descending artery (LAD) in our hospital 6 years before. After intervention, he visited our laboratory regularly without chest pain and had a patent previous stent on a follow-up angiogram. The treadmill test showed ST-segment depression on stage IV. He underwent cardiac computed tomography angiography (CCTA) (Figure 1A) and repeat coronary angiography. A left coronary angiogram showed a Thrombolysis In Myocardial Infarction (TIMI) flow grade 0 with total reocclusion of the previous stent from the mid LAD (Figure 1B). The distal portion of the LAD was filled with a well-developed septal collateral connection from the posterior descending artery (PDA) on a right coronary angiogram (Figure 1C). Because the CTO had a large diagonal branch, well-visible collateral connection and a relatively long lesion, and because the approach to the septal connection was necessary to prevent harmful procedure complications such as tamponade, we planned the retrograde approach using this septal channel for PCI. The right coronary artery was first catheterized with a 7 Fr AL2 SH guiding catheter (Cordis Corporation) through the left femoral artery for retrograde access, and the left coronary artery with a 6 Fr XB 3.5 guiding catheter (Cordis Corporation) through the right radial artery. A 0.014˝, 2.8 Fr, 150 cm coronary microguide Corsair catheter (Asahi Intec, Nagoya, Japan) with a 0.014˝ Fielder FC wire (Asahi Intec) was used to negotitate the septal channel. After crossing over the septal collateral (Figure 2A), the Fielder FC wire for the retrograde approach was then changed sequentially to Miracle 3-g, Miracle 6-g and then Conquest-Pro 9-g wires (Asahi Intec) in order to cross the occluded site of the LAD. However, the hard wires could not be advanced further into the mid-LAD retrogradely. Miracle 6-g and 12-g wires were sequentially used for antegrade advancement. Since the wires could not pass the antegrade true lumen correctly, we decided to perform balloon dilatation in order to create a proximal intimal space of in-stent CTO by using 1.5 x 10 mm and 2.0 x 10 mm Sprinters (Medtronic Inc., Minneapolis, Minnesota) sequentially, with the reverse CART technique (Figure 2B). Thereafter, a retrograde Conquest-Pro 9-g wire (Asahi Intec) reached the proximal true lumen and could be advanced into the antegrade guiding catheter lumen. The retrograde wire was trapped there by a 2.5 x 15 mm Ryujin balloon (Terumo, Bangkok, Thailand), so that the microguide catheter could follow the left guiding catheter (Figures 2C and 2D). After the anchor balloon technique, the wire was changed to a 300 cm Rotawire (Boston Scientific Corporation, Natick, Massachusetts) that was inserted from the right retrograde guiding catheter to the left antegrade guiding catheter, forming a wire loop (retrograde wire externalization). From the guidewire tip outside the radial antegrade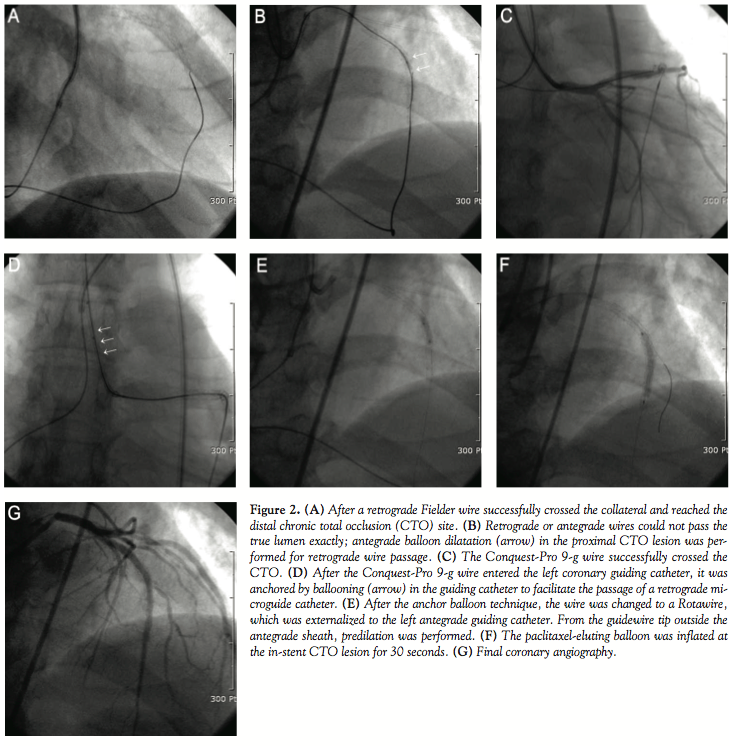 sheath, predilation was performed with 2.5 x 10 mm and 3.0 x 15 mm Ryujin balloons (Figure 2E). Then, a 3.0 x 30 mm paclitaxel-eluting SeQuent-Please ballooning (B. Braun, Melsungen, Germany) was performed at the in-stent CTO lesion (Figure 2F), and a 2.5 x 25 mm bare-metal Coroflex-blue stent (B. Braun) was placed at a de novo distal LAD lesion. The final angiogram showed successful revascularization without periprocedural complications (Figure 2G). A 6-month follow-up angiogram showed no restenosis, and the patient remained in a stable state during the 9 months of clinical follow-up.
sheath, predilation was performed with 2.5 x 10 mm and 3.0 x 15 mm Ryujin balloons (Figure 2E). Then, a 3.0 x 30 mm paclitaxel-eluting SeQuent-Please ballooning (B. Braun, Melsungen, Germany) was performed at the in-stent CTO lesion (Figure 2F), and a 2.5 x 25 mm bare-metal Coroflex-blue stent (B. Braun) was placed at a de novo distal LAD lesion. The final angiogram showed successful revascularization without periprocedural complications (Figure 2G). A 6-month follow-up angiogram showed no restenosis, and the patient remained in a stable state during the 9 months of clinical follow-up.
Discussion. In order to successfully perform percutaneous treatment of a long ISR-CTO in the LAD, we chose to pursue a strategy of applying the technique like reverse CART, using an anchoring balloon for the retrograde wire and externalization, and DEB at the in-stent lesion instead of secondary coverage of another stent.
It has been understood that ISR–CTO is relatively rare, particularly in this era of DES treatment. However, a recent study reported that ISR-CTO accounts for about 5–10% of all CTO lesions with little evidence for long-term success.9 The ISR-CTO lesion shows a lower primary technical success rate. This lesion is mainly composed of smooth muscle cells. Collagen and extracellular matrix constitute a homogenous tissue that becomes a more fibrous structure with a small amount of thrombus.10 Although the previous stent may allow for direct visualization of the anatomic course of the vessel, hard fibrous tissue can hinder correct wire advancement into the stent lumen and may cause wire penetration into the subintimal space through the stent strut. In case of lesion crossing, there is the need for extensive additional stenting to cover the reoccluded stent with sufficient overlap for the prevention of an edge recurrence.
In this case, procedural success was expected to be very difficult, because the lesion length of ISR-CTO was relatively long and because a large diagonal branch existed abeam of the proximal cut-off, which is one of the highest predictors of procedural failure. Non-invasive imaging modalities, such as CCTA, were useful in the evaluation of CTO prior to PCI. CCTA in our case not only showed the collateral supply in the distal vessel beyond the occlusion, but also distinctively revealed the proximal and distal ends of the occluded segment. Therefore, a prudent procedural strategy could be designed prior to PCI of ISR-CTO. CTO angioplasty has recently been developed and has improved the success rate of PCI. The retrograde approach through collateral channels has also shown a better outcome in CTO lesions in which the antegrade approach has been difficult due to unknown entry points, long lesions, and heavy calcium in the lesions.6,11 Compared to the antegrade approach, the retrograde approach requires a special step where the retrograde wire crosses the collateral channel and reaches the site distal to the CTO. Collaterals for retrograde access can be categorized as epicardial or septal channel. The epicardial collateral is very tortuous and has a long course in many cases. In addition, unlike the septal collateral, injury to the epicardial collateral can cause serious complications, such as pericardial tamponade or extensive target vessel ischemia in cases where the epicardial collateral constitutes a major feeding route for the target vessel.12,13 The reverse CART technique has potential disadvantages compared to other techniques for retrograde PCI of coronary CTO. The subintimal ballooning in the antegrade direction can provoke severe iatrogenic dissection, which may propagate and compromise the true lumen distal to the CTO site.6,14 However, in our case, flexible strategies and techniques contributed to procedural success. Because the lesion was ISR-CTO, it was necessary to avoid the chance of complications, such as myocardial ischemia related to retrograde ballooning through the collateral channel.
DES improves clinical and angiographic outcomes in patients with ISR.7 However, repeated DES can reduce the flexibility of the vessel and limit the repeatability of the procedure. Moreover, concerns have been raised about potentially higher lesion recurrence and late stent thrombosis risk. The best treatment of patients with DES ISR remains to be elucidated. A recent study has shown DEB to be superior to DES with respect to primary angiographic and clinical outcomes in the treatment of coronary ISR.15 Finally, we decided to use DEB to avoid an additional second layer of metal in the treatment of a long ISR-CTO.
This case suggests that diverse techniques can contribute to the successful recanalization of the ISR-CTO. However, strict case selection, improved devices and systematic approaches seem to be essential for this procedure due to the technical complexities accompanied by the potential risk of unexpected complications. More experience and refinement are required to generalize our novel approach.
References
- Stone GW, Colombo A, Teirstein PS, et al. Percutaneous recanalization of chronically occluded coronary arteries: Procedural techniques, devices, and results. Catheter Cardiovasc Interv 2005;66:217–236.
- Werner GS, Schwarz G, Prochnau D, et al. Paclitaxel-eluting stents for the treatment of chronic total coronary occlusions: A strategy of extensive lesion coverage with drug-eluting stents. Catheter Cardiovasc Interv 2006;67:1–9.
- Serruys PW, Morice M-C, Kappetein AP, et al. Percutaneous coronary intervention versus coronary artery bypass grafting for severe coronary artery disease. N Engl J Med 2009;360:961–972.
- De Felice F, Fiorilli R, Parma A, et al. 3-year clinical outcome of patients with chronic total occlusion treated with drug-eluting stents. J Am Coll Cardiol Interv 2009;2:1260–1265.
- Ozawa N. A new understanding of chronic total occlusion from a novel PCI technique that involves a retrograde approach to the right coronary artery via a septal branch and passing of the guidewire to a guiding catheter on the other side of lesion. Catheter Cardiovasc Interv 2006;68:907–913.
- Saito S. Different strategies of retrograde approach in coronary angioplasty for chronic total occlusion. Catheter Cardiovasc Interv 2008;71:8–19.
- Kastrati A, Mehilli J, von Beckerath N, et al. The ISAR-DESIRE study investigators. Sirolimus-eluting stent or paclitaxel-eluting stent versus balloon angioplasty for prevention of recurrences in patients with coronary in-stent restenosis: A randomized controlled trial. JAMA 2005;293:165–171.
- Lee CW, Kim SH, Suh J, et al. Long-term clinical outcomes after sirolimus-eluting stent implantation for treatment of restenosis within bare-metal versus drug-eluting stents. Catheter Cardiovasc Interv 2008;71:594–598.
- Werner GS, Moehlis H, Tischer K. Management of total restenotic occlusions. EuroIntervention 2009;5(Suppl D):D79–D83.
- Hoffman R, Mintz GS, Dussaillant GR, et al. Patterns and mechanisms of in-stent restenosis: A serial intravascular ultrasound study. Circulation 1996;94:1247–1254.
- Lee NH, Seo HS, Choi JH, et al. Recanalization strategy of retrograde angioplasty in patients with coronary chronic total occlusion — Analysis of 24 cases, focusing on technical aspects and complications. Int J Cardiol 2010;144:219–229. Epub 2009 May 6.
- Surmely JF, Katoh O, Tsuchikane E, et al. Coronary septal collaterals as an access for the retrograde approach in the percutaneous treatment of coronary chronic total occlusions. Catheter Cardiovasc Interv 2007;69:826–832.
- Werner GS, Ferrari M, Heinke S, et al. Angiographic assessment of collateral connections in comparison with invasively determined collateral function in chronic coronary occlusions. Circulation 2003;107:1972–1977.
- Suh J, Cho YH, Lee NH. Bail-out reverse controlled antegrade and retrograde subintimal tracking accomplished by multiple complications in coronary chronic total occlusion. J Invasive Cardiol 2008;20:E334–E337.
- Unverdorben M, Vallbracht C, Cremers B, et al. Paclitaxel-coated balloon catheter versus paclitaxel-coated stent for the treatment of coronary in-stent restenosis. Circulation 2009;119:2986–2994.
___________________________________________
From the Division of Cardiology, Department of Internal Medicine, SoonChunHyang University Bucheon Hospital, Bucheon, South Korea.
The authors report no conflicts of interest regarding the content herein.
Manuscript submitted September 29, 2010 and accepted November 22, 2010.
Address for correspondence: Prof. Nae-Hee Lee, SoonChunHyang University, Division of Cardiology, Department of Internal Medicine, Bucheon, 420-767 South Korea. Email: naeheelee@paran.com







