

Ablation of Hypertrophic Septum Using Radiofrequency Energy — An Alternative for Gradient Reduction in Patient With Hypertrophic Obstructive Cardiomyopathy?
ABSTRACT: Introduction. Alcohol septal ablation and surgical myectomy represent accepted therapeutic options for treatment of symptomatic patients with hypertrophic obstructive cardiomyopathy. Long-term experience with radiofrequency ablation of arrhythmogenic substrates raised a question if this technique might be effective for left ventricular outflow tract (LVOT) gradient reduction. Case report. We report on a 63-year-old patient with recurrence of symptoms 1 year after alcohol septal ablation (ASA) leading originally to a significant reduction of both symptoms and gradient. Due to a new increase of gradient in the LVOT up to 200 mm Hg with corresponding worsening of symptoms and due to refusal of surgical myectomy by the patient, endocardial radiofrequency ablation of the septal hypertrophy (ERASH) was indicated. Radiofrequency ablation was performed in the LVOT using irrigated-tip ablation catheter; the target site was identified using intracardiac echocardiography and electroanatomical CARTO mapping. ERASH caused an immediate gradient reduction due to hypokinesis of the ablated septum. At 2-month follow-up exam, significant clinical improvement was observed, together with persistent gradient reduction assessed with Doppler echocardiography. Echocardiography and magnetic resonance revealed persistent septal hypokinesis and slight thinning of the ablated region. Conclusion. Septal ablation using radiofrequency energy may be a promising alternative or adjunct to the treatment of hypertrophic obstructive cardiomyopathy. Intracardiac echocardiography and electroanatomical CARTO mapping enable exact lesion placement and preservation of atrioventricular conduction.
J INVASIVE CARDIOL 2013;25(6):E128-E132
Key words: hypertrophic cardiomyopathy, septal ablation, radiofrequency ablation, electroanatomical mapping, echocardiography, magnetic resonance
_____________________________________________
Symptoms occurring as a consequence of obstruction in hypertrophic cardiomyopathy are effectively improved by reducing the obstructive septal hypertrophy in the left ventricular outflow tract (LVOT). To reach this, surgical septal myectomy and alcohol septal ablation (ASA) are largely accepted therapeutic options.1-3 However, applicability and results of the latter method are crucially dependent on the individual anatomy of the septal arteries and in some patients with hypertrophic obstructive cardiomyopathy usage of ASA may therefore be problematic.4 Since the main therapeutic goal in hypertrophic obstructive cardiomyopathy is gradient reduction, another strategy might be theoretically effective. Based on the experience with catheter ablation of arrhythmogenic substrates, it is well known that application of radiofrequency energy is able to create extensive and deep tissue coagulation necrosis5,6 with subsequent scarring of the ablated region. Therefore, endocardial radiofrequency ablation of the septal hypertrophy (ERASH) has been recently suggested as a possible alternative to reduce LVOT obstruction in patients with hypertrophic cardiomyopathy.7,8
 Case Report. A 63-year-old man was sent to a cardiologist because of his progressive dyspnea (New York Heart Association [NYHA] functional class 3), angina (Canadian Cardiovascular Society [CCS] class 3) and signs of hypertrophy on the surface electrocardiogram (ECG). Patient history was non-significant other than permanent anticoagulation because of proven Leiden mutation.
Case Report. A 63-year-old man was sent to a cardiologist because of his progressive dyspnea (New York Heart Association [NYHA] functional class 3), angina (Canadian Cardiovascular Society [CCS] class 3) and signs of hypertrophy on the surface electrocardiogram (ECG). Patient history was non-significant other than permanent anticoagulation because of proven Leiden mutation.
 Echocardiographic examination demonstrated significant hypertrophy of the left ventricle, with posterior wall/interventricular septum thickness of 17/22 mm. In addition, it showed displacement and hypertrophy of the papillary muscles, supranormal ejection fraction, and no regional hypokinesis. Furthermore, septal anterior movement (SAM) was detected, with mild end-systolic mitral regurgitation caused by SAM phenomenon and displacement of the papillary muscles. Continuous-wave (CW) Doppler echocardiography revealed presence of significant LVOT obstruction with a peak gradient reaching 93 mm Hg at rest and 135 mm Hg during the Valsalva maneuver (Figure 1).
Echocardiographic examination demonstrated significant hypertrophy of the left ventricle, with posterior wall/interventricular septum thickness of 17/22 mm. In addition, it showed displacement and hypertrophy of the papillary muscles, supranormal ejection fraction, and no regional hypokinesis. Furthermore, septal anterior movement (SAM) was detected, with mild end-systolic mitral regurgitation caused by SAM phenomenon and displacement of the papillary muscles. Continuous-wave (CW) Doppler echocardiography revealed presence of significant LVOT obstruction with a peak gradient reaching 93 mm Hg at rest and 135 mm Hg during the Valsalva maneuver (Figure 1).
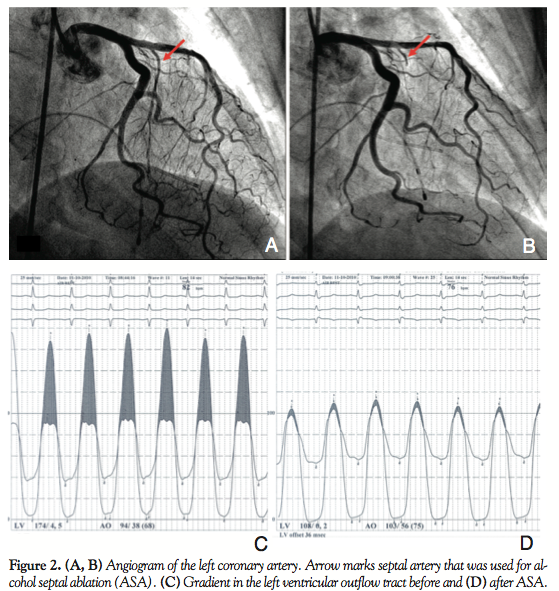
 Therapy with beta-blockers was started; however, it didn’t lead to any significant subjective improvement. Therefore, angiography was indicated 6 months later with normal findings in both coronary arteries and a suitable septal artery was identified. ASA was subsequently performed using 1 mL of 96% alcohol with an immediate gradient reduction during the procedure (the invasive peak gradient decreases from 60 mm Hg to 10 mm Hg) (Figure 2). ASA led to development of right bundle branch block that remained stable and no atrioventricular conduction block developed during follow-up. Echocardiography confirmed optimal location of the ablation lesion with greater reduction in the midventricular part of the septum. Due to persistence of the SAM phenomenon, the patient was kept on beta-blockers. Decrease of the LVOT gradient after ASA led to a significant improvement of symptoms: angina disappeared completely and only mild dyspnea (NYHA class 1-2) was present during the first 6 months.
Therapy with beta-blockers was started; however, it didn’t lead to any significant subjective improvement. Therefore, angiography was indicated 6 months later with normal findings in both coronary arteries and a suitable septal artery was identified. ASA was subsequently performed using 1 mL of 96% alcohol with an immediate gradient reduction during the procedure (the invasive peak gradient decreases from 60 mm Hg to 10 mm Hg) (Figure 2). ASA led to development of right bundle branch block that remained stable and no atrioventricular conduction block developed during follow-up. Echocardiography confirmed optimal location of the ablation lesion with greater reduction in the midventricular part of the septum. Due to persistence of the SAM phenomenon, the patient was kept on beta-blockers. Decrease of the LVOT gradient after ASA led to a significant improvement of symptoms: angina disappeared completely and only mild dyspnea (NYHA class 1-2) was present during the first 6 months.
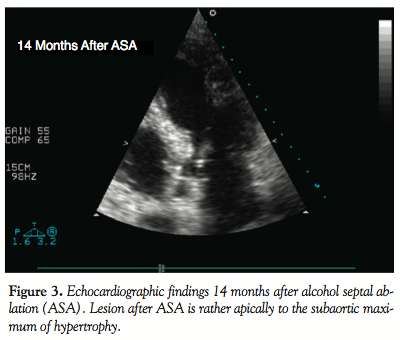
However, 1 year later, the patient presented with a new worsening of dyspnea and manifestation of angina with slow progression to NYHA class 3 and CCS class 2 again. Transthoracic echocardiography performed 14 months after ASA revealed significant subaortic obstruction with SAM. Based on CW Doppler, the subaortic gradient was 26 mm Hg at rest, but it increased up to 200 mm Hg after nitrate provocation. The ASA lesion was smaller and located slightly distally to the subaortic maximum (Figure 3). The location of the septal bulge with regard to the arterial supply didn’t allow performance of a new ASA and performance of surgical myectomy was therefore discussed with the patient. However, the patient refused surgical treatment and therefore ERASH was offered to the patient as an option. After providing detailed information about the procedure, its potential risks, and possible complications, the patient gave and signed informed consent.
 Endocardial radiofrequency ablation of septal hypertrophy. At the beginning of the procedure, a coronary angiography was repeated. No other suitable branch was found. Left ventricular and aortic pressures were then recorded using 5 Fr pigtail catheter and pullback technique. The peak left ventricular and aortic pressures reached 203 mm Hg and 104 mm Hg, respectively.
Endocardial radiofrequency ablation of septal hypertrophy. At the beginning of the procedure, a coronary angiography was repeated. No other suitable branch was found. Left ventricular and aortic pressures were then recorded using 5 Fr pigtail catheter and pullback technique. The peak left ventricular and aortic pressures reached 203 mm Hg and 104 mm Hg, respectively.
A 5 Fr pacing catheter was introduced to mark His bundle location and to perform right ventricular pacing if necessary (Prucka mapping system; General Electric). Through the contralateral femoral vein, the intracardiac echocardiographic probe (Acuson AcuNav diagnostic ultrasound catheter; Siemens) was inserted and placed in the right atrium to display LVOT and septal bulge location. For radiofrequency (RF) ablation, an irrigated tip catheter was used (Navistar Thermocool; Biosense Webster). The cooling pump was programmed to release 30ml/h of saline during ablation (Cool Flow Irrigation Pump, Biosense Webster). The ablation generator (Stockert EPU Shuttle; Biosense Webster) was programmed to the manually controlled ablation mode with delivery of 30 W for 90 seconds. The applied power was manually increased when necessary.
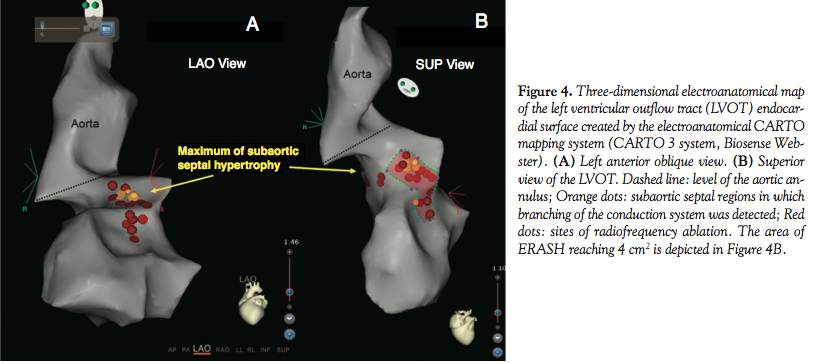
A retrograde transaortic approach was used for the ablation catheter placement. A dose of 5000 IU of heparin was administered and activated clotting time (ACT) was monitored. The catheter was navigated to the region of the septal bulge using both fluoroscopy and later under control of intracardiac echocardiography. Before the first RF application, ablation catheter was used to create a CARTO three-dimensional anatomical reconstruction of the LVOT (Figure 4).
 Based on the local electrocardiograms recorded from the tip of the ablation catheter, branching of the proximal part of the conduction system was registered to prevent its ablation. A series of 33 RF lesions (total time of RF application, 22.4 minutes; energy range, 35-40 W; temperature range, 35-40 °C; impedance, 95-128 Ohm) was delivered under the guidance of both echocardiography and CARTO mapping in the region of the septal bulge. An area of 4 cm2 was ablated. In addition, recording of the local electrograms was used to identify places with higher risk of atrioventricular conduction block during RF application. RF energy was reduced close to such places and atrioventricular conduction was closely monitored during RF application. In case of atrioventricular conduction prolongation, further application of RF energy was stopped at the particular spot with an immediate normalization of atrioventricular conduction.
Based on the local electrocardiograms recorded from the tip of the ablation catheter, branching of the proximal part of the conduction system was registered to prevent its ablation. A series of 33 RF lesions (total time of RF application, 22.4 minutes; energy range, 35-40 W; temperature range, 35-40 °C; impedance, 95-128 Ohm) was delivered under the guidance of both echocardiography and CARTO mapping in the region of the septal bulge. An area of 4 cm2 was ablated. In addition, recording of the local electrograms was used to identify places with higher risk of atrioventricular conduction block during RF application. RF energy was reduced close to such places and atrioventricular conduction was closely monitored during RF application. In case of atrioventricular conduction prolongation, further application of RF energy was stopped at the particular spot with an immediate normalization of atrioventricular conduction.
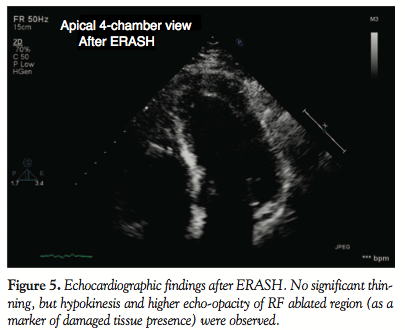
Damage of the tissue after RF ablation of septal hypertrophy was well visible on the echocardiography as a change in the tissue opacity (Figure 5). At the end of the procedure, there was no significant thinning, but hypokinesis was observed in the ablated region. Invasive measurement using the same tools and technique was then repeated at the end of the session. The peak left ventricular pressure of 203 mm Hg was not changed; however, the peak aortic pressure increased to 145 mm Hg. The procedure was stopped at this point, because further RF applications were no longer effective (there was no or minimal change of the amplitude of local electrograms at the site of ablation, indicating possible tissue edema that reduced efficacy of RF application). At the end of the procedure (total fluoroscopy time, 9.6 minutes; dose, 1.36 mGy/m2), there was neither widening of the QRS complex nor a change in the right bundle branch block morphology that was present since the ASA. No prolongation of atrioventricular conduction was observed either.
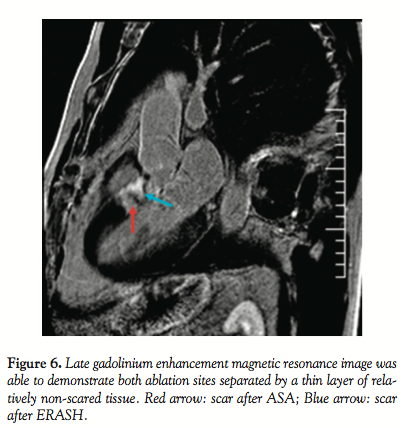 Follow-up. The patient felt well after ERASH. Continuous ECG monitoring (performed until discharge at day 8) did not reveal any atrioventricular conduction block or other arrhythmia. Maximum CK-MB mass was 1.1 µkat/L and maximum Troponin I was 3.3 µg/L (normal upper limit, 7.2 µkat/L and 0.03 µg/L, respectively). Seven days after the procedure, the ablated region exhibited similar changes of the opacity at echocardiography as at the end of the procedure, indicating damage at the ablated site (Figure 5). However SAM and LVOT gradient persisted, reaching about 50 mm Hg at rest and 100 mm Hg after nitrate provocation. The patient was therefore continued on beta-blockers. Magnetic resonance imaging (MRI) using gadolinium administration performed on day 8 after ERASH demonstrated late enhancement in two LVOT regions: the first one in the subaortic region corresponded with RF lesion sites, the second one (more midventricularly located) with scar after ASA (Figure 6). The patient was kept on his permanent medication after the procedure. At the 2-month follow-up exam, the patient reported improvement of symptoms. Dyspnea reduced to NYHA class 2 and angina CCS 1-2. Echocardiographically, the RF ablated region measured 14 mm; however, the persistent subaortic maximum was now akinetic, thus leading to a LVOT gradient reduction to 15 mm Hg. Gadolinium-contrast MRI showed findings similar to day 8 after ERASH.
Follow-up. The patient felt well after ERASH. Continuous ECG monitoring (performed until discharge at day 8) did not reveal any atrioventricular conduction block or other arrhythmia. Maximum CK-MB mass was 1.1 µkat/L and maximum Troponin I was 3.3 µg/L (normal upper limit, 7.2 µkat/L and 0.03 µg/L, respectively). Seven days after the procedure, the ablated region exhibited similar changes of the opacity at echocardiography as at the end of the procedure, indicating damage at the ablated site (Figure 5). However SAM and LVOT gradient persisted, reaching about 50 mm Hg at rest and 100 mm Hg after nitrate provocation. The patient was therefore continued on beta-blockers. Magnetic resonance imaging (MRI) using gadolinium administration performed on day 8 after ERASH demonstrated late enhancement in two LVOT regions: the first one in the subaortic region corresponded with RF lesion sites, the second one (more midventricularly located) with scar after ASA (Figure 6). The patient was kept on his permanent medication after the procedure. At the 2-month follow-up exam, the patient reported improvement of symptoms. Dyspnea reduced to NYHA class 2 and angina CCS 1-2. Echocardiographically, the RF ablated region measured 14 mm; however, the persistent subaortic maximum was now akinetic, thus leading to a LVOT gradient reduction to 15 mm Hg. Gadolinium-contrast MRI showed findings similar to day 8 after ERASH.
Discussion. Alcohol septal ablation, surgical myectomy, and dual-chamber pacing are the most discussed non-pharmacological options in the treatment of patients with symptomatic hypertrophic cardiomyopathy.1,3,9 The advantage of the first two methods is gradient decrease due to physical reduction of the septal thickness. In contrast, dual-chamber pacing reaches gradient reduction through pacing-induced asynchrony very likely, without true change of LVOT anatomy.9
ASA represents an established catheter-based approach causing LVOT gradient reduction through chemically-induced myocardial injury, leading to a change of LVOT morphology due to scarring.10 The success rate of ASA is high,11,12 and application of a very low amount of alcohol results in similar clinical and hemodynamic outcomes.13 Despite that, however, the two main limitations of ASA remain: dependence on the presence of suitable septal artery and risk of late-occurring complete atrioventricular block. RF ablation of hypertrophic septum might be a good therapeutic alternative that may overcome these issues: (1) steerable RF ablation catheter allows RF lesion application into selected region regardless of the septal vasculature; and (2) through recording of the local electrical activity from the catheter tip, it is possible to localize proximal branching of the conduction system and thus prevent RF-induced damage of these structures. In addition, late-occurring conduction blocks are not frequent after RF ablation of conventional arrhythmogenic substrates14 compared to ASA.15 Usage of additional tools like the electroanatomical mapping system CARTO and intracardiac echocardiography further helps to refine target site for RF delivery and to guide the ablation catheter into the target site.
As compared to ASA or surgical myectomy, it seems that RF septal ablation does not reduce LVOT gradient through significant thinning of the septum primarily, but rather through hypokinesis or akinesis of the ablated region. Despite this, akinesis of the ablated region led to a significant LVOT gradient over the long term, with concomitant improvement of symptoms in our patient.
The concept of ERASH was first reported by Lawrenz and Kuhn7 in 2004. Recently, these authors published results of their original series of 19 patients, in whom they performed ERASH using either the left-sided transaortic approach or the right-sided ablation of the interventricular septum.8 Regardless of the approach used, RF ablation led to a significant improvement of symptoms and exercise capacity due to LVOT gradient reduction that was primarily caused by the local hypokinesis rather than reduced thickness of the ablated region. To our knowledge, our study is the third published so far on this topic and its results correspond with the observations of these authors.7,8
Conclusion. RF ablation of septal hypertrophy is feasible and may be a promising method for gradient reduction in some patients with hypertrophic cardiomyopathy. It might be an option in patients with unsuccessful ASA who refuse surgical myectomy. However, the role of ERASH in the treatment of patients with obstructive hypertrophic cardiomyopathy needs to be established in larger prospective trials.
The main advantage of ERASH is its independence on septal vascularization, the possibility to deliver the lesion into a target region with a high accuracy, and reduction of the risk of conduction system damage (which is still a feared serious complication of both ASA and surgical myectomy)15 due to recording of the local electrical activity by the RF catheter at the intended target site. Usage of non-fluoroscopic electroanatomical mapping system and intracardiac echocardiography allows very precise localization of the ablation site.
References
- Gersh BJ, Maron BJ, Bonowe RO, et al. 2011 ACCF/AHA Guideline for the diagnosis and treatment of hypertrophic cardiomyopathy: a report of the American College of Cardiology Foundation/American Heart Association Task Force on Practice Guidelines. Circulation. 2011;124(24):e783-e831.
- Sigwart U. Non-surgical myocardial reduction for hypertrophic obstructive cardiomyopathy. Lancet. 1995;22(8969):211-214.
- Ommen SR, Maron BJ, Olivotto I, et al. Long-term effects of surgical septal myectomy on survival in patients with obstructive hypertrophic cardiomyopathy. J Am Coll Cardiol. 2005;46(3):470-476.
- Kuhn H, Lawrenz T, Lieder F, et al. Survival after transcoronary ablation of septal hypertrophy in hypertrophic obstructive cardiomyopathy (TASH): a 10 year experience. Clin Res Cardiol. 2008;97(4):234-243.
- Skrumeda LL, Mehra R. Comparison of standard and irrigated radiofrequency ablation in the canine ventricle. J Cardiovasc Electrophysiol. 1998;9(11):1196-1205.
- Delacretas E, William G, Stevenson WG, et al. Ablation of ventricular tachycardia with a saline-cooled radiofrequency catheter: anatomic and histologic characteristics of lesions in humans. J Cardiovasc Electrophysiol. 1998;10(6):860-865.
- Lawrenz T, Kuhn H. Endocardial radiofrequency ablation of septal hypertrophy. A new catheter-based modality of gradient reduction in hypertrophic obstructive cardiomyopathy. Z Kardiol. 2004;93(6):493-499.
- Lawrenz T, Borchert B, Leuner C, et al. Endocardial radiofrequency ablation for hypertrophic obstructive cardiomyopathy: acute results and 6 months follow-up in 19 patients. J Am Coll Cardiol. 2011;57(5):572-576.
- Fananapazir L, Epstein ND, Curiel RV, et al. Long-term results of dual-chamber (DDD) pacing in obstructive hypertrophic cardiomyopathy: evidence for progressive symptomatic and hemodynamic improvement and reduction of left ventricular hypertrophy. Circulation. 1994;90(6):2731-2742.
- van Dockum WG, Beek AM, ten Cate FJ, et al. Early onset and progression of left ventricular remodeling after alcohol septal ablation in hypertrophic obstructive cardiomyopathy. Circulation. 2005;111(19):2503-2508.
- Lakkis NM, Nagueh SF, Dunn JK, et al. Nonsurgical septal reduction therapy for hypertrophic obstructive cardiomyopathy: one-year follow-up. J Am Coll Cardiol. 2000;36(3):852-855.
- Veselka J, Duchonova R, Palenıckova J, et al. Impact of ethanol dosing on long-term outcome of alcohol septal ablation for obstructive hypertrophic cardiomyopathy: a single-center, prospective, and randomized study. Circ J. 2006;70(12):1550-1552.
- Veselka J, Zemanek D, Tomasov P, Duchonova R, Linhartova K. Alcohol septal ablation for obstructive hypertrophic cardiomyopathy: ultra-low dose of alcohol (1 ml) is still effective. Heart Vessels. 2009;24(1):27-31.
- Scheinman MM, Huang S. The 1998 NASPE prospective catheter ablation registry. Pacing Clin Electrophysiol. 2000;23(6):1020-1028.
- Nagueh SF, Groves BM, Schwarz L, et al. Alcohol septal ablation for the treatment of hypertrophic obstructive cardiomyopathy. A multicenter North American registry. J Am Coll Cardiol. 2011;58(22):2322-2328.
______________________________________
From the 1Clinic of Cardiology, 2nd Medical School of the Charles University and the University Hospital Motol, and 2Children's Heart Centre, University Hospital Motol, Prague, Czech Republic.
Disclosure: The authors have completed and returned the ICMJE Form for Disclosure of Potential Conflicts of Interest. The authors report no conflicts of interest regarding the content herein.
Funding: Supported by Ministry of Health, Czech Republic — conceptual development of research organization, University Hospital Motol, Prague, Czech Republic 00064203. Manuscript submitted November 21, 2012, final version accepted January 14, 2013.
Address for correspondence: Lucie Riedlbauchová, MD, PhD, Department of Cardiology, 2nd Medical School of the Charles University and University Hospital Motol, V Úvalu 84, 150 06 Prague 5, Czech Republic. Email: lucie.riedlbauchova@fnmotol.cz







