Patient Presentation
 A 55-year-old Caucasian male presented to the emergency department with a 2-day history of what looked like dried crusts of blood on his forearms. They were mildly painful and tender, but non-pruritic. His medical history was significant for atrial fibrillation, treated with sotalol and direct current cardioversion 2 weeks prior. At that time, enoxaparin was started to bridge anticoagulation to warfarin. Concurrent medications included aspirin.
A 55-year-old Caucasian male presented to the emergency department with a 2-day history of what looked like dried crusts of blood on his forearms. They were mildly painful and tender, but non-pruritic. His medical history was significant for atrial fibrillation, treated with sotalol and direct current cardioversion 2 weeks prior. At that time, enoxaparin was started to bridge anticoagulation to warfarin. Concurrent medications included aspirin.
Physical examination revealed scattered, discrete and coalescent, 3-mm to 5-mm, tense, superficial hemorrhagic vesicles on an erythematous base located on the bilateral forearms (see image above). Abdominal skin examination revealed large ecchymoses located at injection sites. Laboratory results showed normal platelets, hemoglobin and hematocrit values. The international normalized ratio and partial thromboplastin time were slightly increased (1.27 (normal 0.9 to 1.1 seconds) and 36.8 seconds (normal 23.0 to 34.0 seconds), respectively). Biopsy was obtained and evaluated for definitive diagnosis.
WHAT IS YOUR DIAGNOSIS?
DIAGNOSIS: HEPARIN-INDUCED HEMORRHAGIC BULLOUS DERMATOSIS
Enoxaparin is a low molecular weight heparin (LWMH) administered by injection for the purpose of anticoagulation. First recognized by Perrinaud and colleagues in 2006, heparin-induced hemorrhagic bullous dermatosis has been reported to result from treatment with LWMHs (enoxaparin, dalteparin and tinzaparin) and unfractionated heparin.1-5 No large studies of heparin-induced hemorrhagic bullous dermatosis have been performed to date and only a limited number of cases have been reported since 1998.
Clinical Presentation
Lesions present as hemorrhagic bullae appearing 5 to 21 days after initiation of heparin therapy on otherwise normal skin and areas of the body distant from the injection sites. Lesions may look similar to hemorrhagic crusts, but are found upon physical examination to be tender, tense hemorrhagic vesicles on an erythematous base. Lesions have mostly been observed on the upper and lower extremities and do not appear to involve the mucous membranes. Laboratory values have shown normal to slightly abnormal international normalized ratio and partial thromboplastin time, with platelets within normal limits. Severe coagulopathy, progression to skin necrosis and associated systemic symptoms have not been reported in published cases, though one patient subsequently died of a seemingly unrelated cerebral hemorrhage.2
Pathophysiology
The underlying pathophysiological mechanism of this condition has not yet been elucidated. Two groups have postulated that the reaction may not be due to heparin alone since reports of similar clinical presentation have been associated with other medications such as etanercept, furosemide, aminocaproic acid and phenylbutazone.2,5
Histopathology

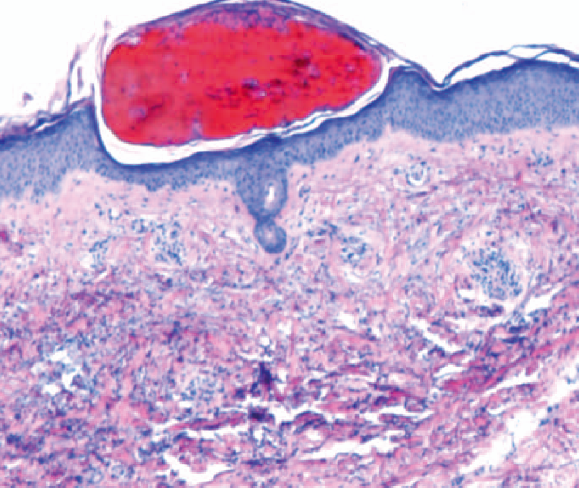
 Histologic examination of skin biopsies showed subcorneal and intracorneal hemorrhagic vesicles with minimal inflammation and no evidence of vasculitis (see Figures 2 and 3, left to right). This was consistent with the diagnosis of heparin-induced hemorrhagic bullous dermatosis. A few cases have reported inflammation and eosinophils within the dermis, which would suggest a hypersensitivity-type reaction, though that was not observed in this case.3,4
Histologic examination of skin biopsies showed subcorneal and intracorneal hemorrhagic vesicles with minimal inflammation and no evidence of vasculitis (see Figures 2 and 3, left to right). This was consistent with the diagnosis of heparin-induced hemorrhagic bullous dermatosis. A few cases have reported inflammation and eosinophils within the dermis, which would suggest a hypersensitivity-type reaction, though that was not observed in this case.3,4
Differential Diagnosis
Porphyria cutanea tarda skin findings include blisters, bullae, increased fragility, scarring and hyperpigmentation and hypopigmentation affecting sun-exposed areas. Bullae contain serosanguinous fluid positive for porphyrin.
Heparin-induced skin necrosis is rare and often associated with heparin-induced thrombocytopenia. Skin necrosis is seen on histology, platelet count is low and anti heparin-platelet factor 4 (HPF4) antibodies can be present.
Bullous pemphigoid rarely presents with hemorrhagic bullae. Sub-epidermal bullae with eosinophils are seen on biopsy, and direct immunofluorescence shows IgG and C3 at the dermal-epidermal junction along the roof of a bulla. Targeted antigens are BP230 and BP180.
Epidermolysis bullosa acquisita may present with hemorrhagic bullae and involve extremities but subepidermal bullae are again seen on histology. Direct immunofluorescence demonstrates IgG or C3 along the floor of a bulla.
Management
Most reports have noted that the hemorrhagic bullae resolve within 10 to 14 days of heparin discontinuation. One report observed that a patient had resolution within the same time period even with continued heparin treatment.2 The patient in our case was advised to continue enoxaparin therapy given the mild nature of the eruption but self-discontinued against medical advice. Reassessment at 1-week follow-up showed resolving lesions and no new lesions.
Conclusion
Heparin-induced hemorrhagic bullous dermatosis was first recognized in 2006 as an uncommon reaction to heparin or low molecular weight heparin treatment. Bullae appear 5 to 21 days after initiation of heparin therapy. Lesions arise on otherwise normal skin, distant from injection sites, and are most commonly located on the extremities. Severe coagulopathy, progression to skin necrosis and associated systemic symptoms have not been observed. Histological examination reveals collections of epidermal red blood cells without associated vasculitis or thrombosis. The mechanism of heparin-induced hemorrhagic bullous dermatosis is not yet understood. Progression to severe disease or heparin-induced skin necrosis does not appear to be associated. Resolution occurs after cessation of heparin therapy in most cases but has also been reported to resolve with continued heparin treatment. While larger studies are needed, limited reports suggest that heparin therapy may be continued in the appropriate clinical context.
Mr. Chang is from the Medical College of Wisconsin.
Dr. Gharia and Chiu are with the Department of Dermatology, Medical College of Wisconsin.
Disclosure: The authors have no conflicts of interest or financial disclosures to report.
Patient Presentation
 A 55-year-old Caucasian male presented to the emergency department with a 2-day history of what looked like dried crusts of blood on his forearms. They were mildly painful and tender, but non-pruritic. His medical history was significant for atrial fibrillation, treated with sotalol and direct current cardioversion 2 weeks prior. At that time, enoxaparin was started to bridge anticoagulation to warfarin. Concurrent medications included aspirin.
A 55-year-old Caucasian male presented to the emergency department with a 2-day history of what looked like dried crusts of blood on his forearms. They were mildly painful and tender, but non-pruritic. His medical history was significant for atrial fibrillation, treated with sotalol and direct current cardioversion 2 weeks prior. At that time, enoxaparin was started to bridge anticoagulation to warfarin. Concurrent medications included aspirin.
Physical examination revealed scattered, discrete and coalescent, 3-mm to 5-mm, tense, superficial hemorrhagic vesicles on an erythematous base located on the bilateral forearms (see image above). Abdominal skin examination revealed large ecchymoses located at injection sites. Laboratory results showed normal platelets, hemoglobin and hematocrit values. The international normalized ratio and partial thromboplastin time were slightly increased (1.27 (normal 0.9 to 1.1 seconds) and 36.8 seconds (normal 23.0 to 34.0 seconds), respectively). Biopsy was obtained and evaluated for definitive diagnosis.
WHAT IS YOUR DIAGNOSIS?
DIAGNOSIS: HEPARIN-INDUCED HEMORRHAGIC BULLOUS DERMATOSIS
Enoxaparin is a low molecular weight heparin (LWMH) administered by injection for the purpose of anticoagulation. First recognized by Perrinaud and colleagues in 2006, heparin-induced hemorrhagic bullous dermatosis has been reported to result from treatment with LWMHs (enoxaparin, dalteparin and tinzaparin) and unfractionated heparin.1-5 No large studies of heparin-induced hemorrhagic bullous dermatosis have been performed to date and only a limited number of cases have been reported since 1998.
Clinical Presentation
Lesions present as hemorrhagic bullae appearing 5 to 21 days after initiation of heparin therapy on otherwise normal skin and areas of the body distant from the injection sites. Lesions may look similar to hemorrhagic crusts, but are found upon physical examination to be tender, tense hemorrhagic vesicles on an erythematous base. Lesions have mostly been observed on the upper and lower extremities and do not appear to involve the mucous membranes. Laboratory values have shown normal to slightly abnormal international normalized ratio and partial thromboplastin time, with platelets within normal limits. Severe coagulopathy, progression to skin necrosis and associated systemic symptoms have not been reported in published cases, though one patient subsequently died of a seemingly unrelated cerebral hemorrhage.2
Pathophysiology
The underlying pathophysiological mechanism of this condition has not yet been elucidated. Two groups have postulated that the reaction may not be due to heparin alone since reports of similar clinical presentation have been associated with other medications such as etanercept, furosemide, aminocaproic acid and phenylbutazone.2,5
Histopathology

 Histologic examination of skin biopsies showed subcorneal and intracorneal hemorrhagic vesicles with minimal inflammation and no evidence of vasculitis (see Figures 2 and 3, left to right). This was consistent with the diagnosis of heparin-induced hemorrhagic bullous dermatosis. A few cases have reported inflammation and eosinophils within the dermis, which would suggest a hypersensitivity-type reaction, though that was not observed in this case.3,4
Histologic examination of skin biopsies showed subcorneal and intracorneal hemorrhagic vesicles with minimal inflammation and no evidence of vasculitis (see Figures 2 and 3, left to right). This was consistent with the diagnosis of heparin-induced hemorrhagic bullous dermatosis. A few cases have reported inflammation and eosinophils within the dermis, which would suggest a hypersensitivity-type reaction, though that was not observed in this case.3,4
Differential Diagnosis
Porphyria cutanea tarda skin findings include blisters, bullae, increased fragility, scarring and hyperpigmentation and hypopigmentation affecting sun-exposed areas. Bullae contain serosanguinous fluid positive for porphyrin.
Heparin-induced skin necrosis is rare and often associated with heparin-induced thrombocytopenia. Skin necrosis is seen on histology, platelet count is low and anti heparin-platelet factor 4 (HPF4) antibodies can be present.
Bullous pemphigoid rarely presents with hemorrhagic bullae. Sub-epidermal bullae with eosinophils are seen on biopsy, and direct immunofluorescence shows IgG and C3 at the dermal-epidermal junction along the roof of a bulla. Targeted antigens are BP230 and BP180.
Epidermolysis bullosa acquisita may present with hemorrhagic bullae and involve extremities but subepidermal bullae are again seen on histology. Direct immunofluorescence demonstrates IgG or C3 along the floor of a bulla.
Management
Most reports have noted that the hemorrhagic bullae resolve within 10 to 14 days of heparin discontinuation. One report observed that a patient had resolution within the same time period even with continued heparin treatment.2 The patient in our case was advised to continue enoxaparin therapy given the mild nature of the eruption but self-discontinued against medical advice. Reassessment at 1-week follow-up showed resolving lesions and no new lesions.
Conclusion
Heparin-induced hemorrhagic bullous dermatosis was first recognized in 2006 as an uncommon reaction to heparin or low molecular weight heparin treatment. Bullae appear 5 to 21 days after initiation of heparin therapy. Lesions arise on otherwise normal skin, distant from injection sites, and are most commonly located on the extremities. Severe coagulopathy, progression to skin necrosis and associated systemic symptoms have not been observed. Histological examination reveals collections of epidermal red blood cells without associated vasculitis or thrombosis. The mechanism of heparin-induced hemorrhagic bullous dermatosis is not yet understood. Progression to severe disease or heparin-induced skin necrosis does not appear to be associated. Resolution occurs after cessation of heparin therapy in most cases but has also been reported to resolve with continued heparin treatment. While larger studies are needed, limited reports suggest that heparin therapy may be continued in the appropriate clinical context.
Mr. Chang is from the Medical College of Wisconsin.
Dr. Gharia and Chiu are with the Department of Dermatology, Medical College of Wisconsin.
Disclosure: The authors have no conflicts of interest or financial disclosures to report.
Patient Presentation
A 55-year-old Caucasian male presented to the emergency department with a 2-day history of what looked like dried crusts of blood on his forearms. They were mildly painful and tender, but non-pruritic. His medical history was significant for atrial fibrillation, treated with sotalol and direct current cardioversion 2 weeks prior. At that time, enoxaparin was started to bridge anticoagulation to warfarin. Concurrent medications included aspirin.
Physical examination revealed scattered, discrete and coalescent, 3-mm to 5-mm, tense, superficial hemorrhagic vesicles on an erythematous base located on the bilateral forearms (see image above). Abdominal skin examination revealed large ecchymoses located at injection sites. Laboratory results showed normal platelets, hemoglobin and hematocrit values. The international normalized ratio and partial thromboplastin time were slightly increased (1.27 (normal 0.9 to 1.1 seconds) and 36.8 seconds (normal 23.0 to 34.0 seconds), respectively). Biopsy was obtained and evaluated for definitive diagnosis.
WHAT IS YOUR DIAGNOSIS?
DIAGNOSIS: HEPARIN-INDUCED HEMORRHAGIC BULLOUS DERMATOSIS
Enoxaparin is a low molecular weight heparin (LWMH) administered by injection for the purpose of anticoagulation. First recognized by Perrinaud and colleagues in 2006, heparin-induced hemorrhagic bullous dermatosis has been reported to result from treatment with LWMHs (enoxaparin, dalteparin and tinzaparin) and unfractionated heparin.1-5 No large studies of heparin-induced hemorrhagic bullous dermatosis have been performed to date and only a limited number of cases have been reported since 1998.
Clinical Presentation
Lesions present as hemorrhagic bullae appearing 5 to 21 days after initiation of heparin therapy on otherwise normal skin and areas of the body distant from the injection sites. Lesions may look similar to hemorrhagic crusts, but are found upon physical examination to be tender, tense hemorrhagic vesicles on an erythematous base. Lesions have mostly been observed on the upper and lower extremities and do not appear to involve the mucous membranes. Laboratory values have shown normal to slightly abnormal international normalized ratio and partial thromboplastin time, with platelets within normal limits. Severe coagulopathy, progression to skin necrosis and associated systemic symptoms have not been reported in published cases, though one patient subsequently died of a seemingly unrelated cerebral hemorrhage.2
Pathophysiology
The underlying pathophysiological mechanism of this condition has not yet been elucidated. Two groups have postulated that the reaction may not be due to heparin alone since reports of similar clinical presentation have been associated with other medications such as etanercept, furosemide, aminocaproic acid and phenylbutazone.2,5
Histopathology
Histologic examination of skin biopsies showed subcorneal and intracorneal hemorrhagic vesicles with minimal inflammation and no evidence of vasculitis (see Figures 2 and 3, left to right). This was consistent with the diagnosis of heparin-induced hemorrhagic bullous dermatosis. A few cases have reported inflammation and eosinophils within the dermis, which would suggest a hypersensitivity-type reaction, though that was not observed in this case.3,4
Differential Diagnosis
Porphyria cutanea tarda skin findings include blisters, bullae, increased fragility, scarring and hyperpigmentation and hypopigmentation affecting sun-exposed areas. Bullae contain serosanguinous fluid positive for porphyrin.
Heparin-induced skin necrosis is rare and often associated with heparin-induced thrombocytopenia. Skin necrosis is seen on histology, platelet count is low and anti heparin-platelet factor 4 (HPF4) antibodies can be present.
Bullous pemphigoid rarely presents with hemorrhagic bullae. Sub-epidermal bullae with eosinophils are seen on biopsy, and direct immunofluorescence shows IgG and C3 at the dermal-epidermal junction along the roof of a bulla. Targeted antigens are BP230 and BP180.
Epidermolysis bullosa acquisita may present with hemorrhagic bullae and involve extremities but subepidermal bullae are again seen on histology. Direct immunofluorescence demonstrates IgG or C3 along the floor of a bulla.
Management
Most reports have noted that the hemorrhagic bullae resolve within 10 to 14 days of heparin discontinuation. One report observed that a patient had resolution within the same time period even with continued heparin treatment.2 The patient in our case was advised to continue enoxaparin therapy given the mild nature of the eruption but self-discontinued against medical advice. Reassessment at 1-week follow-up showed resolving lesions and no new lesions.
Conclusion
Heparin-induced hemorrhagic bullous dermatosis was first recognized in 2006 as an uncommon reaction to heparin or low molecular weight heparin treatment. Bullae appear 5 to 21 days after initiation of heparin therapy. Lesions arise on otherwise normal skin, distant from injection sites, and are most commonly located on the extremities. Severe coagulopathy, progression to skin necrosis and associated systemic symptoms have not been observed. Histological examination reveals collections of epidermal red blood cells without associated vasculitis or thrombosis. The mechanism of heparin-induced hemorrhagic bullous dermatosis is not yet understood. Progression to severe disease or heparin-induced skin necrosis does not appear to be associated. Resolution occurs after cessation of heparin therapy in most cases but has also been reported to resolve with continued heparin treatment. While larger studies are needed, limited reports suggest that heparin therapy may be continued in the appropriate clinical context.
Mr. Chang is from the Medical College of Wisconsin.
Dr. Gharia and Chiu are with the Department of Dermatology, Medical College of Wisconsin.
Disclosure: The authors have no conflicts of interest or financial disclosures to report.





 Histologic examination of skin biopsies showed subcorneal and intracorneal hemorrhagic vesicles with minimal inflammation and no evidence of vasculitis (see Figures 2 and 3, left to right). This was consistent with the diagnosis of heparin-induced hemorrhagic bullous dermatosis. A few cases have reported inflammation and eosinophils within the dermis, which would suggest a hypersensitivity-type reaction, though that was not observed in this case.3,4
Histologic examination of skin biopsies showed subcorneal and intracorneal hemorrhagic vesicles with minimal inflammation and no evidence of vasculitis (see Figures 2 and 3, left to right). This was consistent with the diagnosis of heparin-induced hemorrhagic bullous dermatosis. A few cases have reported inflammation and eosinophils within the dermis, which would suggest a hypersensitivity-type reaction, though that was not observed in this case.3,4















