This column explores top relevant allergens, regional- and topic-based dermatitis presentations and clinical tips and pearls for diagnosis and treatment. The focus this month is sports gear-associated contact dermatitis.
Allergic Contact Dermatitis (ACD) is an important disease that notably affects 14.5 million Americans each year.1 The economic impact of this disease is high in terms of both patient morbidity and loss of income, school and work, not to mention significant expenditures for visits to health care providers and for therapy.1 Once patch testing is performed and a culprit has been identified, education becomes the critical intervention to ensure adherence to an avoidance regimen. With allergen avoidance, remission of the dermatitis ensues. If the patient is unable to comply with the avoidance regimen, they become susceptible to recurrent or sustained dermatitis or progression to a systematized presentation.2,3 In fact, education of the patient often begins before the diagnostic patch test is ever placed to ensure that the patient has an appropriate understanding of potential outcomes and his or her central role in both disease and treatment.
In the initial consultation, patients are often taught about the pathophysiology of ACD, ie, its delayed presentation and relationship with the immune system (sensitization to a chemical and then elicitation of a dermatitis with re-exposure). Moreover, it is explained that it can occur at any point in time, even to something that the patient has been using regularly for a short period of time or intermittently for years. In certain cases, the topics of the other key players, such as irritant contact dermatitis (ICD) and contact urticaria, may be explained, as history (not patch testing) can point to these as the correct diagnosis for the patient. It is important to note that ICD, the most prevalent form of contact dermatitis, can, at times, precede or be a concomitant diagnosis with ACD.4.5 Unlike ACD, ICD is not immune-mediated; it occurs secondary to contact with an irritating or abrasive substance. Contact urticaria (wheal and flare reaction), on the other hand, represents the least prevalent form of CD. It is important to note that it is an immune-mediated phenomenon whose hallmark is an IgE and mast cell-mediated, immediate-type hypersensitivity reaction. We acknowledge this form of hypersensitivity due to the severity of the potential deleterious, anaphylactic-type reactions and direct the reader to key sources.6,7,8
In this column, we highlight ACD and explore top relevant allergens, regional- and topic-based dermatitis presentations and clinical tips and pearls for diagnosis and treatment.
Sports Gear-Associated Contact Dermatitis
Athletes and other individuals who participate in sports activities — in a professional or amateur realm or for personal enjoyment — are at risk for developing contact dermatitis. The vast majority of athletes are amateurs who play sports for school or adult league teams. Athletes are exposed to various irritants and allergens during physical activity. The athlete may be more prone to developing contact dermatitis due to mechanical stress and increased sweating and temperature, which can induce small breaks, fissures, erosions and abrasions in the skin. The disruption of the normal epidermal barrier may increase the likelihood of developing a type IV hypersensitivity reaction. Athletes tend to have repetitive exposures to the same allergens during workouts, practice and training exercises. Continued exposures to allergens along with a break in the normal epidermal barrier may increase risk of contact allergy.
Most athletes will be exposed to a variety of allergens that are unique to their activity and equipment. This focus attempts to be as complete as possible in listing various sources of contact allergens in a tabular form for quick reference for providers and for patients.
Differential Diagnosis
 The differential diagnosis of contact dermatitis in the athlete can be broad and most commonly includes the conditions listed in Table 1 (left). Distinguishing between the two main types of contact dermatitis (allergic and irritant) in the athlete can be difficult, as the two often coexist. Determining a relevant allergen and appropriate avoidance will only help decrease the dermatitis; there will frequently be an associated irritant component that will need to be therapeutically addressed. ACD may be difficult to distinguish clinically from many other potential diagnoses; therefore, a thorough history is necessary.9 Other conditions, such as atopic, seborrheic and dyshidrotic dermatitis, should also be considered. Depending on the clinical presentation, bacterial, fungal or viral cultures can be performed. If ACD is still suspected, patch testing is the standard tool for diagnosis.4,10
The differential diagnosis of contact dermatitis in the athlete can be broad and most commonly includes the conditions listed in Table 1 (left). Distinguishing between the two main types of contact dermatitis (allergic and irritant) in the athlete can be difficult, as the two often coexist. Determining a relevant allergen and appropriate avoidance will only help decrease the dermatitis; there will frequently be an associated irritant component that will need to be therapeutically addressed. ACD may be difficult to distinguish clinically from many other potential diagnoses; therefore, a thorough history is necessary.9 Other conditions, such as atopic, seborrheic and dyshidrotic dermatitis, should also be considered. Depending on the clinical presentation, bacterial, fungal or viral cultures can be performed. If ACD is still suspected, patch testing is the standard tool for diagnosis.4,10
It is important to recognize that the differential diagnosis can vary depending on the site of involvement. For example, the differential diagnosis of ACD of the hands will include pompholyx, palmar plantar psoriasis, irritant contact dermatitis and non-specific or idiopathic dermatitis. The hands are particularly prone to developing contact dermatitis due to their constant use and exposure to various environmental allergens.
As another example, athletes who use mouth guards during contact sports may develop an allergic contact dermatitis (a cheilitis) to the mouthpiece. The differential diagnosis in these cases can be broad and include oral lichen planus, actinic cheilitis and perlèche. Perioral dermatitis may have features similar to allergic contact cheilitis, but there will often be a zone of normal skin immediately surrounding the vermilion border in contrast to allergic cheilitis, where the vermilion is often involved and effaced.9 Oral lichen planus (LP) or lichenoid oral lesions may be caused by contact allergy to dental materials, particularly ones containing metals such as mercury, gold, nickel and chromium.11-13 If LP lesions are in proximity to such materials, suspicion should be heightened.9 Moreover, perlèche-like symptoms may occur in previously sensitized individuals who contact nickel or rubber objects at the corners of the mouth, such as mouth guards in football and basketball players. Erosions resembling aphthous ulcers can result from oral contact with nickel objects14 and has been reported in patients with allergies to balsam of Peru.
Classifying the morphology and location of an individual’s allergic contact dermatitis to site-specific areas is a practical method for approaching the evaluation and treatment of the patient. Table 1 includes a differential diagnosis for sports gear-associated contact dermatitis.
Obtaining a Thorough Patient History
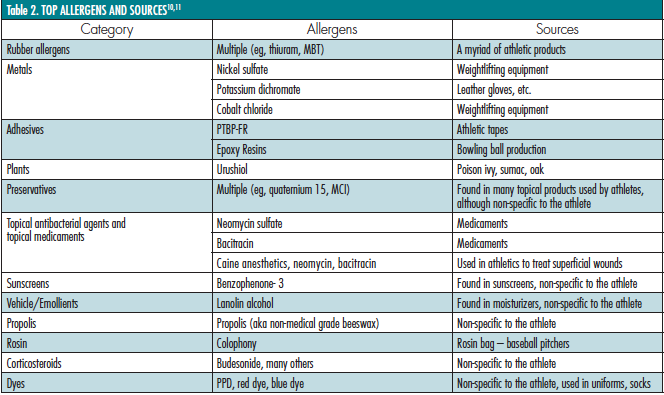
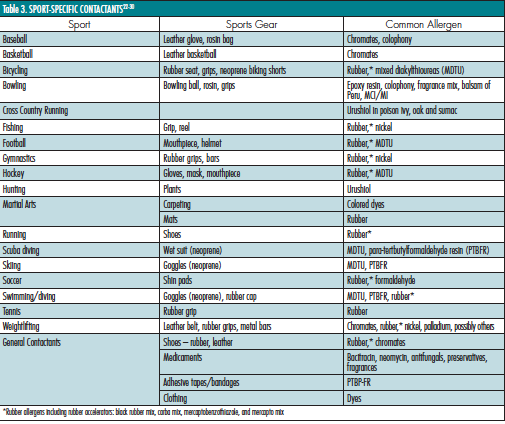
The importance of performing a thorough exposure history cannot be stressed enough. The clinician must assess the patient’s vocation and all activities in which the individual partakes. Pre-made questionnaires that the patient can fill out before or after an appointment can be invaluable in pinpointing causes of allergic and irritant contact dermatitis. In some cases, it is necessary to visit the activity site or workout place to view the athlete in his or her day-to-day routine to try to determine the causative allergen or irritant. Often, patients do not think of potential allergens that could be a problem and detection requires the experience of a physician (Table 2, bottom left). For example, a weight lifter will often overlook rubber or neoprene handles on weight equipment or the leather weight-lifting belt that he or she has used without difficulty for years. It is up to the physician to be as aware of the various sport-specific contactants that athletes may be exposed to (Table 3, bottom right).

 On a final clinical note, tinea pedis, tinea cruris and other forms of this dermatophyte infection will often be seen in athletes. An important diagnostic test in the evaluation of any scaling dermatoses is the potassium hydroxide (KOH) test. Scale is removed in a non-traumatic manner and dissolved in KOH. Under microscopy, fungal elements, if present, are indicative of a dermatophyte infection. Appropriate therapy with topical antifungal agents can be used. If the KOH is negative and the patient worsens when treated with topical corticosteroids, a repeat KOH examination should be performed to again evaluate for a dermatophyte. It is not uncommon to see a dermatophyte infection treated with a topical steroid become worse.
On a final clinical note, tinea pedis, tinea cruris and other forms of this dermatophyte infection will often be seen in athletes. An important diagnostic test in the evaluation of any scaling dermatoses is the potassium hydroxide (KOH) test. Scale is removed in a non-traumatic manner and dissolved in KOH. Under microscopy, fungal elements, if present, are indicative of a dermatophyte infection. Appropriate therapy with topical antifungal agents can be used. If the KOH is negative and the patient worsens when treated with topical corticosteroids, a repeat KOH examination should be performed to again evaluate for a dermatophyte. It is not uncommon to see a dermatophyte infection treated with a topical steroid become worse.
Top Allergens
Results from patch testing patients with sports gear-associated dermatitis have not been thoroughly published. Most information comes from case reports and case series. Some common allergens in these series have included rubber components, mixed dialklyl thiourea, rosin, formaldehyde, metals (especially nickel), benzocaine, epoxy resins and colophony (1-33). It is important to evaluate each individual with ACD thoroughly to properly determine the correct allergens. Table 2 lists common allergens and their sources.
Practicals of Patch Testing
As mentioned above, patch testing is often necessary to distinguish ACD from other causes of dermatitis and to identify the relevant allergen(s) responsible. Screening patch test trays are available, which isolate the most common chemicals and offer the provider clues for potential sources. The North American Standard Series, the North American Contact Dermatitis Group Tray and the Standardized Mayo Clinic Tray are three commonly employed screening trays and they include allergens from several different categories.17 Supplemental trays are also available, which assess for other allergens not included on the screening tray. Many supplemental trays can be used; the patch test history, knowledge of exposures and location of dermatitis should lead the clinician to the appropriate use of these supplemental trays. Supplemental trays should only be used when there is clinical data from the exposure history to justify their use. By including constituents and cross-reactors of the allergen in question, the chance of provoking relevant positive reactions is greater.18
Along these same lines, a topical medicament or moisturizer/cream product can be tested “as is;” however, many allergens may require preparation prior to testing.9 Collectively, these chemicals and products may overcome a threshold for reactivity. Fisher’s Contact Dermatitis9 is a great source to determine patch-testing concentrations to allergens not commonly used. It is contraindicated to patch test known irritants, such as strong acids, and unknown agents, which, on occasion, a patient will supply.
Pearls of Treatment: Every Dose Counts
As alluded to in the preface, one may be exposed to, and subsequently sensitized to, an allergen for days to years before actually developing an allergic contact dermatitis. Exposures can be additive, eventually causing one’s immune system to cross a metaphorical “threshold,” at which time a cutaneous response is elicited, such as in sports gear-associated contact dermatitis.19,22-30 Just as repeated contact over time led to this immune response, repeated avoidance of the majority of exposures over time will be required to induce remission. Irritants that induce ICD do not need this same immunological priming and can cause ICD from day 1.
Avoidance of specific allergens in personal care products in the workplace can prove to be a tedious task; however, there are programs available to aid in this endeavor. Both the Contact Allergen Management Program (CAMP), a service offered through the American Contact Dermatitis Society (ACDS),20 and the Contact Allergen Replacement Database (CARD), developed by the Mayo Clinic,21 allow a provider to enter a patient’s known contact allergens and produce a “shopping list” of products void of those particular chemicals. These programs also have the ability to exclude cross-reactors. They are extremely helpful for patients, most of whom are very grateful to have a list of safe products after leaving a visit.
While the goal of therapy is avoidance for both ACD and ICD, the patient must be treated until the dermatitis subsides. This is typically based on the severity and location of the reaction. For example, a mild case of ACD on the face from a mouth guard may be easily treated with topical hydrocortisone 2.5% cream, typically used in conjunction with an emollient cream. Once the patient has learned to avoid the allergen, use of the topical agents is discontinued. On the other end of the spectrum is the severe case of urushiol dermatitis in the cross-country runner who develops severe facial edema and eyelid swelling. In this scenario a tapering dose of oral corticosteroids may be the best therapeutic option. As in ACD, the best therapeutic approach to treating ICD is irritant avoidance and emollients.
Some sources, however, require avoidance creativity and finding alternatives, such as avoiding neoprene-based products for scuba divers allergic to mixed dialkyl thiourea or avoiding various rubber accelerators for athletes who have foot dermatitis to a component in their shoe. In such cases, custom-made diving suits and footwear can be obtained, respectively. Occasionally, avoidance is impossible and the athlete must either stop the activity or learn to minimize exposure while maintaining a treatment regimen. Topical corticosteroids, topical psoralen + ultraviolet A, and, in rare special cases, oral immunosuppressants may be required. Each patient needs to understand the importance of allergen avoidance and the risks and benefits of therapeutic options.
Dr. Anderson is an Associate Professor of Dermatology at Penn State University College of Medicine in State College, PA.
Dr. Jacob, the Section Editor of Allergen Focus, directs the contact dermatitis clinic at Rady Children’s Hospital – University of California in San Diego, CA. She is also Associate Clinical Professor of Pediatrics and Medicine (Dermatology) at the University of California, San Diego.
Disclosure: Dr. Jacob is the principal investigator for Smartchoice USA PREA-2 trial.
This column explores top relevant allergens, regional- and topic-based dermatitis presentations and clinical tips and pearls for diagnosis and treatment. The focus this month is sports gear-associated contact dermatitis.
Allergic Contact Dermatitis (ACD) is an important disease that notably affects 14.5 million Americans each year.1 The economic impact of this disease is high in terms of both patient morbidity and loss of income, school and work, not to mention significant expenditures for visits to health care providers and for therapy.1 Once patch testing is performed and a culprit has been identified, education becomes the critical intervention to ensure adherence to an avoidance regimen. With allergen avoidance, remission of the dermatitis ensues. If the patient is unable to comply with the avoidance regimen, they become susceptible to recurrent or sustained dermatitis or progression to a systematized presentation.2,3 In fact, education of the patient often begins before the diagnostic patch test is ever placed to ensure that the patient has an appropriate understanding of potential outcomes and his or her central role in both disease and treatment.
In the initial consultation, patients are often taught about the pathophysiology of ACD, ie, its delayed presentation and relationship with the immune system (sensitization to a chemical and then elicitation of a dermatitis with re-exposure). Moreover, it is explained that it can occur at any point in time, even to something that the patient has been using regularly for a short period of time or intermittently for years. In certain cases, the topics of the other key players, such as irritant contact dermatitis (ICD) and contact urticaria, may be explained, as history (not patch testing) can point to these as the correct diagnosis for the patient. It is important to note that ICD, the most prevalent form of contact dermatitis, can, at times, precede or be a concomitant diagnosis with ACD.4.5 Unlike ACD, ICD is not immune-mediated; it occurs secondary to contact with an irritating or abrasive substance. Contact urticaria (wheal and flare reaction), on the other hand, represents the least prevalent form of CD. It is important to note that it is an immune-mediated phenomenon whose hallmark is an IgE and mast cell-mediated, immediate-type hypersensitivity reaction. We acknowledge this form of hypersensitivity due to the severity of the potential deleterious, anaphylactic-type reactions and direct the reader to key sources.6,7,8
In this column, we highlight ACD and explore top relevant allergens, regional- and topic-based dermatitis presentations and clinical tips and pearls for diagnosis and treatment.
Sports Gear-Associated Contact Dermatitis
Athletes and other individuals who participate in sports activities — in a professional or amateur realm or for personal enjoyment — are at risk for developing contact dermatitis. The vast majority of athletes are amateurs who play sports for school or adult league teams. Athletes are exposed to various irritants and allergens during physical activity. The athlete may be more prone to developing contact dermatitis due to mechanical stress and increased sweating and temperature, which can induce small breaks, fissures, erosions and abrasions in the skin. The disruption of the normal epidermal barrier may increase the likelihood of developing a type IV hypersensitivity reaction. Athletes tend to have repetitive exposures to the same allergens during workouts, practice and training exercises. Continued exposures to allergens along with a break in the normal epidermal barrier may increase risk of contact allergy.
Most athletes will be exposed to a variety of allergens that are unique to their activity and equipment. This focus attempts to be as complete as possible in listing various sources of contact allergens in a tabular form for quick reference for providers and for patients.
Differential Diagnosis
 The differential diagnosis of contact dermatitis in the athlete can be broad and most commonly includes the conditions listed in Table 1 (left). Distinguishing between the two main types of contact dermatitis (allergic and irritant) in the athlete can be difficult, as the two often coexist. Determining a relevant allergen and appropriate avoidance will only help decrease the dermatitis; there will frequently be an associated irritant component that will need to be therapeutically addressed. ACD may be difficult to distinguish clinically from many other potential diagnoses; therefore, a thorough history is necessary.9 Other conditions, such as atopic, seborrheic and dyshidrotic dermatitis, should also be considered. Depending on the clinical presentation, bacterial, fungal or viral cultures can be performed. If ACD is still suspected, patch testing is the standard tool for diagnosis.4,10
The differential diagnosis of contact dermatitis in the athlete can be broad and most commonly includes the conditions listed in Table 1 (left). Distinguishing between the two main types of contact dermatitis (allergic and irritant) in the athlete can be difficult, as the two often coexist. Determining a relevant allergen and appropriate avoidance will only help decrease the dermatitis; there will frequently be an associated irritant component that will need to be therapeutically addressed. ACD may be difficult to distinguish clinically from many other potential diagnoses; therefore, a thorough history is necessary.9 Other conditions, such as atopic, seborrheic and dyshidrotic dermatitis, should also be considered. Depending on the clinical presentation, bacterial, fungal or viral cultures can be performed. If ACD is still suspected, patch testing is the standard tool for diagnosis.4,10
It is important to recognize that the differential diagnosis can vary depending on the site of involvement. For example, the differential diagnosis of ACD of the hands will include pompholyx, palmar plantar psoriasis, irritant contact dermatitis and non-specific or idiopathic dermatitis. The hands are particularly prone to developing contact dermatitis due to their constant use and exposure to various environmental allergens.
As another example, athletes who use mouth guards during contact sports may develop an allergic contact dermatitis (a cheilitis) to the mouthpiece. The differential diagnosis in these cases can be broad and include oral lichen planus, actinic cheilitis and perlèche. Perioral dermatitis may have features similar to allergic contact cheilitis, but there will often be a zone of normal skin immediately surrounding the vermilion border in contrast to allergic cheilitis, where the vermilion is often involved and effaced.9 Oral lichen planus (LP) or lichenoid oral lesions may be caused by contact allergy to dental materials, particularly ones containing metals such as mercury, gold, nickel and chromium.11-13 If LP lesions are in proximity to such materials, suspicion should be heightened.9 Moreover, perlèche-like symptoms may occur in previously sensitized individuals who contact nickel or rubber objects at the corners of the mouth, such as mouth guards in football and basketball players. Erosions resembling aphthous ulcers can result from oral contact with nickel objects14 and has been reported in patients with allergies to balsam of Peru.
Classifying the morphology and location of an individual’s allergic contact dermatitis to site-specific areas is a practical method for approaching the evaluation and treatment of the patient. Table 1 includes a differential diagnosis for sports gear-associated contact dermatitis.
Obtaining a Thorough Patient History
The importance of performing a thorough exposure history cannot be stressed enough. The clinician must assess the patient’s vocation and all activities in which the individual partakes. Pre-made questionnaires that the patient can fill out before or after an appointment can be invaluable in pinpointing causes of allergic and irritant contact dermatitis. In some cases, it is necessary to visit the activity site or workout place to view the athlete in his or her day-to-day routine to try to determine the causative allergen or irritant. Often, patients do not think of potential allergens that could be a problem and detection requires the experience of a physician (Table 2, bottom left). For example, a weight lifter will often overlook rubber or neoprene handles on weight equipment or the leather weight-lifting belt that he or she has used without difficulty for years. It is up to the physician to be as aware of the various sport-specific contactants that athletes may be exposed to (Table 3, bottom right).

 On a final clinical note, tinea pedis, tinea cruris and other forms of this dermatophyte infection will often be seen in athletes. An important diagnostic test in the evaluation of any scaling dermatoses is the potassium hydroxide (KOH) test. Scale is removed in a non-traumatic manner and dissolved in KOH. Under microscopy, fungal elements, if present, are indicative of a dermatophyte infection. Appropriate therapy with topical antifungal agents can be used. If the KOH is negative and the patient worsens when treated with topical corticosteroids, a repeat KOH examination should be performed to again evaluate for a dermatophyte. It is not uncommon to see a dermatophyte infection treated with a topical steroid become worse.
On a final clinical note, tinea pedis, tinea cruris and other forms of this dermatophyte infection will often be seen in athletes. An important diagnostic test in the evaluation of any scaling dermatoses is the potassium hydroxide (KOH) test. Scale is removed in a non-traumatic manner and dissolved in KOH. Under microscopy, fungal elements, if present, are indicative of a dermatophyte infection. Appropriate therapy with topical antifungal agents can be used. If the KOH is negative and the patient worsens when treated with topical corticosteroids, a repeat KOH examination should be performed to again evaluate for a dermatophyte. It is not uncommon to see a dermatophyte infection treated with a topical steroid become worse.
Top Allergens
Results from patch testing patients with sports gear-associated dermatitis have not been thoroughly published. Most information comes from case reports and case series. Some common allergens in these series have included rubber components, mixed dialklyl thiourea, rosin, formaldehyde, metals (especially nickel), benzocaine, epoxy resins and colophony (1-33). It is important to evaluate each individual with ACD thoroughly to properly determine the correct allergens. Table 2 lists common allergens and their sources.
Practicals of Patch Testing
As mentioned above, patch testing is often necessary to distinguish ACD from other causes of dermatitis and to identify the relevant allergen(s) responsible. Screening patch test trays are available, which isolate the most common chemicals and offer the provider clues for potential sources. The North American Standard Series, the North American Contact Dermatitis Group Tray and the Standardized Mayo Clinic Tray are three commonly employed screening trays and they include allergens from several different categories.17 Supplemental trays are also available, which assess for other allergens not included on the screening tray. Many supplemental trays can be used; the patch test history, knowledge of exposures and location of dermatitis should lead the clinician to the appropriate use of these supplemental trays. Supplemental trays should only be used when there is clinical data from the exposure history to justify their use. By including constituents and cross-reactors of the allergen in question, the chance of provoking relevant positive reactions is greater.18
Along these same lines, a topical medicament or moisturizer/cream product can be tested “as is;” however, many allergens may require preparation prior to testing.9 Collectively, these chemicals and products may overcome a threshold for reactivity. Fisher’s Contact Dermatitis9 is a great source to determine patch-testing concentrations to allergens not commonly used. It is contraindicated to patch test known irritants, such as strong acids, and unknown agents, which, on occasion, a patient will supply.
Pearls of Treatment: Every Dose Counts
As alluded to in the preface, one may be exposed to, and subsequently sensitized to, an allergen for days to years before actually developing an allergic contact dermatitis. Exposures can be additive, eventually causing one’s immune system to cross a metaphorical “threshold,” at which time a cutaneous response is elicited, such as in sports gear-associated contact dermatitis.19,22-30 Just as repeated contact over time led to this immune response, repeated avoidance of the majority of exposures over time will be required to induce remission. Irritants that induce ICD do not need this same immunological priming and can cause ICD from day 1.
Avoidance of specific allergens in personal care products in the workplace can prove to be a tedious task; however, there are programs available to aid in this endeavor. Both the Contact Allergen Management Program (CAMP), a service offered through the American Contact Dermatitis Society (ACDS),20 and the Contact Allergen Replacement Database (CARD), developed by the Mayo Clinic,21 allow a provider to enter a patient’s known contact allergens and produce a “shopping list” of products void of those particular chemicals. These programs also have the ability to exclude cross-reactors. They are extremely helpful for patients, most of whom are very grateful to have a list of safe products after leaving a visit.
While the goal of therapy is avoidance for both ACD and ICD, the patient must be treated until the dermatitis subsides. This is typically based on the severity and location of the reaction. For example, a mild case of ACD on the face from a mouth guard may be easily treated with topical hydrocortisone 2.5% cream, typically used in conjunction with an emollient cream. Once the patient has learned to avoid the allergen, use of the topical agents is discontinued. On the other end of the spectrum is the severe case of urushiol dermatitis in the cross-country runner who develops severe facial edema and eyelid swelling. In this scenario a tapering dose of oral corticosteroids may be the best therapeutic option. As in ACD, the best therapeutic approach to treating ICD is irritant avoidance and emollients.
Some sources, however, require avoidance creativity and finding alternatives, such as avoiding neoprene-based products for scuba divers allergic to mixed dialkyl thiourea or avoiding various rubber accelerators for athletes who have foot dermatitis to a component in their shoe. In such cases, custom-made diving suits and footwear can be obtained, respectively. Occasionally, avoidance is impossible and the athlete must either stop the activity or learn to minimize exposure while maintaining a treatment regimen. Topical corticosteroids, topical psoralen + ultraviolet A, and, in rare special cases, oral immunosuppressants may be required. Each patient needs to understand the importance of allergen avoidance and the risks and benefits of therapeutic options.
Dr. Anderson is an Associate Professor of Dermatology at Penn State University College of Medicine in State College, PA.
Dr. Jacob, the Section Editor of Allergen Focus, directs the contact dermatitis clinic at Rady Children’s Hospital – University of California in San Diego, CA. She is also Associate Clinical Professor of Pediatrics and Medicine (Dermatology) at the University of California, San Diego.
Disclosure: Dr. Jacob is the principal investigator for Smartchoice USA PREA-2 trial.
This column explores top relevant allergens, regional- and topic-based dermatitis presentations and clinical tips and pearls for diagnosis and treatment. The focus this month is sports gear-associated contact dermatitis.
Allergic Contact Dermatitis (ACD) is an important disease that notably affects 14.5 million Americans each year.1 The economic impact of this disease is high in terms of both patient morbidity and loss of income, school and work, not to mention significant expenditures for visits to health care providers and for therapy.1 Once patch testing is performed and a culprit has been identified, education becomes the critical intervention to ensure adherence to an avoidance regimen. With allergen avoidance, remission of the dermatitis ensues. If the patient is unable to comply with the avoidance regimen, they become susceptible to recurrent or sustained dermatitis or progression to a systematized presentation.2,3 In fact, education of the patient often begins before the diagnostic patch test is ever placed to ensure that the patient has an appropriate understanding of potential outcomes and his or her central role in both disease and treatment.
In the initial consultation, patients are often taught about the pathophysiology of ACD, ie, its delayed presentation and relationship with the immune system (sensitization to a chemical and then elicitation of a dermatitis with re-exposure). Moreover, it is explained that it can occur at any point in time, even to something that the patient has been using regularly for a short period of time or intermittently for years. In certain cases, the topics of the other key players, such as irritant contact dermatitis (ICD) and contact urticaria, may be explained, as history (not patch testing) can point to these as the correct diagnosis for the patient. It is important to note that ICD, the most prevalent form of contact dermatitis, can, at times, precede or be a concomitant diagnosis with ACD.4.5 Unlike ACD, ICD is not immune-mediated; it occurs secondary to contact with an irritating or abrasive substance. Contact urticaria (wheal and flare reaction), on the other hand, represents the least prevalent form of CD. It is important to note that it is an immune-mediated phenomenon whose hallmark is an IgE and mast cell-mediated, immediate-type hypersensitivity reaction. We acknowledge this form of hypersensitivity due to the severity of the potential deleterious, anaphylactic-type reactions and direct the reader to key sources.6,7,8
In this column, we highlight ACD and explore top relevant allergens, regional- and topic-based dermatitis presentations and clinical tips and pearls for diagnosis and treatment.
Sports Gear-Associated Contact Dermatitis
Athletes and other individuals who participate in sports activities — in a professional or amateur realm or for personal enjoyment — are at risk for developing contact dermatitis. The vast majority of athletes are amateurs who play sports for school or adult league teams. Athletes are exposed to various irritants and allergens during physical activity. The athlete may be more prone to developing contact dermatitis due to mechanical stress and increased sweating and temperature, which can induce small breaks, fissures, erosions and abrasions in the skin. The disruption of the normal epidermal barrier may increase the likelihood of developing a type IV hypersensitivity reaction. Athletes tend to have repetitive exposures to the same allergens during workouts, practice and training exercises. Continued exposures to allergens along with a break in the normal epidermal barrier may increase risk of contact allergy.
Most athletes will be exposed to a variety of allergens that are unique to their activity and equipment. This focus attempts to be as complete as possible in listing various sources of contact allergens in a tabular form for quick reference for providers and for patients.
Differential Diagnosis
The differential diagnosis of contact dermatitis in the athlete can be broad and most commonly includes the conditions listed in Table 1 (left). Distinguishing between the two main types of contact dermatitis (allergic and irritant) in the athlete can be difficult, as the two often coexist. Determining a relevant allergen and appropriate avoidance will only help decrease the dermatitis; there will frequently be an associated irritant component that will need to be therapeutically addressed. ACD may be difficult to distinguish clinically from many other potential diagnoses; therefore, a thorough history is necessary.9 Other conditions, such as atopic, seborrheic and dyshidrotic dermatitis, should also be considered. Depending on the clinical presentation, bacterial, fungal or viral cultures can be performed. If ACD is still suspected, patch testing is the standard tool for diagnosis.4,10
It is important to recognize that the differential diagnosis can vary depending on the site of involvement. For example, the differential diagnosis of ACD of the hands will include pompholyx, palmar plantar psoriasis, irritant contact dermatitis and non-specific or idiopathic dermatitis. The hands are particularly prone to developing contact dermatitis due to their constant use and exposure to various environmental allergens.
As another example, athletes who use mouth guards during contact sports may develop an allergic contact dermatitis (a cheilitis) to the mouthpiece. The differential diagnosis in these cases can be broad and include oral lichen planus, actinic cheilitis and perlèche. Perioral dermatitis may have features similar to allergic contact cheilitis, but there will often be a zone of normal skin immediately surrounding the vermilion border in contrast to allergic cheilitis, where the vermilion is often involved and effaced.9 Oral lichen planus (LP) or lichenoid oral lesions may be caused by contact allergy to dental materials, particularly ones containing metals such as mercury, gold, nickel and chromium.11-13 If LP lesions are in proximity to such materials, suspicion should be heightened.9 Moreover, perlèche-like symptoms may occur in previously sensitized individuals who contact nickel or rubber objects at the corners of the mouth, such as mouth guards in football and basketball players. Erosions resembling aphthous ulcers can result from oral contact with nickel objects14 and has been reported in patients with allergies to balsam of Peru.
Classifying the morphology and location of an individual’s allergic contact dermatitis to site-specific areas is a practical method for approaching the evaluation and treatment of the patient. Table 1 includes a differential diagnosis for sports gear-associated contact dermatitis.
Obtaining a Thorough Patient History
The importance of performing a thorough exposure history cannot be stressed enough. The clinician must assess the patient’s vocation and all activities in which the individual partakes. Pre-made questionnaires that the patient can fill out before or after an appointment can be invaluable in pinpointing causes of allergic and irritant contact dermatitis. In some cases, it is necessary to visit the activity site or workout place to view the athlete in his or her day-to-day routine to try to determine the causative allergen or irritant. Often, patients do not think of potential allergens that could be a problem and detection requires the experience of a physician (Table 2, bottom left). For example, a weight lifter will often overlook rubber or neoprene handles on weight equipment or the leather weight-lifting belt that he or she has used without difficulty for years. It is up to the physician to be as aware of the various sport-specific contactants that athletes may be exposed to (Table 3, bottom right).
On a final clinical note, tinea pedis, tinea cruris and other forms of this dermatophyte infection will often be seen in athletes. An important diagnostic test in the evaluation of any scaling dermatoses is the potassium hydroxide (KOH) test. Scale is removed in a non-traumatic manner and dissolved in KOH. Under microscopy, fungal elements, if present, are indicative of a dermatophyte infection. Appropriate therapy with topical antifungal agents can be used. If the KOH is negative and the patient worsens when treated with topical corticosteroids, a repeat KOH examination should be performed to again evaluate for a dermatophyte. It is not uncommon to see a dermatophyte infection treated with a topical steroid become worse.
Top Allergens
Results from patch testing patients with sports gear-associated dermatitis have not been thoroughly published. Most information comes from case reports and case series. Some common allergens in these series have included rubber components, mixed dialklyl thiourea, rosin, formaldehyde, metals (especially nickel), benzocaine, epoxy resins and colophony (1-33). It is important to evaluate each individual with ACD thoroughly to properly determine the correct allergens. Table 2 lists common allergens and their sources.
Practicals of Patch Testing
As mentioned above, patch testing is often necessary to distinguish ACD from other causes of dermatitis and to identify the relevant allergen(s) responsible. Screening patch test trays are available, which isolate the most common chemicals and offer the provider clues for potential sources. The North American Standard Series, the North American Contact Dermatitis Group Tray and the Standardized Mayo Clinic Tray are three commonly employed screening trays and they include allergens from several different categories.17 Supplemental trays are also available, which assess for other allergens not included on the screening tray. Many supplemental trays can be used; the patch test history, knowledge of exposures and location of dermatitis should lead the clinician to the appropriate use of these supplemental trays. Supplemental trays should only be used when there is clinical data from the exposure history to justify their use. By including constituents and cross-reactors of the allergen in question, the chance of provoking relevant positive reactions is greater.18
Along these same lines, a topical medicament or moisturizer/cream product can be tested “as is;” however, many allergens may require preparation prior to testing.9 Collectively, these chemicals and products may overcome a threshold for reactivity. Fisher’s Contact Dermatitis9 is a great source to determine patch-testing concentrations to allergens not commonly used. It is contraindicated to patch test known irritants, such as strong acids, and unknown agents, which, on occasion, a patient will supply.
Pearls of Treatment: Every Dose Counts
As alluded to in the preface, one may be exposed to, and subsequently sensitized to, an allergen for days to years before actually developing an allergic contact dermatitis. Exposures can be additive, eventually causing one’s immune system to cross a metaphorical “threshold,” at which time a cutaneous response is elicited, such as in sports gear-associated contact dermatitis.19,22-30 Just as repeated contact over time led to this immune response, repeated avoidance of the majority of exposures over time will be required to induce remission. Irritants that induce ICD do not need this same immunological priming and can cause ICD from day 1.
Avoidance of specific allergens in personal care products in the workplace can prove to be a tedious task; however, there are programs available to aid in this endeavor. Both the Contact Allergen Management Program (CAMP), a service offered through the American Contact Dermatitis Society (ACDS),20 and the Contact Allergen Replacement Database (CARD), developed by the Mayo Clinic,21 allow a provider to enter a patient’s known contact allergens and produce a “shopping list” of products void of those particular chemicals. These programs also have the ability to exclude cross-reactors. They are extremely helpful for patients, most of whom are very grateful to have a list of safe products after leaving a visit.
While the goal of therapy is avoidance for both ACD and ICD, the patient must be treated until the dermatitis subsides. This is typically based on the severity and location of the reaction. For example, a mild case of ACD on the face from a mouth guard may be easily treated with topical hydrocortisone 2.5% cream, typically used in conjunction with an emollient cream. Once the patient has learned to avoid the allergen, use of the topical agents is discontinued. On the other end of the spectrum is the severe case of urushiol dermatitis in the cross-country runner who develops severe facial edema and eyelid swelling. In this scenario a tapering dose of oral corticosteroids may be the best therapeutic option. As in ACD, the best therapeutic approach to treating ICD is irritant avoidance and emollients.
Some sources, however, require avoidance creativity and finding alternatives, such as avoiding neoprene-based products for scuba divers allergic to mixed dialkyl thiourea or avoiding various rubber accelerators for athletes who have foot dermatitis to a component in their shoe. In such cases, custom-made diving suits and footwear can be obtained, respectively. Occasionally, avoidance is impossible and the athlete must either stop the activity or learn to minimize exposure while maintaining a treatment regimen. Topical corticosteroids, topical psoralen + ultraviolet A, and, in rare special cases, oral immunosuppressants may be required. Each patient needs to understand the importance of allergen avoidance and the risks and benefits of therapeutic options.
Dr. Anderson is an Associate Professor of Dermatology at Penn State University College of Medicine in State College, PA.
Dr. Jacob, the Section Editor of Allergen Focus, directs the contact dermatitis clinic at Rady Children’s Hospital – University of California in San Diego, CA. She is also Associate Clinical Professor of Pediatrics and Medicine (Dermatology) at the University of California, San Diego.
Disclosure: Dr. Jacob is the principal investigator for Smartchoice USA PREA-2 trial.




 The differential diagnosis of contact dermatitis in the athlete can be broad and most commonly includes the conditions listed in Table 1 (left). Distinguishing between the two main types of contact dermatitis (allergic and irritant) in the athlete can be difficult, as the two often coexist. Determining a relevant allergen and appropriate avoidance will only help decrease the dermatitis; there will frequently be an associated irritant component that will need to be therapeutically addressed. ACD may be difficult to distinguish clinically from many other potential diagnoses; therefore, a thorough history is necessary.9 Other conditions, such as atopic, seborrheic and dyshidrotic dermatitis, should also be considered. Depending on the clinical presentation, bacterial, fungal or viral cultures can be performed. If ACD is still suspected, patch testing is the standard tool for diagnosis.4,10
The differential diagnosis of contact dermatitis in the athlete can be broad and most commonly includes the conditions listed in Table 1 (left). Distinguishing between the two main types of contact dermatitis (allergic and irritant) in the athlete can be difficult, as the two often coexist. Determining a relevant allergen and appropriate avoidance will only help decrease the dermatitis; there will frequently be an associated irritant component that will need to be therapeutically addressed. ACD may be difficult to distinguish clinically from many other potential diagnoses; therefore, a thorough history is necessary.9 Other conditions, such as atopic, seborrheic and dyshidrotic dermatitis, should also be considered. Depending on the clinical presentation, bacterial, fungal or viral cultures can be performed. If ACD is still suspected, patch testing is the standard tool for diagnosis.4,10
 On a final clinical note, tinea pedis, tinea cruris and other forms of this dermatophyte infection will often be seen in athletes. An important diagnostic test in the evaluation of any scaling dermatoses is the potassium hydroxide (KOH) test. Scale is removed in a non-traumatic manner and dissolved in KOH. Under microscopy, fungal elements, if present, are indicative of a dermatophyte infection. Appropriate therapy with topical antifungal agents can be used. If the KOH is negative and the patient worsens when treated with topical corticosteroids, a repeat KOH examination should be performed to again evaluate for a dermatophyte. It is not uncommon to see a dermatophyte infection treated with a topical steroid become worse.
On a final clinical note, tinea pedis, tinea cruris and other forms of this dermatophyte infection will often be seen in athletes. An important diagnostic test in the evaluation of any scaling dermatoses is the potassium hydroxide (KOH) test. Scale is removed in a non-traumatic manner and dissolved in KOH. Under microscopy, fungal elements, if present, are indicative of a dermatophyte infection. Appropriate therapy with topical antifungal agents can be used. If the KOH is negative and the patient worsens when treated with topical corticosteroids, a repeat KOH examination should be performed to again evaluate for a dermatophyte. It is not uncommon to see a dermatophyte infection treated with a topical steroid become worse.















