What Are These Hypopigmented Patches?
A 28-year-old woman presented for an initial evaluation of a “rash” on her neck of 1-year duration. She reported that these asymptomatic skin changes initially started as a few spots, and subsequently spread to a larger area. The patient also reported that these spots have “spread” to her shoulder, breasts, and abdomen. On physical examination, hypopigmented, atrophic macules coalescing into patches with the appearance of epidermal wrinkling were noted on the right lateral neck (Figure 1), right shoulder (Figure 2), and bilateral medial breasts. The patient had no family history of similar skin findings, denied trauma to the affected areas, and was otherwise healthy and taking no medications.

What is Your Diagnosis?
Answer on page 2
{{pagebreak}}
Diagnosis: Extragential Lichen Sclerosus et Atrophicus
Lichen sclerosus et atrophicus (LSA), originally described by Francois Henri Hallopeau in 1887, is a chronic inflammatory disease of unclear pathogenesis which affects both the epidermis and the dermis.1 The typical clinical presentation of LSA is in the anogenital area, occurring in at least 85% of cases.2 However, extragenital disease is not uncommon and can be found in as many as 15% to 20% of patients.3
Clinical Presentation
In both men and women, the clinical presentation of LSA is variable and may be insidious or aggressive. In women, it commonly affects the anogenital region. In men, however, involvement is limited to the glans and foreskin. Physical examination findings are classically described as “figure of eight” in female patients, indicating skin changes are seen around the vulva and anus in patches or plaques, with fragile, thinned, and atrophic skin. Similar lesions, grey-white in color, are seen on the glans or prepuce of men and can progress to involve the frenulum, leading to nonretractable foreskin and phimosis.4
Pruritus is the most common presenting symptom, with a tendency to be worse at night. In addition, patients report skin tenderness, burning, dysuria, dyspareunia, pain with defecation, and difficulty retracting the foreskin (in men). Patients with progressive disease often experience fissures, cracking, and abrasions, leading to scarring and a distortion of genital anatomy.5
Extragenital lesions are typically located on the inner thighs, submammary areas, neck, shoulders, and wrists (Figures 1 and 2). However, cases of infraorbital, eyelid, nail, and oral mucosal lesions have been reported.4,6 Morphologically, lesions are typically white opalescent atrophic papules that may coalesce into plaques and result in tissue-paper like skin. Described clinical variants include widespread guttate, zosteriform, and lichen planus-like lesions.1,7-9
Recently, with the advancement of noninvasive imaging modalities in dermatology, features of LSA on dermoscopy and confocal microscopy have been described. When biopsy is not possible or would rather be avoided (as in young children or in cosmetically sensitive areas), these modalities may be used to make the diagnosis of LSA. Dermoscopy demonstrates a well-demarcated, homogenous, whitish plaque with yellow circles akin to comedo-like openings. Furthermore, confocal microscopy reveals hyperkeratosis, atrophy of the epidermis, dark and round structures containing bright amorphous material, and coarse collagen in bundles.10
Epidemiology
Lichen sclerosus occurs in patients of all ages, with cases reported in patients as young as 6 months. There is a bimodal peak of incidence in prepubertal children and postmenopausal women, respectively, and in middle-aged men. LSA disproportionately affects women with the female to male ratio ranging from 10:1 to 5:1.11 Unfortunately, the exact prevalence of LSA is difficult to determine given that patients often present to different providers, including dermatologists, pediatricians, gynecologists, and urologists.12 The prevalence of LSA is estimated to range from 1 in 300 to 1 in 1000.4
Pathogenesis
Although the etiology of LSA is unknown, several mechanisms have been proposed to explain this disease, including autoimmune, genetic, infectious, and hormonal factors.11
Autoimmune and Genetic
A significant amount of autoimmune diseases are found in association with LSA; these being thyroid disease, pernicious anemia, diabetes mellitus, vitiligo, alopecia areata, and systemic lupus erythematosus.13 The frequency of these co-occurring has been described between 21% to 74% in women, however, only approximately 6% in men.12 Furthermore, circulating IgG autoantibodies that target extracellular matrix 1 protein can be found in 74% of women with genital LSA.14 Autoantibodies targeting BP180 and BP230, basement membrane zone proteins, have also been described in patients with vulvar LSA.15
In an observational study of 1052 female patients with vulvar LSA, 12% of patients had a positive family history. HLA-DQ7, HLA-DQ8, and DQ9 have been found to be most frequently associated with LSA.16,17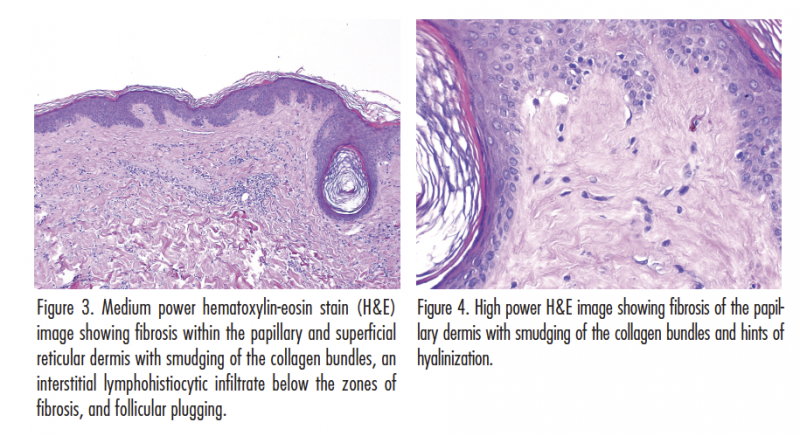
Infectious
Several infectious agents have been considered to have a role in the pathogenesis of LSA. Investigations into the role of Borrelia species have shown conflicting results; serology and polymerase chain reaction (PCR) testing have not been able to conclusively link Borrelia to LSA.18,19
Viral infections, such as Epstein-Barr virus (EBV) and human papilloma virus (HPV), have also been investigated. EBV DNA has been found in 26.5% of 34 patients with vulvar LSA on biopsy. However, further studies are necessary to confirm this association.20
The evidence for HPV infection has also been conflicting, with some reports showing high incidence of HPV PCR in LSA lesion and other showing no association.21,22
Hormonal
Given the high incidence of LSA in women with low estrogen states, such as prepubertal girls and postmenopausal women, hormonal factors have been considered to play a role in the development of LSA.13 Through investigation of punch biopsy specimens in patients with vulvar LSA, no evidence of altered hormone receptors were found in a study of 39 specimens.23 Conversely, in a study examining oral contraceptive use in patients with LSA, 100% were found to be on oral contraceptive pills compared with approximately 66% of controls.24
Article continues on page 3
{{pagebreak}}
Differential Diagnosis
Several diagnoses need to be considered in patients with a clinical presentation consistent with LSA. In women, the differential diagnosis of genital lesions includes lichen planus, vitiligo, lichen simplex chronicus, immunobullous diseases, and vulvar intraepithelial neoplasia. In men, erythroplasia of Queyrat, lichen planus, leukoplakia, and scleroderma must be considered.4,11 For extragenital lesions, morphea, atrophic lichen planus, and discoid lupus erythematosus may appear clinically similar.11 Interestingly, a case of interstitial mycoses fungoides masquerading as LSA, both clinically and histologically, was reported by Tekin and colleagues.25
Treatment
A systematic review and meta-analysis of randomized controlled trials on topical treatment for genital lichen sclerosus was performed to outline the most effective therapies. High-potency topical steroids (ie, clobetasol propionate, 0.05%) remain the most effective treatments available for patients when compared with placebo, without the risk of adverse effects. Pimecrolimus 1% cream has been shown to be effective for the improvement of symptoms, however, less so than clobetasol propionate, 0.05%. Topical testosterone, dihydrotestosterone, and progesterone have not shown to be effective.26
For extragenital disease, case reports confirm that topical clobetasol will improve blistering and hemorrhage, if present, but will have no effect on the atrophic plaque.27 Other treatments reported to have success in case reports and small trials include tacrolimus, calcipotriene, acitretin, carbon dioxide laser therapy, phototherapy, and pulse dye laser.27-30
Our Patient
The initial clinical presentation in our patient favored extragenital lichen sclerosus given the morphology of the lesions and their characteristic distribution. The patient did not have genital involvement. However, other diagnoses were considered and given that lichen sclerosus is a chronic disease, a skin biopsy was performed.
Histologic evaluation showed fibrosis within the papillary and superficial reticular dermis with smudging of the collagen bundles, an interstitial lymphohistiocytic infiltrate below the area of fibrosis, and follicular plugging (Figures 3 and 4). These findings were consistent with early extragenital lichen sclerosus. The patient was treated with high-potency topical steroids with significant improvement on follow-up.
Conclusion
Lichen sclerosus is a chronic, skin limited disease that can cause significant symptoms, disfigurement, and disability. Although etiology is still uncertain, autoimmune and genetic factors seem to play a significant role in the pathogenesis of this disease. While diagnosis is clinical with histologic confirmation, noninvasive imaging modalities such as dermoscopy and confocal microscopy may begin to play a significant role. High-potency topical corticosteroids and calcineurin inhibitors remain the mainstay of treatment for patients with this disease.
 Dr Fisher is a second-year dermatology resident in the department of dermatology at SUNY Downstate Medical Center in Brooklyn, NY.
Dr Fisher is a second-year dermatology resident in the department of dermatology at SUNY Downstate Medical Center in Brooklyn, NY.
Dr Khachemoune, the Section Editor of Derm DX, is with the department of dermatology at Veteran Affairs Medical Center, and the department of dermatology at the State University of New York Downstate, both in Brooklyn, NY.
Acknowledgment: We thank Dr Edward Heilman for reviewing the histopathology slides and description for this case.
Disclosure: The authors report no relevant financial relationships.
References
1. Ganesan L, Parmar H, Das JK, Gangopadhyay A. Extragenital lichen sclerosus et atrophicus. Indian J Dermatol. 2015;60(4):420.
2. Cooper S, Wojnarowska F. Anogenital (non-venereal) disease. In: Jorizzo J, Schaffer J Bolognia J, eds. Dermatology. 3rd ed. New York, NY: Elsevier; 2012:chap 73.
3. Yu L, Li Z, Feng S. Lichen sclerosus of face: a case report and review of literature. Indian J Dermatol. 2016;61(1):120.
4. Pugliese JM, Morey AF, Peterson AC. Lichen sclerosus: review of the literature and current recommendations for management. J Urol. 2007;178(6):2268-2276.
5. Val I, Almeida G. An overview of lichen sclerosus. Clin Obstet Gynecol. 2005;48(4):808-817.
6. Radke PM, Maltry AC, Mokhtarzadeh A, Harrison AR. A unique ocular presentation of extragenital lichen sclerosus [published online March 1, 2016]. Ophthal Plast Reconstr Surg. doi:10.1097/IOP.0000000000000662
7. Jayasekera PS, Parslew RA, McPartland J. An unusual pediatric presentation of guttate atrophic lesions on the trunk [published online March 5, 2016]. Int J Dermatol. doi:10.1111/ijd.13269
8. Vázquez MG, Navarra R, Martin-Urda MT, Abellaneda C, Quer A. Lichen sclerosus et atrophicus with cutaneous distribution simulating lichen planus. Case Rep Dermatol. 2010;2(1):55-59.
9. Chen JF, Chiang CP, Chen YF. Bilateral zosteriform extragenital lichen sclerosus et atrophicus: a new clinical presentation. J Dermatol. 2010;37(5):480-483.
10. Lacarrubba F, Pellacani G, Verzì AE, Pippione M, Micali G. Extragenital lichen sclerosus: clinical, dermoscopic, confocal microscopy and histologic correlations. J Am Acad Dermatol. 2015;72(1 suppl):S50-S52.
11. Yesudian PD, Sugunendran H, Bates CM, O’Mahony C. Lichen sclerosus. Int J STD AIDS. 2005;16(7):465-473.
12. Fistarol SK, Itin PH. Diagnosis and treatment of lichen sclerosus: an update. Am J Clin Dermatol. 2013;14(1):27-47.
13. Meyrick Thomas RH, Ridley CM, McGibbon DH, Black MM. Lichen sclerosus et atrophicus and autoimmunity—a study of 350 women. Br J Dermatol. 1988;118(1):41-46.
14. Oyama N, Chan I, Neill SM, et al. Autoantibodies to extracellular matrix protein 1 in lichen sclerosus. Lancet 2003;362(9378):118-123.
15. Howard A, Dean D, Cooper S, Kirtshig G, Wojnarowska F. Circulating basement membrane zone antibodies are found in lichen sclerosus of the vulva. Australas J Dermatol. 2004;45(1):12-15.
16. Sherman V, McPherson T, Baldo M, Salim A, Gao XH, Wojnarowska F. The high rate of familial lichen sclerosus suggests a genetic contribution: an observational cohort study. J Eur Acad Dermatol Venereol. 2010;24(9):1031-1034.
17. Marren P, Yell J, Chamock FM, Bunce M, Welsh K, Wojnarowska F. The association between lichen sclerosus and antigens of the HLA system. Br J Dermatol. 1995;132(2):197-203.
18. Edmonds E, Mavin S, Francis N, Ho-Yen D, Bunker C. Borrelia burgdorferi is not associated with genital lichen sclerosus in men. Br J Dermatol. 2009;160(2):459-460.
19. Weide B, Walz T, Garbe C. Is morphoea caused by Borrelia burgdorferi? A review. Br J Dermatol. 2000;142(4):636-44.
20. Aidé S, Lattario FR, Almeida G, do Val IC, da Costa Carvalho M. Epstein-Barr virus and human papillomavirus infection in vulvar lichen sclerosus. J Low Genit Tract Dis. 2010;14(4):319-322.
21. Drut RM, Gómez MA, Drut R, Lojo MM. Human papillomavirus is present in some cases of childhood penile lichen sclerosus: an in situ hybridization and SP-PCR study. Pediatr Dermatol. 1998;15(2):85-90.
22. Neill SM, Lessana-Leibowitch M, Pelisse M, Moyal-Barracco M. Lichen sclerosus, invasive squamous cell carcinoma, and human papillomavirus. Am J Obstet Gynecol. 1990;162(6):1633-1634.
23. Kohlberger PD, Joura EA, Bancher D, Gitsch G, Breitenecker G, Kieback DG. Evidence of androgen receptor expression in lichen sclerosus: an immunohistochemical study. J Soc Gynecol Investig. 1998;5(6):331-333.
24. Günthert AR, Faber M, Knappe G, Hellriegel S, Emons G. Early onset vulvar lichen sclerosus in premenopausal women and oral contraceptives. Eur J Obstet Gynecol Reprod Biol. 2008;137(1):56-60.
25. Tekin B, Kempf W, Seckin D, Ergun T, Yucelten D, Demirkessen C. Interstitial mycosis fungoides with lichen sclerosus-like clinical and histopathological features. Am J Dermatopathol. 2016;38(2):138-143.
26. Chi CC, Kirtschig G, Baldo M, Lewis F, Wang SH, Wojnarowska F. Systematic review and meta-analysis of randomized controlled trials on topical interventions for genital lichen sclerosus. J Am Acad Dermatol. 2012;67(2):305-312.
27. Shiver M, Papasakelariou C, Brown JA, Wirges M, Kincannon J. Extragenital bullous lichen sclerosus in a pediatric patient: a case report and literature review. Pediatr Dermatol. 2014;31(3):383-355.
28. Bergstrom KG, Mengden SJ, Kamino H, Ramsay D. Extragenital lichen sclerosus et atrophicus. Dermatol Online J. 2008;14(5):23.
29. Kim GW, Park HJ, Kim HS, et al. Topical tacrolimus ointment for the treatment of lichen sclerosus, comparing genital and extragenital involvement. J Dermatol. 2012;39(2):145-150.
30. Formiga Ade A, Torres Ide S, Rocha Bde O, et al. Disseminated extragenital lichen sclerosus et atrophicus treated with acitretin. Skinmed 2014;12(1):62-63.
What Are These Hypopigmented Patches?
A 28-year-old woman presented for an initial evaluation of a “rash” on her neck of 1-year duration. She reported that these asymptomatic skin changes initially started as a few spots, and subsequently spread to a larger area. The patient also reported that these spots have “spread” to her shoulder, breasts, and abdomen. On physical examination, hypopigmented, atrophic macules coalescing into patches with the appearance of epidermal wrinkling were noted on the right lateral neck (Figure 1), right shoulder (Figure 2), and bilateral medial breasts. The patient had no family history of similar skin findings, denied trauma to the affected areas, and was otherwise healthy and taking no medications.

What is Your Diagnosis?
Diagnosis: Extragential Lichen Sclerosus et Atrophicus
Lichen sclerosus et atrophicus (LSA), originally described by Francois Henri Hallopeau in 1887, is a chronic inflammatory disease of unclear pathogenesis which affects both the epidermis and the dermis.1 The typical clinical presentation of LSA is in the anogenital area, occurring in at least 85% of cases.2 However, extragenital disease is not uncommon and can be found in as many as 15% to 20% of patients.3
Clinical Presentation
In both men and women, the clinical presentation of LSA is variable and may be insidious or aggressive. In women, it commonly affects the anogenital region. In men, however, involvement is limited to the glans and foreskin. Physical examination findings are classically described as “figure of eight” in female patients, indicating skin changes are seen around the vulva and anus in patches or plaques, with fragile, thinned, and atrophic skin. Similar lesions, grey-white in color, are seen on the glans or prepuce of men and can progress to involve the frenulum, leading to nonretractable foreskin and phimosis.4
Pruritus is the most common presenting symptom, with a tendency to be worse at night. In addition, patients report skin tenderness, burning, dysuria, dyspareunia, pain with defecation, and difficulty retracting the foreskin (in men). Patients with progressive disease often experience fissures, cracking, and abrasions, leading to scarring and a distortion of genital anatomy.5
Extragenital lesions are typically located on the inner thighs, submammary areas, neck, shoulders, and wrists (Figures 1 and 2). However, cases of infraorbital, eyelid, nail, and oral mucosal lesions have been reported.4,6 Morphologically, lesions are typically white opalescent atrophic papules that may coalesce into plaques and result in tissue-paper like skin. Described clinical variants include widespread guttate, zosteriform, and lichen planus-like lesions.1,7-9
Recently, with the advancement of noninvasive imaging modalities in dermatology, features of LSA on dermoscopy and confocal microscopy have been described. When biopsy is not possible or would rather be avoided (as in young children or in cosmetically sensitive areas), these modalities may be used to make the diagnosis of LSA. Dermoscopy demonstrates a well-demarcated, homogenous, whitish plaque with yellow circles akin to comedo-like openings. Furthermore, confocal microscopy reveals hyperkeratosis, atrophy of the epidermis, dark and round structures containing bright amorphous material, and coarse collagen in bundles.10
Epidemiology
Lichen sclerosus occurs in patients of all ages, with cases reported in patients as young as 6 months. There is a bimodal peak of incidence in prepubertal children and postmenopausal women, respectively, and in middle-aged men. LSA disproportionately affects women with the female to male ratio ranging from 10:1 to 5:1.11 Unfortunately, the exact prevalence of LSA is difficult to determine given that patients often present to different providers, including dermatologists, pediatricians, gynecologists, and urologists.12 The prevalence of LSA is estimated to range from 1 in 300 to 1 in 1000.4
Pathogenesis
Although the etiology of LSA is unknown, several mechanisms have been proposed to explain this disease, including autoimmune, genetic, infectious, and hormonal factors.11
Autoimmune and Genetic
A significant amount of autoimmune diseases are found in association with LSA; these being thyroid disease, pernicious anemia, diabetes mellitus, vitiligo, alopecia areata, and systemic lupus erythematosus.13 The frequency of these co-occurring has been described between 21% to 74% in women, however, only approximately 6% in men.12 Furthermore, circulating IgG autoantibodies that target extracellular matrix 1 protein can be found in 74% of women with genital LSA.14 Autoantibodies targeting BP180 and BP230, basement membrane zone proteins, have also been described in patients with vulvar LSA.15
In an observational study of 1052 female patients with vulvar LSA, 12% of patients had a positive family history. HLA-DQ7, HLA-DQ8, and DQ9 have been found to be most frequently associated with LSA.16,17
Infectious
Several infectious agents have been considered to have a role in the pathogenesis of LSA. Investigations into the role of Borrelia species have shown conflicting results; serology and polymerase chain reaction (PCR) testing have not been able to conclusively link Borrelia to LSA.18,19
Viral infections, such as Epstein-Barr virus (EBV) and human papilloma virus (HPV), have also been investigated. EBV DNA has been found in 26.5% of 34 patients with vulvar LSA on biopsy. However, further studies are necessary to confirm this association.20
The evidence for HPV infection has also been conflicting, with some reports showing high incidence of HPV PCR in LSA lesion and other showing no association.21,22
Hormonal
Given the high incidence of LSA in women with low estrogen states, such as prepubertal girls and postmenopausal women, hormonal factors have been considered to play a role in the development of LSA.13 Through investigation of punch biopsy specimens in patients with vulvar LSA, no evidence of altered hormone receptors were found in a study of 39 specimens.23 Conversely, in a study examining oral contraceptive use in patients with LSA, 100% were found to be on oral contraceptive pills compared with approximately 66% of controls.24
Article continues on page 3
{{pagebreak}}
Differential Diagnosis
Several diagnoses need to be considered in patients with a clinical presentation consistent with LSA. In women, the differential diagnosis of genital lesions includes lichen planus, vitiligo, lichen simplex chronicus, immunobullous diseases, and vulvar intraepithelial neoplasia. In men, erythroplasia of Queyrat, lichen planus, leukoplakia, and scleroderma must be considered.4,11 For extragenital lesions, morphea, atrophic lichen planus, and discoid lupus erythematosus may appear clinically similar.11 Interestingly, a case of interstitial mycoses fungoides masquerading as LSA, both clinically and histologically, was reported by Tekin and colleagues.25
Treatment
A systematic review and meta-analysis of randomized controlled trials on topical treatment for genital lichen sclerosus was performed to outline the most effective therapies. High-potency topical steroids (ie, clobetasol propionate, 0.05%) remain the most effective treatments available for patients when compared with placebo, without the risk of adverse effects. Pimecrolimus 1% cream has been shown to be effective for the improvement of symptoms, however, less so than clobetasol propionate, 0.05%. Topical testosterone, dihydrotestosterone, and progesterone have not shown to be effective.26
For extragenital disease, case reports confirm that topical clobetasol will improve blistering and hemorrhage, if present, but will have no effect on the atrophic plaque.27 Other treatments reported to have success in case reports and small trials include tacrolimus, calcipotriene, acitretin, carbon dioxide laser therapy, phototherapy, and pulse dye laser.27-30
Our Patient
The initial clinical presentation in our patient favored extragenital lichen sclerosus given the morphology of the lesions and their characteristic distribution. The patient did not have genital involvement. However, other diagnoses were considered and given that lichen sclerosus is a chronic disease, a skin biopsy was performed.
Histologic evaluation showed fibrosis within the papillary and superficial reticular dermis with smudging of the collagen bundles, an interstitial lymphohistiocytic infiltrate below the area of fibrosis, and follicular plugging (Figures 3 and 4). These findings were consistent with early extragenital lichen sclerosus. The patient was treated with high-potency topical steroids with significant improvement on follow-up.
Conclusion
Lichen sclerosus is a chronic, skin limited disease that can cause significant symptoms, disfigurement, and disability. Although etiology is still uncertain, autoimmune and genetic factors seem to play a significant role in the pathogenesis of this disease. While diagnosis is clinical with histologic confirmation, noninvasive imaging modalities such as dermoscopy and confocal microscopy may begin to play a significant role. High-potency topical corticosteroids and calcineurin inhibitors remain the mainstay of treatment for patients with this disease.
 Dr Fisher is a second-year dermatology resident in the department of dermatology at SUNY Downstate Medical Center in Brooklyn, NY.
Dr Fisher is a second-year dermatology resident in the department of dermatology at SUNY Downstate Medical Center in Brooklyn, NY.
Dr Khachemoune, the Section Editor of Derm DX, is with the department of dermatology at Veteran Affairs Medical Center, and the department of dermatology at the State University of New York Downstate, both in Brooklyn, NY.
Acknowledgment: We thank Dr Edward Heilman for reviewing the histopathology slides and description for this case.
Disclosure: The authors report no relevant financial relationships.
References
1. Ganesan L, Parmar H, Das JK, Gangopadhyay A. Extragenital lichen sclerosus et atrophicus. Indian J Dermatol. 2015;60(4):420.
2. Cooper S, Wojnarowska F. Anogenital (non-venereal) disease. In: Jorizzo J, Schaffer J Bolognia J, eds. Dermatology. 3rd ed. New York, NY: Elsevier; 2012:chap 73.
3. Yu L, Li Z, Feng S. Lichen sclerosus of face: a case report and review of literature. Indian J Dermatol. 2016;61(1):120.
4. Pugliese JM, Morey AF, Peterson AC. Lichen sclerosus: review of the literature and current recommendations for management. J Urol. 2007;178(6):2268-2276.
5. Val I, Almeida G. An overview of lichen sclerosus. Clin Obstet Gynecol. 2005;48(4):808-817.
6. Radke PM, Maltry AC, Mokhtarzadeh A, Harrison AR. A unique ocular presentation of extragenital lichen sclerosus [published online March 1, 2016]. Ophthal Plast Reconstr Surg. doi:10.1097/IOP.0000000000000662
7. Jayasekera PS, Parslew RA, McPartland J. An unusual pediatric presentation of guttate atrophic lesions on the trunk [published online March 5, 2016]. Int J Dermatol. doi:10.1111/ijd.13269
8. Vázquez MG, Navarra R, Martin-Urda MT, Abellaneda C, Quer A. Lichen sclerosus et atrophicus with cutaneous distribution simulating lichen planus. Case Rep Dermatol. 2010;2(1):55-59.
9. Chen JF, Chiang CP, Chen YF. Bilateral zosteriform extragenital lichen sclerosus et atrophicus: a new clinical presentation. J Dermatol. 2010;37(5):480-483.
10. Lacarrubba F, Pellacani G, Verzì AE, Pippione M, Micali G. Extragenital lichen sclerosus: clinical, dermoscopic, confocal microscopy and histologic correlations. J Am Acad Dermatol. 2015;72(1 suppl):S50-S52.
11. Yesudian PD, Sugunendran H, Bates CM, O’Mahony C. Lichen sclerosus. Int J STD AIDS. 2005;16(7):465-473.
12. Fistarol SK, Itin PH. Diagnosis and treatment of lichen sclerosus: an update. Am J Clin Dermatol. 2013;14(1):27-47.
13. Meyrick Thomas RH, Ridley CM, McGibbon DH, Black MM. Lichen sclerosus et atrophicus and autoimmunity—a study of 350 women. Br J Dermatol. 1988;118(1):41-46.
14. Oyama N, Chan I, Neill SM, et al. Autoantibodies to extracellular matrix protein 1 in lichen sclerosus. Lancet 2003;362(9378):118-123.
15. Howard A, Dean D, Cooper S, Kirtshig G, Wojnarowska F. Circulating basement membrane zone antibodies are found in lichen sclerosus of the vulva. Australas J Dermatol. 2004;45(1):12-15.
16. Sherman V, McPherson T, Baldo M, Salim A, Gao XH, Wojnarowska F. The high rate of familial lichen sclerosus suggests a genetic contribution: an observational cohort study. J Eur Acad Dermatol Venereol. 2010;24(9):1031-1034.
17. Marren P, Yell J, Chamock FM, Bunce M, Welsh K, Wojnarowska F. The association between lichen sclerosus and antigens of the HLA system. Br J Dermatol. 1995;132(2):197-203.
18. Edmonds E, Mavin S, Francis N, Ho-Yen D, Bunker C. Borrelia burgdorferi is not associated with genital lichen sclerosus in men. Br J Dermatol. 2009;160(2):459-460.
19. Weide B, Walz T, Garbe C. Is morphoea caused by Borrelia burgdorferi? A review. Br J Dermatol. 2000;142(4):636-44.
20. Aidé S, Lattario FR, Almeida G, do Val IC, da Costa Carvalho M. Epstein-Barr virus and human papillomavirus infection in vulvar lichen sclerosus. J Low Genit Tract Dis. 2010;14(4):319-322.
21. Drut RM, Gómez MA, Drut R, Lojo MM. Human papillomavirus is present in some cases of childhood penile lichen sclerosus: an in situ hybridization and SP-PCR study. Pediatr Dermatol. 1998;15(2):85-90.
22. Neill SM, Lessana-Leibowitch M, Pelisse M, Moyal-Barracco M. Lichen sclerosus, invasive squamous cell carcinoma, and human papillomavirus. Am J Obstet Gynecol. 1990;162(6):1633-1634.
23. Kohlberger PD, Joura EA, Bancher D, Gitsch G, Breitenecker G, Kieback DG. Evidence of androgen receptor expression in lichen sclerosus: an immunohistochemical study. J Soc Gynecol Investig. 1998;5(6):331-333.
24. Günthert AR, Faber M, Knappe G, Hellriegel S, Emons G. Early onset vulvar lichen sclerosus in premenopausal women and oral contraceptives. Eur J Obstet Gynecol Reprod Biol. 2008;137(1):56-60.
25. Tekin B, Kempf W, Seckin D, Ergun T, Yucelten D, Demirkessen C. Interstitial mycosis fungoides with lichen sclerosus-like clinical and histopathological features. Am J Dermatopathol. 2016;38(2):138-143.
26. Chi CC, Kirtschig G, Baldo M, Lewis F, Wang SH, Wojnarowska F. Systematic review and meta-analysis of randomized controlled trials on topical interventions for genital lichen sclerosus. J Am Acad Dermatol. 2012;67(2):305-312.
27. Shiver M, Papasakelariou C, Brown JA, Wirges M, Kincannon J. Extragenital bullous lichen sclerosus in a pediatric patient: a case report and literature review. Pediatr Dermatol. 2014;31(3):383-355.
28. Bergstrom KG, Mengden SJ, Kamino H, Ramsay D. Extragenital lichen sclerosus et atrophicus. Dermatol Online J. 2008;14(5):23.
29. Kim GW, Park HJ, Kim HS, et al. Topical tacrolimus ointment for the treatment of lichen sclerosus, comparing genital and extragenital involvement. J Dermatol. 2012;39(2):145-150.
30. Formiga Ade A, Torres Ide S, Rocha Bde O, et al. Disseminated extragenital lichen sclerosus et atrophicus treated with acitretin. Skinmed 2014;12(1):62-63.
What Are These Hypopigmented Patches?
A 28-year-old woman presented for an initial evaluation of a “rash” on her neck of 1-year duration. She reported that these asymptomatic skin changes initially started as a few spots, and subsequently spread to a larger area. The patient also reported that these spots have “spread” to her shoulder, breasts, and abdomen. On physical examination, hypopigmented, atrophic macules coalescing into patches with the appearance of epidermal wrinkling were noted on the right lateral neck (Figure 1), right shoulder (Figure 2), and bilateral medial breasts. The patient had no family history of similar skin findings, denied trauma to the affected areas, and was otherwise healthy and taking no medications.
What is Your Diagnosis?
,
What Are These Hypopigmented Patches?
A 28-year-old woman presented for an initial evaluation of a “rash” on her neck of 1-year duration. She reported that these asymptomatic skin changes initially started as a few spots, and subsequently spread to a larger area. The patient also reported that these spots have “spread” to her shoulder, breasts, and abdomen. On physical examination, hypopigmented, atrophic macules coalescing into patches with the appearance of epidermal wrinkling were noted on the right lateral neck (Figure 1), right shoulder (Figure 2), and bilateral medial breasts. The patient had no family history of similar skin findings, denied trauma to the affected areas, and was otherwise healthy and taking no medications.
What is Your Diagnosis?
Answer on page 2
{{pagebreak}}
Diagnosis: Extragential Lichen Sclerosus et Atrophicus
Lichen sclerosus et atrophicus (LSA), originally described by Francois Henri Hallopeau in 1887, is a chronic inflammatory disease of unclear pathogenesis which affects both the epidermis and the dermis.1 The typical clinical presentation of LSA is in the anogenital area, occurring in at least 85% of cases.2 However, extragenital disease is not uncommon and can be found in as many as 15% to 20% of patients.3
Clinical Presentation
In both men and women, the clinical presentation of LSA is variable and may be insidious or aggressive. In women, it commonly affects the anogenital region. In men, however, involvement is limited to the glans and foreskin. Physical examination findings are classically described as “figure of eight” in female patients, indicating skin changes are seen around the vulva and anus in patches or plaques, with fragile, thinned, and atrophic skin. Similar lesions, grey-white in color, are seen on the glans or prepuce of men and can progress to involve the frenulum, leading to nonretractable foreskin and phimosis.4
Pruritus is the most common presenting symptom, with a tendency to be worse at night. In addition, patients report skin tenderness, burning, dysuria, dyspareunia, pain with defecation, and difficulty retracting the foreskin (in men). Patients with progressive disease often experience fissures, cracking, and abrasions, leading to scarring and a distortion of genital anatomy.5
Extragenital lesions are typically located on the inner thighs, submammary areas, neck, shoulders, and wrists (Figures 1 and 2). However, cases of infraorbital, eyelid, nail, and oral mucosal lesions have been reported.4,6 Morphologically, lesions are typically white opalescent atrophic papules that may coalesce into plaques and result in tissue-paper like skin. Described clinical variants include widespread guttate, zosteriform, and lichen planus-like lesions.1,7-9
Recently, with the advancement of noninvasive imaging modalities in dermatology, features of LSA on dermoscopy and confocal microscopy have been described. When biopsy is not possible or would rather be avoided (as in young children or in cosmetically sensitive areas), these modalities may be used to make the diagnosis of LSA. Dermoscopy demonstrates a well-demarcated, homogenous, whitish plaque with yellow circles akin to comedo-like openings. Furthermore, confocal microscopy reveals hyperkeratosis, atrophy of the epidermis, dark and round structures containing bright amorphous material, and coarse collagen in bundles.10
Epidemiology
Lichen sclerosus occurs in patients of all ages, with cases reported in patients as young as 6 months. There is a bimodal peak of incidence in prepubertal children and postmenopausal women, respectively, and in middle-aged men. LSA disproportionately affects women with the female to male ratio ranging from 10:1 to 5:1.11 Unfortunately, the exact prevalence of LSA is difficult to determine given that patients often present to different providers, including dermatologists, pediatricians, gynecologists, and urologists.12 The prevalence of LSA is estimated to range from 1 in 300 to 1 in 1000.4
Pathogenesis
Although the etiology of LSA is unknown, several mechanisms have been proposed to explain this disease, including autoimmune, genetic, infectious, and hormonal factors.11
Autoimmune and Genetic
A significant amount of autoimmune diseases are found in association with LSA; these being thyroid disease, pernicious anemia, diabetes mellitus, vitiligo, alopecia areata, and systemic lupus erythematosus.13 The frequency of these co-occurring has been described between 21% to 74% in women, however, only approximately 6% in men.12 Furthermore, circulating IgG autoantibodies that target extracellular matrix 1 protein can be found in 74% of women with genital LSA.14 Autoantibodies targeting BP180 and BP230, basement membrane zone proteins, have also been described in patients with vulvar LSA.15
In an observational study of 1052 female patients with vulvar LSA, 12% of patients had a positive family history. HLA-DQ7, HLA-DQ8, and DQ9 have been found to be most frequently associated with LSA.16,17
Infectious
Several infectious agents have been considered to have a role in the pathogenesis of LSA. Investigations into the role of Borrelia species have shown conflicting results; serology and polymerase chain reaction (PCR) testing have not been able to conclusively link Borrelia to LSA.18,19
Viral infections, such as Epstein-Barr virus (EBV) and human papilloma virus (HPV), have also been investigated. EBV DNA has been found in 26.5% of 34 patients with vulvar LSA on biopsy. However, further studies are necessary to confirm this association.20
The evidence for HPV infection has also been conflicting, with some reports showing high incidence of HPV PCR in LSA lesion and other showing no association.21,22
Hormonal
Given the high incidence of LSA in women with low estrogen states, such as prepubertal girls and postmenopausal women, hormonal factors have been considered to play a role in the development of LSA.13 Through investigation of punch biopsy specimens in patients with vulvar LSA, no evidence of altered hormone receptors were found in a study of 39 specimens.23 Conversely, in a study examining oral contraceptive use in patients with LSA, 100% were found to be on oral contraceptive pills compared with approximately 66% of controls.24
Article continues on page 3
{{pagebreak}}
Differential Diagnosis
Several diagnoses need to be considered in patients with a clinical presentation consistent with LSA. In women, the differential diagnosis of genital lesions includes lichen planus, vitiligo, lichen simplex chronicus, immunobullous diseases, and vulvar intraepithelial neoplasia. In men, erythroplasia of Queyrat, lichen planus, leukoplakia, and scleroderma must be considered.4,11 For extragenital lesions, morphea, atrophic lichen planus, and discoid lupus erythematosus may appear clinically similar.11 Interestingly, a case of interstitial mycoses fungoides masquerading as LSA, both clinically and histologically, was reported by Tekin and colleagues.25
Treatment
A systematic review and meta-analysis of randomized controlled trials on topical treatment for genital lichen sclerosus was performed to outline the most effective therapies. High-potency topical steroids (ie, clobetasol propionate, 0.05%) remain the most effective treatments available for patients when compared with placebo, without the risk of adverse effects. Pimecrolimus 1% cream has been shown to be effective for the improvement of symptoms, however, less so than clobetasol propionate, 0.05%. Topical testosterone, dihydrotestosterone, and progesterone have not shown to be effective.26
For extragenital disease, case reports confirm that topical clobetasol will improve blistering and hemorrhage, if present, but will have no effect on the atrophic plaque.27 Other treatments reported to have success in case reports and small trials include tacrolimus, calcipotriene, acitretin, carbon dioxide laser therapy, phototherapy, and pulse dye laser.27-30
Our Patient
The initial clinical presentation in our patient favored extragenital lichen sclerosus given the morphology of the lesions and their characteristic distribution. The patient did not have genital involvement. However, other diagnoses were considered and given that lichen sclerosus is a chronic disease, a skin biopsy was performed.
Histologic evaluation showed fibrosis within the papillary and superficial reticular dermis with smudging of the collagen bundles, an interstitial lymphohistiocytic infiltrate below the area of fibrosis, and follicular plugging (Figures 3 and 4). These findings were consistent with early extragenital lichen sclerosus. The patient was treated with high-potency topical steroids with significant improvement on follow-up.
Conclusion
Lichen sclerosus is a chronic, skin limited disease that can cause significant symptoms, disfigurement, and disability. Although etiology is still uncertain, autoimmune and genetic factors seem to play a significant role in the pathogenesis of this disease. While diagnosis is clinical with histologic confirmation, noninvasive imaging modalities such as dermoscopy and confocal microscopy may begin to play a significant role. High-potency topical corticosteroids and calcineurin inhibitors remain the mainstay of treatment for patients with this disease.
Dr Fisher is a second-year dermatology resident in the department of dermatology at SUNY Downstate Medical Center in Brooklyn, NY.
Dr Khachemoune, the Section Editor of Derm DX, is with the department of dermatology at Veteran Affairs Medical Center, and the department of dermatology at the State University of New York Downstate, both in Brooklyn, NY.
Acknowledgment: We thank Dr Edward Heilman for reviewing the histopathology slides and description for this case.
Disclosure: The authors report no relevant financial relationships.
References
1. Ganesan L, Parmar H, Das JK, Gangopadhyay A. Extragenital lichen sclerosus et atrophicus. Indian J Dermatol. 2015;60(4):420.
2. Cooper S, Wojnarowska F. Anogenital (non-venereal) disease. In: Jorizzo J, Schaffer J Bolognia J, eds. Dermatology. 3rd ed. New York, NY: Elsevier; 2012:chap 73.
3. Yu L, Li Z, Feng S. Lichen sclerosus of face: a case report and review of literature. Indian J Dermatol. 2016;61(1):120.
4. Pugliese JM, Morey AF, Peterson AC. Lichen sclerosus: review of the literature and current recommendations for management. J Urol. 2007;178(6):2268-2276.
5. Val I, Almeida G. An overview of lichen sclerosus. Clin Obstet Gynecol. 2005;48(4):808-817.
6. Radke PM, Maltry AC, Mokhtarzadeh A, Harrison AR. A unique ocular presentation of extragenital lichen sclerosus [published online March 1, 2016]. Ophthal Plast Reconstr Surg. doi:10.1097/IOP.0000000000000662
7. Jayasekera PS, Parslew RA, McPartland J. An unusual pediatric presentation of guttate atrophic lesions on the trunk [published online March 5, 2016]. Int J Dermatol. doi:10.1111/ijd.13269
8. Vázquez MG, Navarra R, Martin-Urda MT, Abellaneda C, Quer A. Lichen sclerosus et atrophicus with cutaneous distribution simulating lichen planus. Case Rep Dermatol. 2010;2(1):55-59.
9. Chen JF, Chiang CP, Chen YF. Bilateral zosteriform extragenital lichen sclerosus et atrophicus: a new clinical presentation. J Dermatol. 2010;37(5):480-483.
10. Lacarrubba F, Pellacani G, Verzì AE, Pippione M, Micali G. Extragenital lichen sclerosus: clinical, dermoscopic, confocal microscopy and histologic correlations. J Am Acad Dermatol. 2015;72(1 suppl):S50-S52.
11. Yesudian PD, Sugunendran H, Bates CM, O’Mahony C. Lichen sclerosus. Int J STD AIDS. 2005;16(7):465-473.
12. Fistarol SK, Itin PH. Diagnosis and treatment of lichen sclerosus: an update. Am J Clin Dermatol. 2013;14(1):27-47.
13. Meyrick Thomas RH, Ridley CM, McGibbon DH, Black MM. Lichen sclerosus et atrophicus and autoimmunity—a study of 350 women. Br J Dermatol. 1988;118(1):41-46.
14. Oyama N, Chan I, Neill SM, et al. Autoantibodies to extracellular matrix protein 1 in lichen sclerosus. Lancet 2003;362(9378):118-123.
15. Howard A, Dean D, Cooper S, Kirtshig G, Wojnarowska F. Circulating basement membrane zone antibodies are found in lichen sclerosus of the vulva. Australas J Dermatol. 2004;45(1):12-15.
16. Sherman V, McPherson T, Baldo M, Salim A, Gao XH, Wojnarowska F. The high rate of familial lichen sclerosus suggests a genetic contribution: an observational cohort study. J Eur Acad Dermatol Venereol. 2010;24(9):1031-1034.
17. Marren P, Yell J, Chamock FM, Bunce M, Welsh K, Wojnarowska F. The association between lichen sclerosus and antigens of the HLA system. Br J Dermatol. 1995;132(2):197-203.
18. Edmonds E, Mavin S, Francis N, Ho-Yen D, Bunker C. Borrelia burgdorferi is not associated with genital lichen sclerosus in men. Br J Dermatol. 2009;160(2):459-460.
19. Weide B, Walz T, Garbe C. Is morphoea caused by Borrelia burgdorferi? A review. Br J Dermatol. 2000;142(4):636-44.
20. Aidé S, Lattario FR, Almeida G, do Val IC, da Costa Carvalho M. Epstein-Barr virus and human papillomavirus infection in vulvar lichen sclerosus. J Low Genit Tract Dis. 2010;14(4):319-322.
21. Drut RM, Gómez MA, Drut R, Lojo MM. Human papillomavirus is present in some cases of childhood penile lichen sclerosus: an in situ hybridization and SP-PCR study. Pediatr Dermatol. 1998;15(2):85-90.
22. Neill SM, Lessana-Leibowitch M, Pelisse M, Moyal-Barracco M. Lichen sclerosus, invasive squamous cell carcinoma, and human papillomavirus. Am J Obstet Gynecol. 1990;162(6):1633-1634.
23. Kohlberger PD, Joura EA, Bancher D, Gitsch G, Breitenecker G, Kieback DG. Evidence of androgen receptor expression in lichen sclerosus: an immunohistochemical study. J Soc Gynecol Investig. 1998;5(6):331-333.
24. Günthert AR, Faber M, Knappe G, Hellriegel S, Emons G. Early onset vulvar lichen sclerosus in premenopausal women and oral contraceptives. Eur J Obstet Gynecol Reprod Biol. 2008;137(1):56-60.
25. Tekin B, Kempf W, Seckin D, Ergun T, Yucelten D, Demirkessen C. Interstitial mycosis fungoides with lichen sclerosus-like clinical and histopathological features. Am J Dermatopathol. 2016;38(2):138-143.
26. Chi CC, Kirtschig G, Baldo M, Lewis F, Wang SH, Wojnarowska F. Systematic review and meta-analysis of randomized controlled trials on topical interventions for genital lichen sclerosus. J Am Acad Dermatol. 2012;67(2):305-312.
27. Shiver M, Papasakelariou C, Brown JA, Wirges M, Kincannon J. Extragenital bullous lichen sclerosus in a pediatric patient: a case report and literature review. Pediatr Dermatol. 2014;31(3):383-355.
28. Bergstrom KG, Mengden SJ, Kamino H, Ramsay D. Extragenital lichen sclerosus et atrophicus. Dermatol Online J. 2008;14(5):23.
29. Kim GW, Park HJ, Kim HS, et al. Topical tacrolimus ointment for the treatment of lichen sclerosus, comparing genital and extragenital involvement. J Dermatol. 2012;39(2):145-150.
30. Formiga Ade A, Torres Ide S, Rocha Bde O, et al. Disseminated extragenital lichen sclerosus et atrophicus treated with acitretin. Skinmed 2014;12(1):62-63.
What Are These Hypopigmented Patches?
A 28-year-old woman presented for an initial evaluation of a “rash” on her neck of 1-year duration. She reported that these asymptomatic skin changes initially started as a few spots, and subsequently spread to a larger area. The patient also reported that these spots have “spread” to her shoulder, breasts, and abdomen. On physical examination, hypopigmented, atrophic macules coalescing into patches with the appearance of epidermal wrinkling were noted on the right lateral neck (Figure 1), right shoulder (Figure 2), and bilateral medial breasts. The patient had no family history of similar skin findings, denied trauma to the affected areas, and was otherwise healthy and taking no medications.
What is Your Diagnosis?
Diagnosis: Extragential Lichen Sclerosus et Atrophicus
Lichen sclerosus et atrophicus (LSA), originally described by Francois Henri Hallopeau in 1887, is a chronic inflammatory disease of unclear pathogenesis which affects both the epidermis and the dermis.1 The typical clinical presentation of LSA is in the anogenital area, occurring in at least 85% of cases.2 However, extragenital disease is not uncommon and can be found in as many as 15% to 20% of patients.3
Clinical Presentation
In both men and women, the clinical presentation of LSA is variable and may be insidious or aggressive. In women, it commonly affects the anogenital region. In men, however, involvement is limited to the glans and foreskin. Physical examination findings are classically described as “figure of eight” in female patients, indicating skin changes are seen around the vulva and anus in patches or plaques, with fragile, thinned, and atrophic skin. Similar lesions, grey-white in color, are seen on the glans or prepuce of men and can progress to involve the frenulum, leading to nonretractable foreskin and phimosis.4
Pruritus is the most common presenting symptom, with a tendency to be worse at night. In addition, patients report skin tenderness, burning, dysuria, dyspareunia, pain with defecation, and difficulty retracting the foreskin (in men). Patients with progressive disease often experience fissures, cracking, and abrasions, leading to scarring and a distortion of genital anatomy.5
Extragenital lesions are typically located on the inner thighs, submammary areas, neck, shoulders, and wrists (Figures 1 and 2). However, cases of infraorbital, eyelid, nail, and oral mucosal lesions have been reported.4,6 Morphologically, lesions are typically white opalescent atrophic papules that may coalesce into plaques and result in tissue-paper like skin. Described clinical variants include widespread guttate, zosteriform, and lichen planus-like lesions.1,7-9
Recently, with the advancement of noninvasive imaging modalities in dermatology, features of LSA on dermoscopy and confocal microscopy have been described. When biopsy is not possible or would rather be avoided (as in young children or in cosmetically sensitive areas), these modalities may be used to make the diagnosis of LSA. Dermoscopy demonstrates a well-demarcated, homogenous, whitish plaque with yellow circles akin to comedo-like openings. Furthermore, confocal microscopy reveals hyperkeratosis, atrophy of the epidermis, dark and round structures containing bright amorphous material, and coarse collagen in bundles.10
Epidemiology
Lichen sclerosus occurs in patients of all ages, with cases reported in patients as young as 6 months. There is a bimodal peak of incidence in prepubertal children and postmenopausal women, respectively, and in middle-aged men. LSA disproportionately affects women with the female to male ratio ranging from 10:1 to 5:1.11 Unfortunately, the exact prevalence of LSA is difficult to determine given that patients often present to different providers, including dermatologists, pediatricians, gynecologists, and urologists.12 The prevalence of LSA is estimated to range from 1 in 300 to 1 in 1000.4
Pathogenesis
Although the etiology of LSA is unknown, several mechanisms have been proposed to explain this disease, including autoimmune, genetic, infectious, and hormonal factors.11
Autoimmune and Genetic
A significant amount of autoimmune diseases are found in association with LSA; these being thyroid disease, pernicious anemia, diabetes mellitus, vitiligo, alopecia areata, and systemic lupus erythematosus.13 The frequency of these co-occurring has been described between 21% to 74% in women, however, only approximately 6% in men.12 Furthermore, circulating IgG autoantibodies that target extracellular matrix 1 protein can be found in 74% of women with genital LSA.14 Autoantibodies targeting BP180 and BP230, basement membrane zone proteins, have also been described in patients with vulvar LSA.15
In an observational study of 1052 female patients with vulvar LSA, 12% of patients had a positive family history. HLA-DQ7, HLA-DQ8, and DQ9 have been found to be most frequently associated with LSA.16,17
Infectious
Several infectious agents have been considered to have a role in the pathogenesis of LSA. Investigations into the role of Borrelia species have shown conflicting results; serology and polymerase chain reaction (PCR) testing have not been able to conclusively link Borrelia to LSA.18,19
Viral infections, such as Epstein-Barr virus (EBV) and human papilloma virus (HPV), have also been investigated. EBV DNA has been found in 26.5% of 34 patients with vulvar LSA on biopsy. However, further studies are necessary to confirm this association.20
The evidence for HPV infection has also been conflicting, with some reports showing high incidence of HPV PCR in LSA lesion and other showing no association.21,22
Hormonal
Given the high incidence of LSA in women with low estrogen states, such as prepubertal girls and postmenopausal women, hormonal factors have been considered to play a role in the development of LSA.13 Through investigation of punch biopsy specimens in patients with vulvar LSA, no evidence of altered hormone receptors were found in a study of 39 specimens.23 Conversely, in a study examining oral contraceptive use in patients with LSA, 100% were found to be on oral contraceptive pills compared with approximately 66% of controls.24
Article continues on page 3
{{pagebreak}}
Differential Diagnosis
Several diagnoses need to be considered in patients with a clinical presentation consistent with LSA. In women, the differential diagnosis of genital lesions includes lichen planus, vitiligo, lichen simplex chronicus, immunobullous diseases, and vulvar intraepithelial neoplasia. In men, erythroplasia of Queyrat, lichen planus, leukoplakia, and scleroderma must be considered.4,11 For extragenital lesions, morphea, atrophic lichen planus, and discoid lupus erythematosus may appear clinically similar.11 Interestingly, a case of interstitial mycoses fungoides masquerading as LSA, both clinically and histologically, was reported by Tekin and colleagues.25
Treatment
A systematic review and meta-analysis of randomized controlled trials on topical treatment for genital lichen sclerosus was performed to outline the most effective therapies. High-potency topical steroids (ie, clobetasol propionate, 0.05%) remain the most effective treatments available for patients when compared with placebo, without the risk of adverse effects. Pimecrolimus 1% cream has been shown to be effective for the improvement of symptoms, however, less so than clobetasol propionate, 0.05%. Topical testosterone, dihydrotestosterone, and progesterone have not shown to be effective.26
For extragenital disease, case reports confirm that topical clobetasol will improve blistering and hemorrhage, if present, but will have no effect on the atrophic plaque.27 Other treatments reported to have success in case reports and small trials include tacrolimus, calcipotriene, acitretin, carbon dioxide laser therapy, phototherapy, and pulse dye laser.27-30
Our Patient
The initial clinical presentation in our patient favored extragenital lichen sclerosus given the morphology of the lesions and their characteristic distribution. The patient did not have genital involvement. However, other diagnoses were considered and given that lichen sclerosus is a chronic disease, a skin biopsy was performed.
Histologic evaluation showed fibrosis within the papillary and superficial reticular dermis with smudging of the collagen bundles, an interstitial lymphohistiocytic infiltrate below the area of fibrosis, and follicular plugging (Figures 3 and 4). These findings were consistent with early extragenital lichen sclerosus. The patient was treated with high-potency topical steroids with significant improvement on follow-up.
Conclusion
Lichen sclerosus is a chronic, skin limited disease that can cause significant symptoms, disfigurement, and disability. Although etiology is still uncertain, autoimmune and genetic factors seem to play a significant role in the pathogenesis of this disease. While diagnosis is clinical with histologic confirmation, noninvasive imaging modalities such as dermoscopy and confocal microscopy may begin to play a significant role. High-potency topical corticosteroids and calcineurin inhibitors remain the mainstay of treatment for patients with this disease.
Dr Fisher is a second-year dermatology resident in the department of dermatology at SUNY Downstate Medical Center in Brooklyn, NY.
Dr Khachemoune, the Section Editor of Derm DX, is with the department of dermatology at Veteran Affairs Medical Center, and the department of dermatology at the State University of New York Downstate, both in Brooklyn, NY.
Acknowledgment: We thank Dr Edward Heilman for reviewing the histopathology slides and description for this case.
Disclosure: The authors report no relevant financial relationships.
References
1. Ganesan L, Parmar H, Das JK, Gangopadhyay A. Extragenital lichen sclerosus et atrophicus. Indian J Dermatol. 2015;60(4):420.
2. Cooper S, Wojnarowska F. Anogenital (non-venereal) disease. In: Jorizzo J, Schaffer J Bolognia J, eds. Dermatology. 3rd ed. New York, NY: Elsevier; 2012:chap 73.
3. Yu L, Li Z, Feng S. Lichen sclerosus of face: a case report and review of literature. Indian J Dermatol. 2016;61(1):120.
4. Pugliese JM, Morey AF, Peterson AC. Lichen sclerosus: review of the literature and current recommendations for management. J Urol. 2007;178(6):2268-2276.
5. Val I, Almeida G. An overview of lichen sclerosus. Clin Obstet Gynecol. 2005;48(4):808-817.
6. Radke PM, Maltry AC, Mokhtarzadeh A, Harrison AR. A unique ocular presentation of extragenital lichen sclerosus [published online March 1, 2016]. Ophthal Plast Reconstr Surg. doi:10.1097/IOP.0000000000000662
7. Jayasekera PS, Parslew RA, McPartland J. An unusual pediatric presentation of guttate atrophic lesions on the trunk [published online March 5, 2016]. Int J Dermatol. doi:10.1111/ijd.13269
8. Vázquez MG, Navarra R, Martin-Urda MT, Abellaneda C, Quer A. Lichen sclerosus et atrophicus with cutaneous distribution simulating lichen planus. Case Rep Dermatol. 2010;2(1):55-59.
9. Chen JF, Chiang CP, Chen YF. Bilateral zosteriform extragenital lichen sclerosus et atrophicus: a new clinical presentation. J Dermatol. 2010;37(5):480-483.
10. Lacarrubba F, Pellacani G, Verzì AE, Pippione M, Micali G. Extragenital lichen sclerosus: clinical, dermoscopic, confocal microscopy and histologic correlations. J Am Acad Dermatol. 2015;72(1 suppl):S50-S52.
11. Yesudian PD, Sugunendran H, Bates CM, O’Mahony C. Lichen sclerosus. Int J STD AIDS. 2005;16(7):465-473.
12. Fistarol SK, Itin PH. Diagnosis and treatment of lichen sclerosus: an update. Am J Clin Dermatol. 2013;14(1):27-47.
13. Meyrick Thomas RH, Ridley CM, McGibbon DH, Black MM. Lichen sclerosus et atrophicus and autoimmunity—a study of 350 women. Br J Dermatol. 1988;118(1):41-46.
14. Oyama N, Chan I, Neill SM, et al. Autoantibodies to extracellular matrix protein 1 in lichen sclerosus. Lancet 2003;362(9378):118-123.
15. Howard A, Dean D, Cooper S, Kirtshig G, Wojnarowska F. Circulating basement membrane zone antibodies are found in lichen sclerosus of the vulva. Australas J Dermatol. 2004;45(1):12-15.
16. Sherman V, McPherson T, Baldo M, Salim A, Gao XH, Wojnarowska F. The high rate of familial lichen sclerosus suggests a genetic contribution: an observational cohort study. J Eur Acad Dermatol Venereol. 2010;24(9):1031-1034.
17. Marren P, Yell J, Chamock FM, Bunce M, Welsh K, Wojnarowska F. The association between lichen sclerosus and antigens of the HLA system. Br J Dermatol. 1995;132(2):197-203.
18. Edmonds E, Mavin S, Francis N, Ho-Yen D, Bunker C. Borrelia burgdorferi is not associated with genital lichen sclerosus in men. Br J Dermatol. 2009;160(2):459-460.
19. Weide B, Walz T, Garbe C. Is morphoea caused by Borrelia burgdorferi? A review. Br J Dermatol. 2000;142(4):636-44.
20. Aidé S, Lattario FR, Almeida G, do Val IC, da Costa Carvalho M. Epstein-Barr virus and human papillomavirus infection in vulvar lichen sclerosus. J Low Genit Tract Dis. 2010;14(4):319-322.
21. Drut RM, Gómez MA, Drut R, Lojo MM. Human papillomavirus is present in some cases of childhood penile lichen sclerosus: an in situ hybridization and SP-PCR study. Pediatr Dermatol. 1998;15(2):85-90.
22. Neill SM, Lessana-Leibowitch M, Pelisse M, Moyal-Barracco M. Lichen sclerosus, invasive squamous cell carcinoma, and human papillomavirus. Am J Obstet Gynecol. 1990;162(6):1633-1634.
23. Kohlberger PD, Joura EA, Bancher D, Gitsch G, Breitenecker G, Kieback DG. Evidence of androgen receptor expression in lichen sclerosus: an immunohistochemical study. J Soc Gynecol Investig. 1998;5(6):331-333.
24. Günthert AR, Faber M, Knappe G, Hellriegel S, Emons G. Early onset vulvar lichen sclerosus in premenopausal women and oral contraceptives. Eur J Obstet Gynecol Reprod Biol. 2008;137(1):56-60.
25. Tekin B, Kempf W, Seckin D, Ergun T, Yucelten D, Demirkessen C. Interstitial mycosis fungoides with lichen sclerosus-like clinical and histopathological features. Am J Dermatopathol. 2016;38(2):138-143.
26. Chi CC, Kirtschig G, Baldo M, Lewis F, Wang SH, Wojnarowska F. Systematic review and meta-analysis of randomized controlled trials on topical interventions for genital lichen sclerosus. J Am Acad Dermatol. 2012;67(2):305-312.
27. Shiver M, Papasakelariou C, Brown JA, Wirges M, Kincannon J. Extragenital bullous lichen sclerosus in a pediatric patient: a case report and literature review. Pediatr Dermatol. 2014;31(3):383-355.
28. Bergstrom KG, Mengden SJ, Kamino H, Ramsay D. Extragenital lichen sclerosus et atrophicus. Dermatol Online J. 2008;14(5):23.
29. Kim GW, Park HJ, Kim HS, et al. Topical tacrolimus ointment for the treatment of lichen sclerosus, comparing genital and extragenital involvement. J Dermatol. 2012;39(2):145-150.
30. Formiga Ade A, Torres Ide S, Rocha Bde O, et al. Disseminated extragenital lichen sclerosus et atrophicus treated with acitretin. Skinmed 2014;12(1):62-63.
Diagnosis: Extragential Lichen Sclerosus et Atrophicus
Lichen sclerosus et atrophicus (LSA), originally described by Francois Henri Hallopeau in 1887, is a chronic inflammatory disease of unclear pathogenesis which affects both the epidermis and the dermis.1 The typical clinical presentation of LSA is in the anogenital area, occurring in at least 85% of cases.2 However, extragenital disease is not uncommon and can be found in as many as 15% to 20% of patients.3
Clinical Presentation
In both men and women, the clinical presentation of LSA is variable and may be insidious or aggressive. In women, it commonly affects the anogenital region. In men, however, involvement is limited to the glans and foreskin. Physical examination findings are classically described as “figure of eight” in female patients, indicating skin changes are seen around the vulva and anus in patches or plaques, with fragile, thinned, and atrophic skin. Similar lesions, grey-white in color, are seen on the glans or prepuce of men and can progress to involve the frenulum, leading to nonretractable foreskin and phimosis.4
Pruritus is the most common presenting symptom, with a tendency to be worse at night. In addition, patients report skin tenderness, burning, dysuria, dyspareunia, pain with defecation, and difficulty retracting the foreskin (in men). Patients with progressive disease often experience fissures, cracking, and abrasions, leading to scarring and a distortion of genital anatomy.5
Extragenital lesions are typically located on the inner thighs, submammary areas, neck, shoulders, and wrists (Figures 1 and 2). However, cases of infraorbital, eyelid, nail, and oral mucosal lesions have been reported.4,6 Morphologically, lesions are typically white opalescent atrophic papules that may coalesce into plaques and result in tissue-paper like skin. Described clinical variants include widespread guttate, zosteriform, and lichen planus-like lesions.1,7-9
Recently, with the advancement of noninvasive imaging modalities in dermatology, features of LSA on dermoscopy and confocal microscopy have been described. When biopsy is not possible or would rather be avoided (as in young children or in cosmetically sensitive areas), these modalities may be used to make the diagnosis of LSA. Dermoscopy demonstrates a well-demarcated, homogenous, whitish plaque with yellow circles akin to comedo-like openings. Furthermore, confocal microscopy reveals hyperkeratosis, atrophy of the epidermis, dark and round structures containing bright amorphous material, and coarse collagen in bundles.10
Epidemiology
Lichen sclerosus occurs in patients of all ages, with cases reported in patients as young as 6 months. There is a bimodal peak of incidence in prepubertal children and postmenopausal women, respectively, and in middle-aged men. LSA disproportionately affects women with the female to male ratio ranging from 10:1 to 5:1.11 Unfortunately, the exact prevalence of LSA is difficult to determine given that patients often present to different providers, including dermatologists, pediatricians, gynecologists, and urologists.12 The prevalence of LSA is estimated to range from 1 in 300 to 1 in 1000.4
Pathogenesis
Although the etiology of LSA is unknown, several mechanisms have been proposed to explain this disease, including autoimmune, genetic, infectious, and hormonal factors.11
Autoimmune and Genetic
A significant amount of autoimmune diseases are found in association with LSA; these being thyroid disease, pernicious anemia, diabetes mellitus, vitiligo, alopecia areata, and systemic lupus erythematosus.13 The frequency of these co-occurring has been described between 21% to 74% in women, however, only approximately 6% in men.12 Furthermore, circulating IgG autoantibodies that target extracellular matrix 1 protein can be found in 74% of women with genital LSA.14 Autoantibodies targeting BP180 and BP230, basement membrane zone proteins, have also been described in patients with vulvar LSA.15
In an observational study of 1052 female patients with vulvar LSA, 12% of patients had a positive family history. HLA-DQ7, HLA-DQ8, and DQ9 have been found to be most frequently associated with LSA.16,17
Infectious
Several infectious agents have been considered to have a role in the pathogenesis of LSA. Investigations into the role of Borrelia species have shown conflicting results; serology and polymerase chain reaction (PCR) testing have not been able to conclusively link Borrelia to LSA.18,19
Viral infections, such as Epstein-Barr virus (EBV) and human papilloma virus (HPV), have also been investigated. EBV DNA has been found in 26.5% of 34 patients with vulvar LSA on biopsy. However, further studies are necessary to confirm this association.20
The evidence for HPV infection has also been conflicting, with some reports showing high incidence of HPV PCR in LSA lesion and other showing no association.21,22
Hormonal
Given the high incidence of LSA in women with low estrogen states, such as prepubertal girls and postmenopausal women, hormonal factors have been considered to play a role in the development of LSA.13 Through investigation of punch biopsy specimens in patients with vulvar LSA, no evidence of altered hormone receptors were found in a study of 39 specimens.23 Conversely, in a study examining oral contraceptive use in patients with LSA, 100% were found to be on oral contraceptive pills compared with approximately 66% of controls.24
Article continues on page 3
{{pagebreak}}
Differential Diagnosis
Several diagnoses need to be considered in patients with a clinical presentation consistent with LSA. In women, the differential diagnosis of genital lesions includes lichen planus, vitiligo, lichen simplex chronicus, immunobullous diseases, and vulvar intraepithelial neoplasia. In men, erythroplasia of Queyrat, lichen planus, leukoplakia, and scleroderma must be considered.4,11 For extragenital lesions, morphea, atrophic lichen planus, and discoid lupus erythematosus may appear clinically similar.11 Interestingly, a case of interstitial mycoses fungoides masquerading as LSA, both clinically and histologically, was reported by Tekin and colleagues.25
Treatment
A systematic review and meta-analysis of randomized controlled trials on topical treatment for genital lichen sclerosus was performed to outline the most effective therapies. High-potency topical steroids (ie, clobetasol propionate, 0.05%) remain the most effective treatments available for patients when compared with placebo, without the risk of adverse effects. Pimecrolimus 1% cream has been shown to be effective for the improvement of symptoms, however, less so than clobetasol propionate, 0.05%. Topical testosterone, dihydrotestosterone, and progesterone have not shown to be effective.26
For extragenital disease, case reports confirm that topical clobetasol will improve blistering and hemorrhage, if present, but will have no effect on the atrophic plaque.27 Other treatments reported to have success in case reports and small trials include tacrolimus, calcipotriene, acitretin, carbon dioxide laser therapy, phototherapy, and pulse dye laser.27-30
Our Patient
The initial clinical presentation in our patient favored extragenital lichen sclerosus given the morphology of the lesions and their characteristic distribution. The patient did not have genital involvement. However, other diagnoses were considered and given that lichen sclerosus is a chronic disease, a skin biopsy was performed.
Histologic evaluation showed fibrosis within the papillary and superficial reticular dermis with smudging of the collagen bundles, an interstitial lymphohistiocytic infiltrate below the area of fibrosis, and follicular plugging (Figures 3 and 4). These findings were consistent with early extragenital lichen sclerosus. The patient was treated with high-potency topical steroids with significant improvement on follow-up.
Conclusion
Lichen sclerosus is a chronic, skin limited disease that can cause significant symptoms, disfigurement, and disability. Although etiology is still uncertain, autoimmune and genetic factors seem to play a significant role in the pathogenesis of this disease. While diagnosis is clinical with histologic confirmation, noninvasive imaging modalities such as dermoscopy and confocal microscopy may begin to play a significant role. High-potency topical corticosteroids and calcineurin inhibitors remain the mainstay of treatment for patients with this disease.
Dr Fisher is a second-year dermatology resident in the department of dermatology at SUNY Downstate Medical Center in Brooklyn, NY.
Dr Khachemoune, the Section Editor of Derm DX, is with the department of dermatology at Veteran Affairs Medical Center, and the department of dermatology at the State University of New York Downstate, both in Brooklyn, NY.
Acknowledgment: We thank Dr Edward Heilman for reviewing the histopathology slides and description for this case.
Disclosure: The authors report no relevant financial relationships.
References
1. Ganesan L, Parmar H, Das JK, Gangopadhyay A. Extragenital lichen sclerosus et atrophicus. Indian J Dermatol. 2015;60(4):420.
2. Cooper S, Wojnarowska F. Anogenital (non-venereal) disease. In: Jorizzo J, Schaffer J Bolognia J, eds. Dermatology. 3rd ed. New York, NY: Elsevier; 2012:chap 73.
3. Yu L, Li Z, Feng S. Lichen sclerosus of face: a case report and review of literature. Indian J Dermatol. 2016;61(1):120.
4. Pugliese JM, Morey AF, Peterson AC. Lichen sclerosus: review of the literature and current recommendations for management. J Urol. 2007;178(6):2268-2276.
5. Val I, Almeida G. An overview of lichen sclerosus. Clin Obstet Gynecol. 2005;48(4):808-817.
6. Radke PM, Maltry AC, Mokhtarzadeh A, Harrison AR. A unique ocular presentation of extragenital lichen sclerosus [published online March 1, 2016]. Ophthal Plast Reconstr Surg. doi:10.1097/IOP.0000000000000662
7. Jayasekera PS, Parslew RA, McPartland J. An unusual pediatric presentation of guttate atrophic lesions on the trunk [published online March 5, 2016]. Int J Dermatol. doi:10.1111/ijd.13269
8. Vázquez MG, Navarra R, Martin-Urda MT, Abellaneda C, Quer A. Lichen sclerosus et atrophicus with cutaneous distribution simulating lichen planus. Case Rep Dermatol. 2010;2(1):55-59.
9. Chen JF, Chiang CP, Chen YF. Bilateral zosteriform extragenital lichen sclerosus et atrophicus: a new clinical presentation. J Dermatol. 2010;37(5):480-483.
10. Lacarrubba F, Pellacani G, Verzì AE, Pippione M, Micali G. Extragenital lichen sclerosus: clinical, dermoscopic, confocal microscopy and histologic correlations. J Am Acad Dermatol. 2015;72(1 suppl):S50-S52.
11. Yesudian PD, Sugunendran H, Bates CM, O’Mahony C. Lichen sclerosus. Int J STD AIDS. 2005;16(7):465-473.
12. Fistarol SK, Itin PH. Diagnosis and treatment of lichen sclerosus: an update. Am J Clin Dermatol. 2013;14(1):27-47.
13. Meyrick Thomas RH, Ridley CM, McGibbon DH, Black MM. Lichen sclerosus et atrophicus and autoimmunity—a study of 350 women. Br J Dermatol. 1988;118(1):41-46.
14. Oyama N, Chan I, Neill SM, et al. Autoantibodies to extracellular matrix protein 1 in lichen sclerosus. Lancet 2003;362(9378):118-123.
15. Howard A, Dean D, Cooper S, Kirtshig G, Wojnarowska F. Circulating basement membrane zone antibodies are found in lichen sclerosus of the vulva. Australas J Dermatol. 2004;45(1):12-15.
16. Sherman V, McPherson T, Baldo M, Salim A, Gao XH, Wojnarowska F. The high rate of familial lichen sclerosus suggests a genetic contribution: an observational cohort study. J Eur Acad Dermatol Venereol. 2010;24(9):1031-1034.
17. Marren P, Yell J, Chamock FM, Bunce M, Welsh K, Wojnarowska F. The association between lichen sclerosus and antigens of the HLA system. Br J Dermatol. 1995;132(2):197-203.
18. Edmonds E, Mavin S, Francis N, Ho-Yen D, Bunker C. Borrelia burgdorferi is not associated with genital lichen sclerosus in men. Br J Dermatol. 2009;160(2):459-460.
19. Weide B, Walz T, Garbe C. Is morphoea caused by Borrelia burgdorferi? A review. Br J Dermatol. 2000;142(4):636-44.
20. Aidé S, Lattario FR, Almeida G, do Val IC, da Costa Carvalho M. Epstein-Barr virus and human papillomavirus infection in vulvar lichen sclerosus. J Low Genit Tract Dis. 2010;14(4):319-322.
21. Drut RM, Gómez MA, Drut R, Lojo MM. Human papillomavirus is present in some cases of childhood penile lichen sclerosus: an in situ hybridization and SP-PCR study. Pediatr Dermatol. 1998;15(2):85-90.
22. Neill SM, Lessana-Leibowitch M, Pelisse M, Moyal-Barracco M. Lichen sclerosus, invasive squamous cell carcinoma, and human papillomavirus. Am J Obstet Gynecol. 1990;162(6):1633-1634.
23. Kohlberger PD, Joura EA, Bancher D, Gitsch G, Breitenecker G, Kieback DG. Evidence of androgen receptor expression in lichen sclerosus: an immunohistochemical study. J Soc Gynecol Investig. 1998;5(6):331-333.
24. Günthert AR, Faber M, Knappe G, Hellriegel S, Emons G. Early onset vulvar lichen sclerosus in premenopausal women and oral contraceptives. Eur J Obstet Gynecol Reprod Biol. 2008;137(1):56-60.
25. Tekin B, Kempf W, Seckin D, Ergun T, Yucelten D, Demirkessen C. Interstitial mycosis fungoides with lichen sclerosus-like clinical and histopathological features. Am J Dermatopathol. 2016;38(2):138-143.
26. Chi CC, Kirtschig G, Baldo M, Lewis F, Wang SH, Wojnarowska F. Systematic review and meta-analysis of randomized controlled trials on topical interventions for genital lichen sclerosus. J Am Acad Dermatol. 2012;67(2):305-312.
27. Shiver M, Papasakelariou C, Brown JA, Wirges M, Kincannon J. Extragenital bullous lichen sclerosus in a pediatric patient: a case report and literature review. Pediatr Dermatol. 2014;31(3):383-355.
28. Bergstrom KG, Mengden SJ, Kamino H, Ramsay D. Extragenital lichen sclerosus et atrophicus. Dermatol Online J. 2008;14(5):23.
29. Kim GW, Park HJ, Kim HS, et al. Topical tacrolimus ointment for the treatment of lichen sclerosus, comparing genital and extragenital involvement. J Dermatol. 2012;39(2):145-150.
30. Formiga Ade A, Torres Ide S, Rocha Bde O, et al. Disseminated extragenital lichen sclerosus et atrophicus treated with acitretin. Skinmed 2014;12(1):62-63.













