This new column was created to enhance your dermatopathology education and skills. Take the quiz and check your work on below or the PDF.
Please click here to download quiz (PDF)

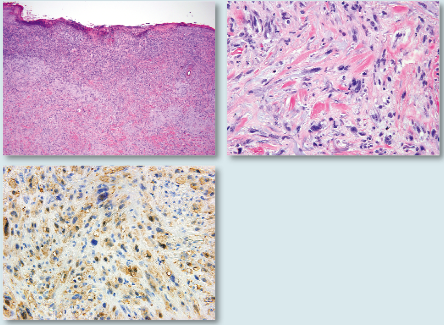
CASE 1. These images best represent:
a. Epithelioid sarcoma
b. Desmoplastic malignant melanoma
c. Dermatofibroma
d. Dermatofibrosarcoma protuberans

Case 2. These images
best represent:
a. Contact dermatitis
b. Bullous pemphigoid
c. Toxic epidermal necrolysis
d. Erythema multiforme

Case 3. These images best represent:
a. Granuloma annulare
b. Necrobiosis lipoidica
c. Tuberculoid leprosy
d. Cutaneous tuberculosis

Case 4. These images best represent:
a. Bullous pemphigoid
b. Grover’s disease
c. Hailey-Hailey disease
d. Herpes simplex virus infection

Case 5. These images
best represent:
a. Keratosis pilaris
b. Superficial chronic folliculitis
c. Discoid lesion of chronic lupus erythematosus
d. Porokeratosis
Case 1 — b
These sections show desmoplastic malignant melanoma (DMM). The salient features of DMM pathology include spindle, and sometimes nevoid, atypical cells in the dermis embedded in a desmoplastic stroma. An overlying melanocytic proliferation may be seen in the epidermis. Dermal spindle cells are usually haphazardly arranged and show enlarged hyperchromatic nuclei with mitotic figures. Neurotropism with spindle cells extending in and around small cutaneous nerves may be seen. Patchy lymphocytic infiltrates are classically described around the tumor. S100 staining is usually positive.
Case 2 — d
These sections show erythema multiforme (EM). The salient features of EM include vacuolar degeneration of the basal layer with necrotic keratinocytes within the epidermis and a lichenoid lymphocytic infiltrate along the basal layer of the epidermis. Eosinophils may also be seen in the infiltrate. Vesiculation may also be seen in bullous EM. The stratum corneum is usually basket weave, denoting the acute nature of this entity. Full thickness necrosis is not seen, as would be with toxic epidermal necrolysis.
Case 3 — a
These sections show granuloma annulare (GA). The classic features of GA are that of a palisading granuloma, with a dermal granulomatous infiltrate composed of lymphocytes and histiocytes, surrounding an area of degenerated collagen and elastic fibers (“necrobiosis”), and dermal mucin deposition. In interstitial GA, the most common histologic pattern areas of collagen degeneration may not be seen and histiocytic infiltrates are present between collagen bundles. Mucin is often not seen on the H&E stain, but separated collagen bundles can serve as a clue of its presence. Scattered eosinophils may also be seen in the infiltrate. While palisading granulomas with “necrobiosis” are also seen in necrobiosis lipoidica, these are usually layered and span the dermis and involve subcutaneous fat; plasma cells are also characteristic in the infiltrate; mucin deposition is usually absent.
Case 4 — b
These sections show Grover’s disease (transient and persistent acantholytic dermatosis). Four histologic patterns are possible in Grover’s disease (GD): resembling Darier’s disease, Hailey-Hailey disease, pemphigus vulgaris (PV), and spongiosis with acntholysis. These sections show a Darier’s disease pattern, with acantholysis in the epidermis with prominent dyskeratosis (corp ronds and grains). Follicular involvement by acantholysis is not seen, as would be in PV. Hailey-Hailey usually lacks the level of dyskeratosis of Darier’s disease pattern and shows a “dilapidated brick wall” appearance.
Case 5 - a
These sections show keratosis pilaris (KP). The salient features include a follicular plug with parakeratosis, projecting from the follicular opening,
epidermal hyperkeratosis and hypergranulosis. Perifollicular infiltrates may be seen, especially if there is follicular rupture secondary to plugging. Similar histology is seen in lichen spinulosus.

CASE 1. These images best represent:
a. Epithelioid sarcoma
b. Desmoplastic malignant melanoma
c. Dermatofibroma
d. Dermatofibrosarcoma protuberans

Case 2. These images
best represent:
a. Contact dermatitis
b. Bullous pemphigoid
c. Toxic epidermal necrolysis
d. Erythema multiforme

Case 3. These images best represent:
a. Granuloma annulare
b. Necrobiosis lipoidica
c. Tuberculoid leprosy
d. Cutaneous tuberculosis

Case 4. These images best represent:
a. Bullous pemphigoid
b. Grover’s disease
c. Hailey-Hailey disease
d. Herpes simplex virus infection

Case 5. These images
best represent:
a. Keratosis pilaris
b. Superficial chronic folliculitis
c. Discoid lesion of chronic lupus erythematosus
d. Porokeratosis
Case 1 — b
These sections show desmoplastic malignant melanoma (DMM). The salient features of DMM pathology include spindle, and sometimes nevoid, atypical cells in the dermis embedded in a desmoplastic stroma. An overlying melanocytic proliferation may be seen in the epidermis. Dermal spindle cells are usually haphazardly arranged and show enlarged hyperchromatic nuclei with mitotic figures. Neurotropism with spindle cells extending in and around small cutaneous nerves may be seen. Patchy lymphocytic infiltrates are classically described around the tumor. S100 staining is usually positive.
Case 2 — d
These sections show erythema multiforme (EM). The salient features of EM include vacuolar degeneration of the basal layer with necrotic keratinocytes within the epidermis and a lichenoid lymphocytic infiltrate along the basal layer of the epidermis. Eosinophils may also be seen in the infiltrate. Vesiculation may also be seen in bullous EM. The stratum corneum is usually basket weave, denoting the acute nature of this entity. Full thickness necrosis is not seen, as would be with toxic epidermal necrolysis.
Case 3 — a
These sections show granuloma annulare (GA). The classic features of GA are that of a palisading granuloma, with a dermal granulomatous infiltrate composed of lymphocytes and histiocytes, surrounding an area of degenerated collagen and elastic fibers (“necrobiosis”), and dermal mucin deposition. In interstitial GA, the most common histologic pattern areas of collagen degeneration may not be seen and histiocytic infiltrates are present between collagen bundles. Mucin is often not seen on the H&E stain, but separated collagen bundles can serve as a clue of its presence. Scattered eosinophils may also be seen in the infiltrate. While palisading granulomas with “necrobiosis” are also seen in necrobiosis lipoidica, these are usually layered and span the dermis and involve subcutaneous fat; plasma cells are also characteristic in the infiltrate; mucin deposition is usually absent.
Case 4 — b
These sections show Grover’s disease (transient and persistent acantholytic dermatosis). Four histologic patterns are possible in Grover’s disease (GD): resembling Darier’s disease, Hailey-Hailey disease, pemphigus vulgaris (PV), and spongiosis with acntholysis. These sections show a Darier’s disease pattern, with acantholysis in the epidermis with prominent dyskeratosis (corp ronds and grains). Follicular involvement by acantholysis is not seen, as would be in PV. Hailey-Hailey usually lacks the level of dyskeratosis of Darier’s disease pattern and shows a “dilapidated brick wall” appearance.
Case 5 - a
These sections show keratosis pilaris (KP). The salient features include a follicular plug with parakeratosis, projecting from the follicular opening,
epidermal hyperkeratosis and hypergranulosis. Perifollicular infiltrates may be seen, especially if there is follicular rupture secondary to plugging. Similar histology is seen in lichen spinulosus.
CASE 1. These images best represent:
a. Epithelioid sarcoma
b. Desmoplastic malignant melanoma
c. Dermatofibroma
d. Dermatofibrosarcoma protuberans
Case 2. These images
best represent:
a. Contact dermatitis
b. Bullous pemphigoid
c. Toxic epidermal necrolysis
d. Erythema multiforme
Case 3. These images best represent:
a. Granuloma annulare
b. Necrobiosis lipoidica
c. Tuberculoid leprosy
d. Cutaneous tuberculosis
Case 4. These images best represent:
a. Bullous pemphigoid
b. Grover’s disease
c. Hailey-Hailey disease
d. Herpes simplex virus infection
Case 5. These images
best represent:
a. Keratosis pilaris
b. Superficial chronic folliculitis
c. Discoid lesion of chronic lupus erythematosus
d. Porokeratosis
Case 1 — b
These sections show desmoplastic malignant melanoma (DMM). The salient features of DMM pathology include spindle, and sometimes nevoid, atypical cells in the dermis embedded in a desmoplastic stroma. An overlying melanocytic proliferation may be seen in the epidermis. Dermal spindle cells are usually haphazardly arranged and show enlarged hyperchromatic nuclei with mitotic figures. Neurotropism with spindle cells extending in and around small cutaneous nerves may be seen. Patchy lymphocytic infiltrates are classically described around the tumor. S100 staining is usually positive.
Case 2 — d
These sections show erythema multiforme (EM). The salient features of EM include vacuolar degeneration of the basal layer with necrotic keratinocytes within the epidermis and a lichenoid lymphocytic infiltrate along the basal layer of the epidermis. Eosinophils may also be seen in the infiltrate. Vesiculation may also be seen in bullous EM. The stratum corneum is usually basket weave, denoting the acute nature of this entity. Full thickness necrosis is not seen, as would be with toxic epidermal necrolysis.
Case 3 — a
These sections show granuloma annulare (GA). The classic features of GA are that of a palisading granuloma, with a dermal granulomatous infiltrate composed of lymphocytes and histiocytes, surrounding an area of degenerated collagen and elastic fibers (“necrobiosis”), and dermal mucin deposition. In interstitial GA, the most common histologic pattern areas of collagen degeneration may not be seen and histiocytic infiltrates are present between collagen bundles. Mucin is often not seen on the H&E stain, but separated collagen bundles can serve as a clue of its presence. Scattered eosinophils may also be seen in the infiltrate. While palisading granulomas with “necrobiosis” are also seen in necrobiosis lipoidica, these are usually layered and span the dermis and involve subcutaneous fat; plasma cells are also characteristic in the infiltrate; mucin deposition is usually absent.
Case 4 — b
These sections show Grover’s disease (transient and persistent acantholytic dermatosis). Four histologic patterns are possible in Grover’s disease (GD): resembling Darier’s disease, Hailey-Hailey disease, pemphigus vulgaris (PV), and spongiosis with acntholysis. These sections show a Darier’s disease pattern, with acantholysis in the epidermis with prominent dyskeratosis (corp ronds and grains). Follicular involvement by acantholysis is not seen, as would be in PV. Hailey-Hailey usually lacks the level of dyskeratosis of Darier’s disease pattern and shows a “dilapidated brick wall” appearance.
Case 5 - a
These sections show keratosis pilaris (KP). The salient features include a follicular plug with parakeratosis, projecting from the follicular opening,
epidermal hyperkeratosis and hypergranulosis. Perifollicular infiltrates may be seen, especially if there is follicular rupture secondary to plugging. Similar histology is seen in lichen spinulosus.