

Case Study
Key Pearls For Treating Haglund’s Deformity In Runners
May 2014
This author offers insights on the surgical treatment of a 43-year-old runner with pain in her posterior Achilles tendon that had not responded to conservative treatment.
 Pain in the posterior portion of the heel can result from various pathologies such as Haglund’s deformity, retrocalcaneal bursitis, insertional Achilles tendinopathy and posterior calcaneal exostosis.1 Many times, the pain is secondary to a combination of the aforementioned conditions, which can lead to challenges in therapy, especially in choosing the correct surgical pathway if necessary.1
Pain in the posterior portion of the heel can result from various pathologies such as Haglund’s deformity, retrocalcaneal bursitis, insertional Achilles tendinopathy and posterior calcaneal exostosis.1 Many times, the pain is secondary to a combination of the aforementioned conditions, which can lead to challenges in therapy, especially in choosing the correct surgical pathway if necessary.1
 In my practice, one of the more common causes of posterior heel pain I frequently encounter is the posterior calcaneal exostosis with associated intratendinous calcifications. Depending on the severity and failure or success of conservative care, my treatment for this typically involves resection of the prominence with detachment of the Achilles and debridement of the calcifications followed by reattachment of the Achilles and augmentation with a flexor hallucis longus transfer. I have had cases in which insignificant amounts of prominence went unresected and symptoms persisted so I tend to be more aggressive with my resection. This leads to the need for a transfer of the flexor hallucis longus tendon.
In my practice, one of the more common causes of posterior heel pain I frequently encounter is the posterior calcaneal exostosis with associated intratendinous calcifications. Depending on the severity and failure or success of conservative care, my treatment for this typically involves resection of the prominence with detachment of the Achilles and debridement of the calcifications followed by reattachment of the Achilles and augmentation with a flexor hallucis longus transfer. I have had cases in which insignificant amounts of prominence went unresected and symptoms persisted so I tend to be more aggressive with my resection. This leads to the need for a transfer of the flexor hallucis longus tendon.
 Although Haglund’s deformity is reportedly one of the most common causes of posterior heel pain, I infrequently encounter Haglund's deformity (according to its original description) in my practice.2 In fact, many times, the condition that is often referred to as Haglund's deformity is more of a retrocalcaneal exostosis than a Haglund's deformity.3 A true Haglund's deformity is an enlargement of the posterosuperior prominence of the calcaneus.4,5
Although Haglund’s deformity is reportedly one of the most common causes of posterior heel pain, I infrequently encounter Haglund's deformity (according to its original description) in my practice.2 In fact, many times, the condition that is often referred to as Haglund's deformity is more of a retrocalcaneal exostosis than a Haglund's deformity.3 A true Haglund's deformity is an enlargement of the posterosuperior prominence of the calcaneus.4,5
 Radiographic determination of the deformity occurs by drawing parallel pitch lines over the calcaneus and observing the enlargement extending above to the superior pitch line. The lower parallel pitch line is a straight line drawn tangent to the anterior tubercle, the medial tubercle and the posterior tuberosity. Create the upper parallel pitch line by first drawing a perpendicular line from the first pitch line and superior to the posterior lip of the talar articular facet. Then draw a parallel line from the end of the perpendicular line from the tip of the talus extending posteriorly.6
Radiographic determination of the deformity occurs by drawing parallel pitch lines over the calcaneus and observing the enlargement extending above to the superior pitch line. The lower parallel pitch line is a straight line drawn tangent to the anterior tubercle, the medial tubercle and the posterior tuberosity. Create the upper parallel pitch line by first drawing a perpendicular line from the first pitch line and superior to the posterior lip of the talar articular facet. Then draw a parallel line from the end of the perpendicular line from the tip of the talus extending posteriorly.6
 Surgical treatment may involve open resection, a wedge shape osteotomy known as the Keck and Kelly, or arthroscopic resection.1,5,7
Surgical treatment may involve open resection, a wedge shape osteotomy known as the Keck and Kelly, or arthroscopic resection.1,5,7
 After reviewing radiographs and magnetic resonance imaging (MRI), I was able to establish that she most likely was suffering from a true Haglund’s deformity. Before resorting to surgical intervention, I made an attempt to work with her training patterns. We had her slow her pace down and follow her aerobic pace (her heart rate was well below lactic threshold, which for her was 137 beats per minute (BPM) to ensure she was not overdoing it. She was concerned that she would not be able to get her heart rate this high but after her first run under monitoring, she was blown away to find out how slow she had to run to keep her heart rate this low. While this may not seem important to most practitioners, running too hard too often can lead to overuse injuries, which then get stuck in the chronic phase. She adhered to this principle of training for almost six months before we elected to surgically resect the prominent Haglund’s deformity due to her continued pain with running.
After reviewing radiographs and magnetic resonance imaging (MRI), I was able to establish that she most likely was suffering from a true Haglund’s deformity. Before resorting to surgical intervention, I made an attempt to work with her training patterns. We had her slow her pace down and follow her aerobic pace (her heart rate was well below lactic threshold, which for her was 137 beats per minute (BPM) to ensure she was not overdoing it. She was concerned that she would not be able to get her heart rate this high but after her first run under monitoring, she was blown away to find out how slow she had to run to keep her heart rate this low. While this may not seem important to most practitioners, running too hard too often can lead to overuse injuries, which then get stuck in the chronic phase. She adhered to this principle of training for almost six months before we elected to surgically resect the prominent Haglund’s deformity due to her continued pain with running.
 For this procedure, I took a lateral approach through an incision approximately 4 cm in length. I identified and retracted the Achilles posteriorly. Deep dissection revealed the prominent superoposterior margin of the calcaneus. I excised the associated inflammatory tissue consistent with the retrocalcaneal bursa. After achieving adequate visualization with a Senn retractor, I resected the prominence with an osteotome. I then smoothed the remaining bone with a rasp and palpation revealed no further prominence. There was no further impingement of the posterior calcaneus on the Achilles tendon.
For this procedure, I took a lateral approach through an incision approximately 4 cm in length. I identified and retracted the Achilles posteriorly. Deep dissection revealed the prominent superoposterior margin of the calcaneus. I excised the associated inflammatory tissue consistent with the retrocalcaneal bursa. After achieving adequate visualization with a Senn retractor, I resected the prominence with an osteotome. I then smoothed the remaining bone with a rasp and palpation revealed no further prominence. There was no further impingement of the posterior calcaneus on the Achilles tendon.
 Postoperative care consisted of a posterior splint and non-weightbearing for two weeks followed by weightbearing in a CAM walker. Physical therapy started at three weeks post-surgery and she began spinning on a bicycle at this time as well. I also encourage my patients (especially the runners) to progress toward performing 100 calf raises a day. This doesn't have to be 100 at one time but over the course of a day. She was able to achieve this seven weeks after surgery. After nine weeks post-op, she was able to begin running. At eight months, she is able to run for 30 minutes at a time pain-free in her heel region, which she had not been able to do for over five years.
Postoperative care consisted of a posterior splint and non-weightbearing for two weeks followed by weightbearing in a CAM walker. Physical therapy started at three weeks post-surgery and she began spinning on a bicycle at this time as well. I also encourage my patients (especially the runners) to progress toward performing 100 calf raises a day. This doesn't have to be 100 at one time but over the course of a day. She was able to achieve this seven weeks after surgery. After nine weeks post-op, she was able to begin running. At eight months, she is able to run for 30 minutes at a time pain-free in her heel region, which she had not been able to do for over five years.
 I prefer to do the procedure open as opposed to arthroscopically because I feel I can access the prominence with less trauma through an incision that is slightly larger. The increased exposure allows me to remove any inflammatory bursa with ease and the recovery time is still quick. I think it is important for clinicians to look for a Haglund’s deformity with any heel pain and focus the exam on palpating deep to the anterior portion of the Achilles because even though there may be some retrocalcaneal spurring occurring, the Haglund’s deformity could be the source of the pain. The recovery time is much faster with a simple Haglund’s resection in comparison to detaching the Achilles and reattaching it to remove an exostosis.
Dr. Campitelli is an Adjunct Professor at the Kent State University College of Podiatric Medicine. He is in private practice at North East Ohio Medical Associates.
References
1. Boffeli TJ, Peterson MC. The Keck and Kelly wedge calcaneal osteotomy for Haglund's deformity: a technique for reproducible results. J Foot Ankle Surg. 2012; 51(3):398-401.
2. Johansson KJ, Sarimo JJ, Lempainen LL, Laitala-Leinonen T, Orava SY. Calcific spurs at the insertion of the Achilles tendon: a clinical and histological study. Muscles Ligaments Tendons J. 2013; 2(4):273-7.
3. Kang S, Thordarson DB, Charlton TP. Insertional Achilles tendinitis and Haglund's deformity. Foot Ankle Int. 2012; 33(6):487-91.
4. Haglund P. Beitrag zur Klinik der Achilles tendon. Zeitschr Orthop Chir 1928;49:49–58.
5. Schunck J, Jerosch J. Operative treatment of Haglund’s syndrome. Basics, indications, procedures, surgical techniques, results and problems. J Foot Ankle Surg. 2005; 11(3):123–130.
6. Banks AS, Downey MS, Martin DE, Miller SJ. (2001).Heel Surgery. In McGlamry's Comprehensive Textbook of Foot and Ankle Surgery, third edition volume 1. Lippincott Williams and Wilkins, Philadelphia, p. 443.
7. Frey C. Surgical advancements: arthroscopic alternatives to open procedures: great toe, subtalar joint, Haglund's deformity, and tendoscopy. Foot Ankle Clin. 2009; 14(2):313-39.
I prefer to do the procedure open as opposed to arthroscopically because I feel I can access the prominence with less trauma through an incision that is slightly larger. The increased exposure allows me to remove any inflammatory bursa with ease and the recovery time is still quick. I think it is important for clinicians to look for a Haglund’s deformity with any heel pain and focus the exam on palpating deep to the anterior portion of the Achilles because even though there may be some retrocalcaneal spurring occurring, the Haglund’s deformity could be the source of the pain. The recovery time is much faster with a simple Haglund’s resection in comparison to detaching the Achilles and reattaching it to remove an exostosis.
Dr. Campitelli is an Adjunct Professor at the Kent State University College of Podiatric Medicine. He is in private practice at North East Ohio Medical Associates.
References
1. Boffeli TJ, Peterson MC. The Keck and Kelly wedge calcaneal osteotomy for Haglund's deformity: a technique for reproducible results. J Foot Ankle Surg. 2012; 51(3):398-401.
2. Johansson KJ, Sarimo JJ, Lempainen LL, Laitala-Leinonen T, Orava SY. Calcific spurs at the insertion of the Achilles tendon: a clinical and histological study. Muscles Ligaments Tendons J. 2013; 2(4):273-7.
3. Kang S, Thordarson DB, Charlton TP. Insertional Achilles tendinitis and Haglund's deformity. Foot Ankle Int. 2012; 33(6):487-91.
4. Haglund P. Beitrag zur Klinik der Achilles tendon. Zeitschr Orthop Chir 1928;49:49–58.
5. Schunck J, Jerosch J. Operative treatment of Haglund’s syndrome. Basics, indications, procedures, surgical techniques, results and problems. J Foot Ankle Surg. 2005; 11(3):123–130.
6. Banks AS, Downey MS, Martin DE, Miller SJ. (2001).Heel Surgery. In McGlamry's Comprehensive Textbook of Foot and Ankle Surgery, third edition volume 1. Lippincott Williams and Wilkins, Philadelphia, p. 443.
7. Frey C. Surgical advancements: arthroscopic alternatives to open procedures: great toe, subtalar joint, Haglund's deformity, and tendoscopy. Foot Ankle Clin. 2009; 14(2):313-39.
 Pain in the posterior portion of the heel can result from various pathologies such as Haglund’s deformity, retrocalcaneal bursitis, insertional Achilles tendinopathy and posterior calcaneal exostosis.1 Many times, the pain is secondary to a combination of the aforementioned conditions, which can lead to challenges in therapy, especially in choosing the correct surgical pathway if necessary.1
Pain in the posterior portion of the heel can result from various pathologies such as Haglund’s deformity, retrocalcaneal bursitis, insertional Achilles tendinopathy and posterior calcaneal exostosis.1 Many times, the pain is secondary to a combination of the aforementioned conditions, which can lead to challenges in therapy, especially in choosing the correct surgical pathway if necessary.1
 In my practice, one of the more common causes of posterior heel pain I frequently encounter is the posterior calcaneal exostosis with associated intratendinous calcifications. Depending on the severity and failure or success of conservative care, my treatment for this typically involves resection of the prominence with detachment of the Achilles and debridement of the calcifications followed by reattachment of the Achilles and augmentation with a flexor hallucis longus transfer. I have had cases in which insignificant amounts of prominence went unresected and symptoms persisted so I tend to be more aggressive with my resection. This leads to the need for a transfer of the flexor hallucis longus tendon.
In my practice, one of the more common causes of posterior heel pain I frequently encounter is the posterior calcaneal exostosis with associated intratendinous calcifications. Depending on the severity and failure or success of conservative care, my treatment for this typically involves resection of the prominence with detachment of the Achilles and debridement of the calcifications followed by reattachment of the Achilles and augmentation with a flexor hallucis longus transfer. I have had cases in which insignificant amounts of prominence went unresected and symptoms persisted so I tend to be more aggressive with my resection. This leads to the need for a transfer of the flexor hallucis longus tendon.
 Although Haglund’s deformity is reportedly one of the most common causes of posterior heel pain, I infrequently encounter Haglund's deformity (according to its original description) in my practice.2 In fact, many times, the condition that is often referred to as Haglund's deformity is more of a retrocalcaneal exostosis than a Haglund's deformity.3 A true Haglund's deformity is an enlargement of the posterosuperior prominence of the calcaneus.4,5
Although Haglund’s deformity is reportedly one of the most common causes of posterior heel pain, I infrequently encounter Haglund's deformity (according to its original description) in my practice.2 In fact, many times, the condition that is often referred to as Haglund's deformity is more of a retrocalcaneal exostosis than a Haglund's deformity.3 A true Haglund's deformity is an enlargement of the posterosuperior prominence of the calcaneus.4,5
 Radiographic determination of the deformity occurs by drawing parallel pitch lines over the calcaneus and observing the enlargement extending above to the superior pitch line. The lower parallel pitch line is a straight line drawn tangent to the anterior tubercle, the medial tubercle and the posterior tuberosity. Create the upper parallel pitch line by first drawing a perpendicular line from the first pitch line and superior to the posterior lip of the talar articular facet. Then draw a parallel line from the end of the perpendicular line from the tip of the talus extending posteriorly.6
Radiographic determination of the deformity occurs by drawing parallel pitch lines over the calcaneus and observing the enlargement extending above to the superior pitch line. The lower parallel pitch line is a straight line drawn tangent to the anterior tubercle, the medial tubercle and the posterior tuberosity. Create the upper parallel pitch line by first drawing a perpendicular line from the first pitch line and superior to the posterior lip of the talar articular facet. Then draw a parallel line from the end of the perpendicular line from the tip of the talus extending posteriorly.6
 Surgical treatment may involve open resection, a wedge shape osteotomy known as the Keck and Kelly, or arthroscopic resection.1,5,7
Surgical treatment may involve open resection, a wedge shape osteotomy known as the Keck and Kelly, or arthroscopic resection.1,5,7
A Closer Look At The Patient Presentation
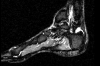
This case concerns a 43-year-old female runner who had dealt with pain in her posterior Achilles tendon and heel for five years. She had been a distance runner for over 30 years and had exhausted all forms of conservative therapy consisting of non-steroidal anti-inflammatory drugs (NSAIDs), rest, physical therapy, deep tissue massage, pressure point management and finally eight weeks in a controlled ankle motion (CAM) walker. She got a referral to me from a fellow colleague who thought she may need surgery and we began initial contact via email as she was far from my office. After reviewing radiographs and magnetic resonance imaging (MRI), I was able to establish that she most likely was suffering from a true Haglund’s deformity. Before resorting to surgical intervention, I made an attempt to work with her training patterns. We had her slow her pace down and follow her aerobic pace (her heart rate was well below lactic threshold, which for her was 137 beats per minute (BPM) to ensure she was not overdoing it. She was concerned that she would not be able to get her heart rate this high but after her first run under monitoring, she was blown away to find out how slow she had to run to keep her heart rate this low. While this may not seem important to most practitioners, running too hard too often can lead to overuse injuries, which then get stuck in the chronic phase. She adhered to this principle of training for almost six months before we elected to surgically resect the prominent Haglund’s deformity due to her continued pain with running.
After reviewing radiographs and magnetic resonance imaging (MRI), I was able to establish that she most likely was suffering from a true Haglund’s deformity. Before resorting to surgical intervention, I made an attempt to work with her training patterns. We had her slow her pace down and follow her aerobic pace (her heart rate was well below lactic threshold, which for her was 137 beats per minute (BPM) to ensure she was not overdoing it. She was concerned that she would not be able to get her heart rate this high but after her first run under monitoring, she was blown away to find out how slow she had to run to keep her heart rate this low. While this may not seem important to most practitioners, running too hard too often can lead to overuse injuries, which then get stuck in the chronic phase. She adhered to this principle of training for almost six months before we elected to surgically resect the prominent Haglund’s deformity due to her continued pain with running.
Pertinent Pointers On The Surgical Technique And Results
 For this procedure, I took a lateral approach through an incision approximately 4 cm in length. I identified and retracted the Achilles posteriorly. Deep dissection revealed the prominent superoposterior margin of the calcaneus. I excised the associated inflammatory tissue consistent with the retrocalcaneal bursa. After achieving adequate visualization with a Senn retractor, I resected the prominence with an osteotome. I then smoothed the remaining bone with a rasp and palpation revealed no further prominence. There was no further impingement of the posterior calcaneus on the Achilles tendon.
For this procedure, I took a lateral approach through an incision approximately 4 cm in length. I identified and retracted the Achilles posteriorly. Deep dissection revealed the prominent superoposterior margin of the calcaneus. I excised the associated inflammatory tissue consistent with the retrocalcaneal bursa. After achieving adequate visualization with a Senn retractor, I resected the prominence with an osteotome. I then smoothed the remaining bone with a rasp and palpation revealed no further prominence. There was no further impingement of the posterior calcaneus on the Achilles tendon.
 Postoperative care consisted of a posterior splint and non-weightbearing for two weeks followed by weightbearing in a CAM walker. Physical therapy started at three weeks post-surgery and she began spinning on a bicycle at this time as well. I also encourage my patients (especially the runners) to progress toward performing 100 calf raises a day. This doesn't have to be 100 at one time but over the course of a day. She was able to achieve this seven weeks after surgery. After nine weeks post-op, she was able to begin running. At eight months, she is able to run for 30 minutes at a time pain-free in her heel region, which she had not been able to do for over five years.
Postoperative care consisted of a posterior splint and non-weightbearing for two weeks followed by weightbearing in a CAM walker. Physical therapy started at three weeks post-surgery and she began spinning on a bicycle at this time as well. I also encourage my patients (especially the runners) to progress toward performing 100 calf raises a day. This doesn't have to be 100 at one time but over the course of a day. She was able to achieve this seven weeks after surgery. After nine weeks post-op, she was able to begin running. At eight months, she is able to run for 30 minutes at a time pain-free in her heel region, which she had not been able to do for over five years.
 I prefer to do the procedure open as opposed to arthroscopically because I feel I can access the prominence with less trauma through an incision that is slightly larger. The increased exposure allows me to remove any inflammatory bursa with ease and the recovery time is still quick. I think it is important for clinicians to look for a Haglund’s deformity with any heel pain and focus the exam on palpating deep to the anterior portion of the Achilles because even though there may be some retrocalcaneal spurring occurring, the Haglund’s deformity could be the source of the pain. The recovery time is much faster with a simple Haglund’s resection in comparison to detaching the Achilles and reattaching it to remove an exostosis.
Dr. Campitelli is an Adjunct Professor at the Kent State University College of Podiatric Medicine. He is in private practice at North East Ohio Medical Associates.
References
1. Boffeli TJ, Peterson MC. The Keck and Kelly wedge calcaneal osteotomy for Haglund's deformity: a technique for reproducible results. J Foot Ankle Surg. 2012; 51(3):398-401.
2. Johansson KJ, Sarimo JJ, Lempainen LL, Laitala-Leinonen T, Orava SY. Calcific spurs at the insertion of the Achilles tendon: a clinical and histological study. Muscles Ligaments Tendons J. 2013; 2(4):273-7.
3. Kang S, Thordarson DB, Charlton TP. Insertional Achilles tendinitis and Haglund's deformity. Foot Ankle Int. 2012; 33(6):487-91.
4. Haglund P. Beitrag zur Klinik der Achilles tendon. Zeitschr Orthop Chir 1928;49:49–58.
5. Schunck J, Jerosch J. Operative treatment of Haglund’s syndrome. Basics, indications, procedures, surgical techniques, results and problems. J Foot Ankle Surg. 2005; 11(3):123–130.
6. Banks AS, Downey MS, Martin DE, Miller SJ. (2001).Heel Surgery. In McGlamry's Comprehensive Textbook of Foot and Ankle Surgery, third edition volume 1. Lippincott Williams and Wilkins, Philadelphia, p. 443.
7. Frey C. Surgical advancements: arthroscopic alternatives to open procedures: great toe, subtalar joint, Haglund's deformity, and tendoscopy. Foot Ankle Clin. 2009; 14(2):313-39.
I prefer to do the procedure open as opposed to arthroscopically because I feel I can access the prominence with less trauma through an incision that is slightly larger. The increased exposure allows me to remove any inflammatory bursa with ease and the recovery time is still quick. I think it is important for clinicians to look for a Haglund’s deformity with any heel pain and focus the exam on palpating deep to the anterior portion of the Achilles because even though there may be some retrocalcaneal spurring occurring, the Haglund’s deformity could be the source of the pain. The recovery time is much faster with a simple Haglund’s resection in comparison to detaching the Achilles and reattaching it to remove an exostosis.
Dr. Campitelli is an Adjunct Professor at the Kent State University College of Podiatric Medicine. He is in private practice at North East Ohio Medical Associates.
References
1. Boffeli TJ, Peterson MC. The Keck and Kelly wedge calcaneal osteotomy for Haglund's deformity: a technique for reproducible results. J Foot Ankle Surg. 2012; 51(3):398-401.
2. Johansson KJ, Sarimo JJ, Lempainen LL, Laitala-Leinonen T, Orava SY. Calcific spurs at the insertion of the Achilles tendon: a clinical and histological study. Muscles Ligaments Tendons J. 2013; 2(4):273-7.
3. Kang S, Thordarson DB, Charlton TP. Insertional Achilles tendinitis and Haglund's deformity. Foot Ankle Int. 2012; 33(6):487-91.
4. Haglund P. Beitrag zur Klinik der Achilles tendon. Zeitschr Orthop Chir 1928;49:49–58.
5. Schunck J, Jerosch J. Operative treatment of Haglund’s syndrome. Basics, indications, procedures, surgical techniques, results and problems. J Foot Ankle Surg. 2005; 11(3):123–130.
6. Banks AS, Downey MS, Martin DE, Miller SJ. (2001).Heel Surgery. In McGlamry's Comprehensive Textbook of Foot and Ankle Surgery, third edition volume 1. Lippincott Williams and Wilkins, Philadelphia, p. 443.
7. Frey C. Surgical advancements: arthroscopic alternatives to open procedures: great toe, subtalar joint, Haglund's deformity, and tendoscopy. Foot Ankle Clin. 2009; 14(2):313-39.
Current Issue
April 2025
Volume 38
Issue 4

Subscribe to our E-newsletter!
Podiatry Today Newsletter
