

Why ‘Cuboid Syndrome’ Is A Misnomer
First off, I would like to say that I’m honored that Podiatry Today asked me to write a biomechanics/orthotics DPM Blog. I know some big names have been doing posts like this for years, folks like Rich Blake, DPM, and Doug Richie, DPM, among many others. So, obviously the bar has been set kind of high already and hopefully I can continue to live up to their standards of outstanding biomechanics education and insight.
Now, let’s talk about cuboid syndrome. Cuboid syndrome is one of those garbage can terms we have in medicine, like shin splints, heel pain and metatarsalgia. It is a broad diagnosis used for almost any type of non-specific lateral midfoot pain. We have written and published a lot on this “diagnosis,” but done little to specify what cuboid syndrome is about most of the time.
Most clinicians think cuboid syndrome is about a poorly positioned cuboid. They think if one mobilizes, manipulates or “whips” the cuboid back into position, it will then function normally. Many who use orthotics as a treatment element will use a cuboid pad to position the cuboid properly or elevate the apex of the lateral midfoot arch. These treatments are valid within reason but they really don’t get to the point of what the real issue is—where the tissue stress really lies in cuboid syndrome.
 Cuboid syndrome, in my opinion, is almost always about the peroneal tendons. The peroneus longus runs lateral to the ankle and midfoot, and then dives under the cuboid to insert into the first metatarsal base. The peroneus brevis runs along with the longus, but attaches to the base of the fifth metatarsal, just distal to the cuboid. Let’s not forget about the peroneus tertius. The origin of the peroneus tertius is the anterior lower one-third of the fibula and then inserts into the dorsal lateral aspect of the fifth metatarsal base. The tertius acts as an extensor of the foot but it can also evert the lateral column in late midstance.
Cuboid syndrome, in my opinion, is almost always about the peroneal tendons. The peroneus longus runs lateral to the ankle and midfoot, and then dives under the cuboid to insert into the first metatarsal base. The peroneus brevis runs along with the longus, but attaches to the base of the fifth metatarsal, just distal to the cuboid. Let’s not forget about the peroneus tertius. The origin of the peroneus tertius is the anterior lower one-third of the fibula and then inserts into the dorsal lateral aspect of the fifth metatarsal base. The tertius acts as an extensor of the foot but it can also evert the lateral column in late midstance.
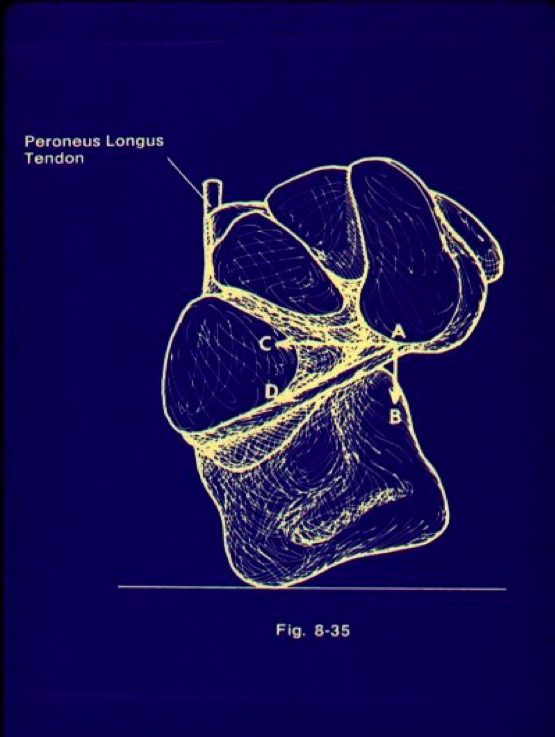
All these tendons pass lateral to, under or over the cuboid. In the case of the peroneus longus, the anatomical position of the cuboid can affect its action. Root’s text on biomechanics has a great picture (left) on how the position of the cuboid and midfoot can affect the pull of the peroneus longus tendon, and thereby affect the stability of its action in keeping the first metatarsal plantarflexed.1 When the cuboid everts, the width of the midfoot increases and this can stop any eccentric energy storage and action of the tendon, which then can lead to hypermobility of the first ray, or a better term, decreased stiffness of the first ray, according to Kirby.2 I’ll be discussing some of these different terms more in-depth as this blog continues. If the cuboid is properly positioned and inverted (see right photo), the width of the midfoot is usually shorter and this can allow the peroneus longus to work better in most instances.
 The peroneus tertius is interesting because it tends to become inflamed when the peroneus longus, in particular, is no longer working effectively in late midstance. I often find that when a patient has an unstable medial column, the peroneus tertius will attempt to help with late midstance eversion of the forefoot, also known as supination in Root terms. If you trace the action and muscle test the tertius, you will often find the pain to be over this area of the tendon from its insertion and overlying the cuboid.
The peroneus tertius is interesting because it tends to become inflamed when the peroneus longus, in particular, is no longer working effectively in late midstance. I often find that when a patient has an unstable medial column, the peroneus tertius will attempt to help with late midstance eversion of the forefoot, also known as supination in Root terms. If you trace the action and muscle test the tertius, you will often find the pain to be over this area of the tendon from its insertion and overlying the cuboid.
I also find many patients have decreased stiffness of their lateral column and this can affect their ability to drive the lateral forces medially for proper propulsion of the foot.
Let’s discuss treatment options briefly. As I mentioned above, the use of manipulation techniques and pads can assist with this issue. I’m all for manipulations as I use them daily in my practice. I think you must start at the fibular head with Dananberg’s technique, work down to the ankle joint and then finally manipulate the plantar midfoot and third cuneiform/cuboid articulation.3 I have found these techniques can help to position the foot for a better cast for orthotics. Plus, when one combines this with an orthotic that has proper prescriptive elements, Dananberg’s technique maintains the position without a regular need for repeated manipulations.
To help the lateral column evert in late midstance and maximally pronate or dorsiflex a less stiff or hypermobile lateral column, I will use a lateral forefoot wedge of varying degrees. This will assist the foot as it supinates in late midstance to propulsion, driving it toward the medial column. A cuboid pad may do the same thing but I tend to put the valgus wedge under the fourth and fifth metatarsals, and often extend it out to the fourth and fifth metatarsophalangeal joints (MPJs). I will often use a first ray cutout, digital wedging and heel lifts for ankle equinus in my prescription as well. I will touch on these last prescriptive elements in future blog posts.
Using manipulation techniques and valgus wedging along with other prescriptive elements can help with the peroneal function in what is often termed “cuboid syndrome.” Try it and I think you will be pleasantly surprised with the improved results for your patients.
References
1. Root ML, Orien WP, Weed JH, RJ Hughes. Biomechanical Examination of the Foot, Volume 1. Clinical Biomechanics Corporation, Los Angeles, 1971, p. 24.
2. Kirby KA, Roukis TS. Precise naming aids dorsiflexion stiffness diagnosis. Biomechanics. 2005;12 (7): 55-62.
3. Dananberg HJ, Shearstone J, Guillano M. Manipulation method for the treatment of ankle equinus. J Am Podiatr Med Assoc. 2000; 90(8):385-389.


