

What Nerve Provides The Sensation Of Plantar Heel Pain?
There has always been misunderstanding about the nomenclature, anatomy and role of certain nerves in the propagation of plantar heel pain.
For example, consider this simple quiz:
Question: What nerve innervates the periosteum and plantar fascia attachment at the medial calcaneal tubercle?
A. Medial calcaneal nerve
B. First branch of the lateral plantar nerve
C. Nerve to the abductor digiti quinti
D. Baxter’s nerve
Answer: B, C and D because they are all the same nerve!
The critical issue is that the medial calcaneal nerve is often implicated as a cause of heel pain but it is actually a sensory nerve, which only innervates the skin and fat pad under the calcaneus. The medial calcaneal nerve does not pass deep enough to innervate the origin of the plantar fascia. However, degeneration of the enthesis of the plantar fascia is implicated as the most common cause of plantar heel pain.1-3
Why is it important to know the anatomy and innervation of the nerves around the calcaneus when treating plantar heel pain?
• Careful physical examination along with certain diagnostic studies can detect if plantar heel pain is neurogenic in origin.
• Accurate placement of injection therapy to a specific nerve can be helpful as both a diagnostic and therapeutic modality in treating plantar heel pain.
• Surgical decompression, neurolysis and/or radiofrequency ablation of a specific nerve may be options in certain cases of chronic plantar heel pain. These modalities all require detailed knowledge of the relevant anatomy.
Reviewing The Neuroanatomy Relevant To Heel Pain
 Many authors name the first branch of the lateral plantar nerve as a potential cause of plantar heel pain.4 This nerve, also known as the nerve to the abductor digiti quinti, originates from the lateral plantar nerve at the level of the bifurcation of the tibial nerve into the medial and lateral plantar nerves.5 It is also known as the inferior calcaneal nerve (ICN). (See “A Guide To Nerve Anatomy Of The Tarsal Tunnel And Medial Calcaneus” at the right.)
Many authors name the first branch of the lateral plantar nerve as a potential cause of plantar heel pain.4 This nerve, also known as the nerve to the abductor digiti quinti, originates from the lateral plantar nerve at the level of the bifurcation of the tibial nerve into the medial and lateral plantar nerves.5 It is also known as the inferior calcaneal nerve (ICN). (See “A Guide To Nerve Anatomy Of The Tarsal Tunnel And Medial Calcaneus” at the right.)
The first branch of the lateral plantar nerve passes through a discreet corridor bordered medially by the abductor hallucis muscle and laterally by the medial head of the quadratus plantae muscle. At the lower border of the abductor hallucis, the nerve makes an abrupt lateral turn, passing above the thick fascia of the medial intermuscular septum. The inferior calcaneal nerve takes its lateral turn across the bony inferior medial ridge of the calcaneus. Then it crosses beneath the quadratus plantae obliquely, giving branches to the periosteum of the medial tuberosity of the calcaneus, the long plantar ligament, the lateral head of the quadratus plantae and the flexor digitorum brevis. It finally divides into two branches that insert into the abductor digiti quinti.5
Roegholt was the first to propose a mechanism whereby the first branch of the lateral plantar nerve could become entrapped and cause plantar heel pain.6 He re-named this nerve the inferior calcaneal nerve and speculated that its position is vulnerable to entrapment by a calcaneal spur. Tanz evaluated the first branch of the lateral plantar nerve and also observed that there was potential for entrapment by a calcaneal spur, inflammation or venous engorgement.7
Arenson and colleagues studied 30 cadaver feet and confirmed previous reports showing the course of the inferior calcaneal nerve and its insertion into the proximal attachment of the plantar fascia to the periosteum of the calcaneus.8 Przylucki and Jones dissected the inferior calcaneal nerve in four surgical patients with heel pain and performed histologic examination of the specimens, documenting changes consistent with entrapment neuropathy.9 They proposed a mechanism by which there could be entrapment of the inferior calcaneal nerve at the medial edge of the calcaneus.
Baxter and Thigpen described neurolysis of the “mixed nerve supplying the abductor digiti quinti muscle” in 26 patients.10 They proposed the site of entrapment to be at two possible locations: the fascia of the abductor hallucis muscle and/or the medial edge of the calcaneus. After publication of this article, entrapment of the first branch of the lateral plantar nerve became known as “Baxter’s neuropathy” despite the fact that the condition had been described by at least three other authors in previous publications.6-8
It is appropriate that Saraffian also adopted the name inferior calcaneal nerve to describe the first branch of the lateral plantar nerve.5 The term “first branch of the lateral plantar nerve” is a misnomer because sometimes this nerve branches off the tibial nerve. The term “nerve to abductor digiti quinti” is misleading because it neglects to describe the important innervation this nerve provides to the flexor digitorum brevis and quadratus plantae muscles. The term inferior calcaneal nerve is appropriate in describing its unique location and its potential role in plantar heel pain.
 The medial calcaneal nerve is a pure sensory nerve, which has no innervation to the plantar fascia or periosteum of the calcaneus.13 This nerve originates from the posterior tibial nerve, usually posterior and proximal to the origin of the lateral calcaneal nerve.5 The medial calcaneal nerve divides into three branches at the level of the tarsal tunnel. The posterior branch innervates the skin covering the medial aspect of the Achilles tendon as well as the medial and posterior portion of the heel. (See “Subcalcaneal Fat Pad Innervation Of The Medial Calcaneal Nerve” at the right.)
The medial calcaneal nerve is a pure sensory nerve, which has no innervation to the plantar fascia or periosteum of the calcaneus.13 This nerve originates from the posterior tibial nerve, usually posterior and proximal to the origin of the lateral calcaneal nerve.5 The medial calcaneal nerve divides into three branches at the level of the tarsal tunnel. The posterior branch innervates the skin covering the medial aspect of the Achilles tendon as well as the medial and posterior portion of the heel. (See “Subcalcaneal Fat Pad Innervation Of The Medial Calcaneal Nerve” at the right.)
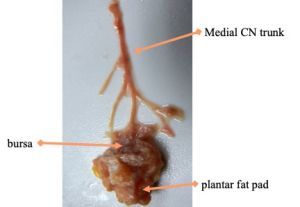 The middle and anterior branches course through the fat pad of the heel, innervating the skin on the plantar heel and proximal arch. There is no connection of the medial calcaneal nerve to the deep fascia, the periosteum of the calcaneus or the plantar aponeurosis. However, the medial calcaneal nerve does innervate the fat pad and bursa beneath the calcaneus so it could be involved with a variation of plantar heel pain not caused by the plantar fasciitis.5,13 (See “Isolated Dissection Of The Medial Calcaneal Nerve” at the right.)
The middle and anterior branches course through the fat pad of the heel, innervating the skin on the plantar heel and proximal arch. There is no connection of the medial calcaneal nerve to the deep fascia, the periosteum of the calcaneus or the plantar aponeurosis. However, the medial calcaneal nerve does innervate the fat pad and bursa beneath the calcaneus so it could be involved with a variation of plantar heel pain not caused by the plantar fasciitis.5,13 (See “Isolated Dissection Of The Medial Calcaneal Nerve” at the right.)
Understanding The Ramifications Of Nerve Entrapment In Plantar Heel Pain
Entrapment of the medial calcaneal nerve can be a cause of plantar heel pain.14 This nerve is superficial and vulnerable to compression against the plantar and medial edges of the calcaneus. The most common symptom besides superficial pain is numbness in the integument medial and plantar to the calcaneus. However, diagnosing a specific entrapment of the medial calcaneal nerve is difficult. Interestingly, there is evidence that patients suffering from plantar fasciitis show abnormal sensory nerve potentials of the medial calcaneal nerve with nerve conduction studies.15 It is unknown if this conduction delay is a cause or an effect of plantar heel pain since edema from plantar fasciitis can secondarily cause compression of the superficial medical calcaneal nerve.
Entrapment of the inferior calcaneal nerve can be a secondary result of longstanding plantar fasciopathy in which degenerative changes cause hypertrophy of the plantar fascia at or near the insertion to the calcaneus.3 The thickened plantar fascia will limit the space in the narrow tunnel where the inferior calcaneal nerve passes beneath the calcaneus, leading to entrapment. When the nerve becomes entrapped, compromise of motor function to the abductor digiti quinti as well as the flexor digitorum brevis will occur. This may show clinically as an inability for the patient to plantarflex his or her toes, or abduct the fifth digit. Even though these are subtle findings, comparison to the unaffected contralateral foot can demonstrate the weakness.
In 2012, I participated in a prospective, randomized double-blinded study investigating the efficacy of radiofrequency ablation of the inferior calcaneal nerve to treat chronic heel pain.16 Pulsed radiofrequency ablation can safely target the sensory fibers of the mixed inferior calcaneal nerve while sparing the motor fibers. Our study showed that 90 percent of patients with chronic heel pain can obtain relief with radiofrequency nerve ablation, regardless of whether the pain is due to plantar fasciitis, entrapment of the inferior calcaneal nerve or both.16 The pain of plantar fasciitis can be addressed with ablation of the ICN and does not require that the nerve itself is entrapped. Other studies have confirmed our positive results treating chronic plantar heel pain with radiofrequency nerve ablation of the inferior calcaneal nerve.17-20
There are several studies report targeting the medial calcaneal nerve rather than the inferior calcaneal nerve with radiofrequency ablation to treat chronic heel pain.21,22 In another study, Arsan and colleagues performed ablation on both the medial calcaneal nerve and the inferior calcaneal nerve.23 When study authors chose the medial calcaneal nerve as the site for ablation, patient symptoms were clearly isolated to the integument and fat pad at the plantar and medial margins of the calcaneus. However, in most cases of plantar heel pain, the symptoms are located at the medial calcaneal tubercle where the enthesis of the plantar fascia attaches. The inferior calcaneal nerve innervates this area, not the medial calcaneal nerve. One can expect ablation of the inferior calcaneal nerve at this location to reduce plantar heel pain whether the condition is due to plantar fasciopathy or nerve entrapment.
I am not suggesting that radiofrequency nerve ablation should be the first choice of treatment of patients with plantar heel pain. However, in chronic recalcitrant cases, this modality warrants consideration as evidence suggests it is a safe and effective option.16-19 There are certainly other options for treatment of chronic plantar heel pain. Either way, when a patient with chronic plantar heel pain is not responding to treatment, further diagnostic workup is necessary. A thorough knowledge of the anatomy and function of the nerves in the medial and plantar aspects of the calcaneus is essential. One must consider the health of the plantar fascia and the calcaneus as well as the possibility of nerve entrapment before implementing further treatment options.
Dr. Richie is an Adjunct Associate Professor within the Department of Applied Biomechanics at the California School of Podiatric Medicine at Samuel Merritt University in Oakland, Calif. He is a Fellow and Past President of the American Academy of Podiatric Sports Medicine. Dr. Richie is a Fellow of the American College of Foot and Ankle Surgeons and the American Academy of Podiatric Sports Medicine.
References
- Michelson JD. Heel pain: when is it plantar fasciitis?J Musculoskelet Med.1995;12:22-26.
- Rome K. Anthropometric and biomechanical risk factors in the development of plantar heel pain–a review of the literature. Phys Ther Rev. 1997;2(3):123-134.
- Beeson P. Plantar fasciopathy: revisiting the risk factors. Foot Ankle Surg. 2014;20(3):160-165.
- Rondhuis JJ, Huson A. The first branch of the lateral plantar nerve and heel pain. Acta Morphol Neerl Scand. 1986;24:269.
- Sarrafian SK, Kelikian AS. Nerves. In: Sarrafian’s Anatomy of the Foot and Ankle: Descriptive, Topographic, Functional. 3rd ed. Philadelphia: Wolters Kluwer;2011:381-428.
- Roegholt MN. Een nervus calcaneus inferior als overbrenger van de pijn bij calcaneodynie of calcanensspoor en de daaruit volgende therapie. Ned Tijdschr v Geneeskd. 1940; 84:1898.
- Tanz SS. Heel pain. Clin Orthop. 1963;28:169.
- Arenson DJ, Cosentina GL, Suran SM. The inferior calcaneal nerve, an anatomical study. J Am Podiatr Assoc. 1980;70:552
- Przylucki H, Jones CL. Entrapment neuropathy of muscle branch of lateral plantar nerve. J Am Podiatr Assoc. 1981:71:119.
- Baxter DE, Thigpen CM. Heel pain - operative results. Foot Ankle.1984;5(1):16.
- Moroni S, Zwierzina M, Starke V, Moriggl B, Montesi F, Konschake M. Clinical-anatomic mapping of the tarsal tunnel with regard to Baxter’s neuropathy in recalcitrant heel pain syndrome: part 1. Surg Radiol Anat. 2018;41(1):29-41.
- Hornick B, Amabile AH. Baxter’s nerve impingement and other neuropathies of the foot: implications for physical therapy. FASEB J. 2017;4:31.
- Louisia S, Masquelet AC.The medial and inferior calcaneal nerves: an anatomic study. Surg Radiol Anat.1999;21:169–173.
- Diers DJ. Medial calcaneal nerve entrapment as a cause for chronic heel pain. Physiother Theory Prac. 2008;24(4):291-298.
- Chang C-W, Wang Y-C, Hou W-H, Xin-Xian L, Chang K-F. Medial calcaneal neuropathy is associated with plantar fasciitis. Clin Neurophysiol. 2007;118(1):119–123.
- Landsman AS, Catanese DJ, Wiener SN, Richie DH, Hanft JR. A prospective, randomized, double-blinded study with crossover to determine the efficacy of radio-frequency nerve ablation for the treatment of heel pain. J Am Podiatr Med Assoc. 2013;103:8–15.
- Liden B, Simmons M, Landsman A. A retrospective analysis of 22 patients treated with percutaneous radiofrequency nerve ablation for prolonged moderate to severe heel pain associated with plantar fasciitis. J Foot Ankle Surg. 2009;48:642–647.
- Erken HY, Ayanoglu S, Akmaz I, Erler K, Kiral A. Prospective study of percutaneous radiofrequency nerve ablation for chronic plantar fasciitis. Foot Ankle Int. 2013;35(2):95-103.
- Cozzarelli J, Sollitto RJ, Thapar J, Caponigro J. A 12-year long-term retrospective analysis of the use of radiofrequency nerve ablation for the treatment of neurogenic heel pain. Foot Ankle Spec. 2010;3(6):338-346.
- Turhan Y, Arican M. Comparison of three different treatment modalities in the treatment of chronic plantar fasciitis: corticosteroid injection, extracorporeal shock wave therapy and radiofrequency nerve ablation. Duzce Med J. 2019;21(2):118-122.
- Cione J, Cozzarelli J, Mullin C. A retrospective study of radiofrequency thermal lesioning for the treatment of neuritis of the medial calcaneal nerve and its terminal branches in chronic heel pain. J Foot Ankle Surg. 2009;48:142–147.
- Counsel PD, Davenport MB, Brown A, et al. Ultrasound-guided radiofrequency denervation of the medial calcaneal nerve. Clin J Sport Med. 2016;26(6):465.
- Arslan A, Koca TT, Utkan A, Sevimli R, Akel I. Treatment of chronic plantar heel pain with radiofrequency neural ablation of the first branch of the lateral plantar nerve and medial calcaneal nerve branches. J Foot Ankle Surg. 2016;55(4):767-771.


