

ADVERTISEMENT
Peroneal Function And Fibular Translation: Assessing Their Impact On The First Ray And Ankle Range Of Motion
 In my first DPM Blog post, I talked about the peroneals and the misnomer of “cuboid syndrome.”1 I want to continue to discuss the peroneals again in this post, regarding their importance to the functional stiffness of the first ray and their effect on ankle joint range of motion.
In my first DPM Blog post, I talked about the peroneals and the misnomer of “cuboid syndrome.”1 I want to continue to discuss the peroneals again in this post, regarding their importance to the functional stiffness of the first ray and their effect on ankle joint range of motion.
 The peroneus longus originates along the lateral aspect of the fibula and then slides behind and under the lateral malleolus. The peroneus longus then slides under the cuboid to insert at the base of the first metatarsal and medial midfoot (see photo 1). The anatomy of this tendon is of great importance to the first ray’s ability to remain stable against the ground as the foot pivots over and around the first metatarsophalangeal joint (MPJ) in gait (see photo 2).
The peroneus longus originates along the lateral aspect of the fibula and then slides behind and under the lateral malleolus. The peroneus longus then slides under the cuboid to insert at the base of the first metatarsal and medial midfoot (see photo 1). The anatomy of this tendon is of great importance to the first ray’s ability to remain stable against the ground as the foot pivots over and around the first metatarsophalangeal joint (MPJ) in gait (see photo 2).
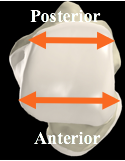 I cannot overstress the importance of the attachment of the peroneals to the fibula. The fibula is part of the ankle joint mortise along with the tibia and the superior articular surface of the talus. The superior talar articulation is broader at the anterior aspect of the talus and narrower at the posterior aspect of the talus (see photo 3). As Howard Dananberg, DPM, explained to me a long time ago, for the talus to dorsiflex within the ankle mortise, because the anterior aspect of the talar articulation is wider than the posterior aspect, something must move out of the way to allow for this dorsiflexion movement.
I cannot overstress the importance of the attachment of the peroneals to the fibula. The fibula is part of the ankle joint mortise along with the tibia and the superior articular surface of the talus. The superior talar articulation is broader at the anterior aspect of the talus and narrower at the posterior aspect of the talus (see photo 3). As Howard Dananberg, DPM, explained to me a long time ago, for the talus to dorsiflex within the ankle mortise, because the anterior aspect of the talar articulation is wider than the posterior aspect, something must move out of the way to allow for this dorsiflexion movement.
 The fibula is what moves in the ankle joint to allow for talar dorsiflexion (see photo 4). The fibula translates superiorly, laterally and posteriorly for the talus to dorsiflex appropriately. The further importance of the superior translation of the fibula is that the peroneals are attached to the lateral aspect of the fibula. So, as the fibula translates superiorly, it pulls the origin of the peroneals along with it. The effect of this motion, along with the timing of this event, which is mid- to late midstance, allows for the peroneus longus tendon to tighten its pull on the base of the first metatarsal and evert the cuboid. This also leads to a more stable midfoot and medial column while stabilizing the first metatarsal head against the ground so the foot can roll over the first MPJ into propulsion.
The fibula is what moves in the ankle joint to allow for talar dorsiflexion (see photo 4). The fibula translates superiorly, laterally and posteriorly for the talus to dorsiflex appropriately. The further importance of the superior translation of the fibula is that the peroneals are attached to the lateral aspect of the fibula. So, as the fibula translates superiorly, it pulls the origin of the peroneals along with it. The effect of this motion, along with the timing of this event, which is mid- to late midstance, allows for the peroneus longus tendon to tighten its pull on the base of the first metatarsal and evert the cuboid. This also leads to a more stable midfoot and medial column while stabilizing the first metatarsal head against the ground so the foot can roll over the first MPJ into propulsion.
If any of these things do not occur, then the first MPJ will dorsiflex instead of staying stable against the ground. This can lead to both a functional and structural hallux limitus over time. Failure of the fibula to translate superiorly and in a timely manner can lead to ankle joint equinus as well.
There are issues that can affect both translational events at the ankle and the first MPJ. One issue is the ankle sprain, which can cause loosening of the anterior talofibular ligament and allow the talus to move anterior in the talar mortise. This can keep the fibula from translating superiorly effectively because the narrower posterior aspect of the talar articulation is in the central portion of the ankle mortise. Over time, the capsule and ligaments of the ankle can fibrose and create a functional equinus that will continue to be an issue.
At the first ray, if the first metatarsal is long and the medial column has no inherent stiffness, then the first metatarsal will dorsiflex regardless of the pull of the peroneus longus. This may possibly have a retrograde effect on ankle dorsiflexion as well but I am not completely sure about this. If you consider that one needs a stable midfoot and medial column to tighten the peroneus longus as the fibula translates, then this could make sense from a chicken/egg standpoint.
Regardless, fibular translation and peroneal function are key in stabilizing the first metatarsal and providing proper function of the first MPJ. If one of these actions fails to work in a timely fashion, functional hallux limitus will result along with other potential gait issues.
Thanks for reading. I’d love to get your feedback. Until next month, cheers.
Reference
1. Williams B. Why ‘cuboid syndrome’ is a misnomer. Podiatry Today DPM Blog. Available at https://www.podiatrytoday.com/blogged/why-%E2%80%98cuboid-syndrome%E2%80%99-misnomer . Published April 6, 2018.


