

Study Examines Seasonal Variance Between PAD and Infection-Related Transmetatarsal Amputations
Lower extremity amputations can result from complications associated with peripheral arterial disease (PAD), trauma, and most commonly diabetes.1,2 An estimated 1.6 million people in the United States are living with a lower extremity amputation at some level; however, this number is expected to double and reach 3.6 million by 2050.1,2 Even though the diabetic population is increasing, diabetes-related amputations are declining due to early intervention and preventative measures.1 Previous studies have demonstrated the negative physical and mental health associations with amputations.3,4 The combined 5-year mortality for minor and major amputations in the literature ranges from 53% to 100%.3
In 1997, Armstrong and colleagues published a study that determined the most common season for a diabetes-related amputation is in the spring, and for patients without diabetes, winter.5 They reported that cold weather may be a protective measure for at-risk limbs as patients with diabetes are likely less active, thus decreasing the chances of ulceration. Chung and colleagues reported that the most common months to have a diabetic amputation were in March, July, and November.6 However, there are no studies to our knowledge that have analyzed the seasonal variance of amputations based on the reason for the amputation.
In the present study, we separated patients into 3 groups: those with PAD, infection, or infection in the setting of PAD such as wet gangrene. Our purpose is to compare the seasons and demographics among the 3 groups to assist providers in patient education and amputation prevention. We hypothesize that amputations secondary to infection will increase in the spring, whereas amputations resulting from PAD will increase during winter.
A Closer Look at the Study
After obtaining Institutional Review Board approval, we conducted a retrospective chart review to identify all patients who underwent a transmetatarsal amputation (TMA) between January 1, 2020, and December 31, 2021 at a single academic hospital. Inclusion criteria encompassed all patients over ages 18 and above who underwent a transmetatarsal amputation for infection, peripheral arterial disease, or infection in the setting of PAD. Exclusion criteria included patients who underwent a transmetatarsal amputation for trauma or deformity. All patients were divided into 3 categories: infection, peripheral arterial disease, or infection in the setting of PAD. Consult note diagnoses, laboratory values, and operative notes classified patients into these 3 categories. Laboratory values analyzed included white blood cell count, C-reactive protein (CRP), and erythrocyte sedimentation rate (ESR). Patients with ankle brachial index (ABI) values within 2 months of surgery were included and analyzed. An ABI result was defined as abnormal if the value was < 0.9.
We performed summary statistics including mean and standard deviation for continuous variables such as age and laboratory values for both groups. We compared categorical variables using a Fischer’s test and used the Kruskal-Wallist test to compare continuous variables. P-values < .05 were assumed to be statistically significant.
What the Study Results Revealed
After applying inclusion and exclusion criteria, the study included 86 patients with 87 operative extremities. The average age for patients who underwent TMA was 60.5 +/- 11.1. There was no statistically significant difference in age, gender, or laterality between seasons as seen in Table 1, Table 2, and Table 3 respectively.
Season variance of surgery. The study classified patients by season based on the date of surgery. Fall was defined as starting September 1, winter starting December 1, spring starting March 1, and summer starting June 1. There was no statistically significant difference in the season that the transmetatarsal amputations occurred among the 3 categories: infection, PAD, and infection in the setting of PAD (P = .96) (Table 4).
Comorbidities. We documented comorbidities for patients at the time of surgery as seen in Table 5. There was no statistically significant difference between the prevalence of diabetes, chronic kidney disease, coronary arterial disease, and peripheral arterial disease. However, there was a statistically significant difference in hypertension between the seasons (P = .029).
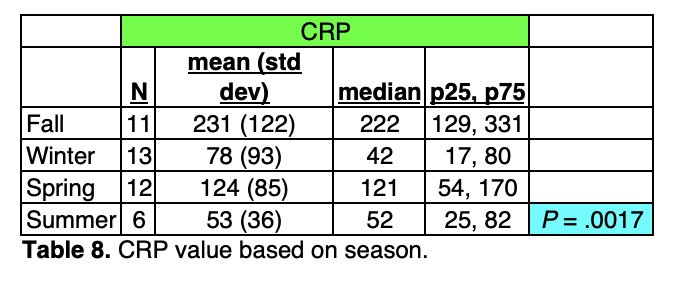
Laboratory values. We recorded the preoperative white blood cells (WBC), CRP, and ESR for patients who underwent a TMA. When comparing the laboratory values based on the season of surgery, WBC (P = .13) and ESR (P = .32) showed no statistically significant difference, as seen in Table 6 and Table 7. However, CRP was found to have statistically significant differences amongst the seasons (P = .0017). Fall reported the highest CRP values with a mean of 231 (Table 8). Significant comparisons between seasons for CRP included fall to summer, fall to spring, and fall to winter as seen in Table 9.
Ankle brachial index. There were 57 patients who had an ABI within 2 months of surgery. An ABI was abnormal if the value was <0.9. As shown in Table 10, there was no statistically significant difference between the abnormal and normal ABI groups based on the season (P = .54).
Insights on Seasonal Variance in Amputation
This is the first study to our knowledge that breaks down the causes of amputations between PAD and infection, and analyzes the relationship between the seasons. The present study found no relationship between the season of surgery and the cause of the surgery (P = .96); therefore, we fail to reject our null hypothesis.
The present study did not find a difference in the prevalence of diabetes in patients who underwent a TMA (P = .42). This is different from what has previously been reported. Armstrong and colleagues published in 1997 that diabetes-related amputations are most common in the spring.5,7 Leung and colleagues found in Hong Kong, warm weather aggravates the severity of the infection and precipitates amputation.8 Chung and colleagues found in South Korea, diabetic foot amputations occurred most in March, July, and November.6
Altin and colleagues analyzed critical limb ischemia hospitalizations and amputations.9 The peak admission season was in spring. They found a seasonal variability in critical limb ischemia admissions and mortality but no significant seasonal rates for minor or major amputation rates. This is similar to our present study, which investigated ABIs and the diagnosis of PAD in patients with a TMA according to season and found no statistically significant differences, P = .54 and P = .57, respectively.
One limitation of the present study is that it only analyzed transmetatarsal amputations. We chose this procedure as it is a common surgery for PAD and infection-related amputations. However, our findings may be limited to only this procedure. Therefore, we recommend future studies look at the seasonal variance of other minor and major amputations.
Another limitation of the study is that all amputations were performed in the state of North Carolina; therefore, regional climate differences may play a factor in our results. The average highs and low temperatures of the seasons in North Carolina are as follows: winter (51ºF, 32ºF), spring (70ºF, 48ºF), summer (86.6ºF, 46.6ºF), and fall (71ºF, 50.3ºF), respectively.10 It is certainly possible that varying climates may play a contributing role in the pathology necessitating a transmetatarsal amputation. Further studies in different regions of the country may address this question.
In order to classify patients into the 3 categories (PAD, infection, and PAD in the setting of infection), the authors looked at the operative, preoperative, and postoperative diagnoses and findings, laboratory values, vital signs, and clinical exam findings. If there was any discrepancy between patient classification among the authors, we consulted the senior surgeon. However, we recognize there are multiple confounding factors that may contribute to a patient needing an amputation and dividing patients into 3 categories may be oversimplification. We attempted to reduce this bias by analyzing comorbidities and laboratory values as well.
Our institution uses non-cardiac CRP to evaluate patients on presentation with possible infection or inflammatory processes. This study found statistically significant elevated non-cardiac CRP levels in the fall when compared to the other seasons. No studies to our knowledge have variances in non-cardiac CRP based on seasons. A study by Sung and colleagues investigated cardiac CRP and found a highly significant seasonal variation in CRP levels with higher values in the winter and spring than in summer.11 We recommend future studies analyze the seasonal variance of non-cardiac CRP.
In Conclusion
Our findings do not support our hypothesis that seasonal variance plays a role in the pathology necessitating transmetatarsal amputations. We found no significant difference between patients who underwent a transmetatarsal amputation for infection, peripheral arterial disease, or infection in the setting of peripheral arterial disease and the season in which the amputation occurred. Regardless of the presence or absence of seasonal correlation, the mission of podiatrists and other limb preservation professionals remains critical.
Jennifer Kipp, DPM, is a third year resident in the Department of Orthopaedic Surgery and Rehabilitation at Wake Forest University School of Medicine.
Bryanna D. Vesely, DPM, MPH, practices at Orthopaedic and Spine Center in Newport News, VA.
Madeline Fram, BA, is a fourth year medical student at Wake Forest University School of Medicine.
Gregory Russell, MS, is a Senior Biostatistician at Wake Forest University School of Medicine.
Ashleigh W. Medda, DPM, is an Assistant Professor in the Department of Orthopaedic Surgery and Rehabilitation at Wake Forest University School of Medicine.
References
1. Varma P, Stineman MG, Dillingham TR. Epidemiology of limb loss. Phys Med Rehabil Clin N Am. 2014 Feb;25(1):1-8. doi: 10.1016/j.pmr.2013.09.001. PMID: 24287235; PMCID: PMC4533906.
2. Ziegler-Graham K, MacKenzie EJ, Ephraim PL, Travison TG, Brookmeyer R. Estimating the prevalence of limb loss in the United States: 2005 to 2050. Arch Phys Med Rehabil. 2008;89(3):422-429. doi:10.1016/j.apmr.2007.11.005
3. Thorud JC, Plemmons B, Buckley CJ, Shibuya N, Jupiter DC. Mortality after nontraumatic major amputation among patients with diabetes and peripheral vascular disease: a systematic review. J Foot Ankle Surg. 2016 May-Jun;55(3):591-9. doi: 10.1053/j.jfas.2016.01.012. Epub 2016 Feb 19. PMID: 26898398.
4. Wukich DK, Raspovic KM, Suder NC. Patients with diabetic foot disease fear major lower-extremity amputation more than death. Foot Ankle Spec. 2018;11(1):17–21.
5. Armstrong DG, Lavery LA, van Houtum WH, Harkless LB. Seasonal variations in lower extremity amputation. J Foot Ankle Surg. 1997 Mar-Apr;36(2):146-50. doi: 10.1016/s1067-2516(97)80062-2. PMID: 9127220.
6. Chung HJ, Chun DI, Kang EM, et al. Trend and seasonality of diabetic foot amputation in South Korea: a population-based nationwide study. Int J Environ Res Public Health. 2022 Mar 30;19(7):4111. doi: 10.3390/ijerph19074111. PMID: 35409793; PMCID: PMC8998930.
7. Armstrong DG, Swerdlow MA, Armstrong AA, Conte MS, Padula WV, Bus SA. Five year mortality and direct costs of care for people with diabetic foot complications are comparable to cancer. J Foot Ankle Res. 2020 Mar 24;13(1):16. doi: 10.1186/s13047-020-00383-2. PMID: 32209136; PMCID: PMC7092527.
8. Leung HB, Ho YC, Wong WC, Guerin J. Seasonal variations in non-traumatic major lower limb amputation in Hong Kong Chinese diabetic patients. Hong Kong Med J. 2007 Oct;13(5):379-81. PMID: 17914144.
9. Altin SE, Kim YG, Aronow HD, et al. Seasonal variation in U.S. hospitalizations for chronic limb-threatening ischemia. Catheter Cardiovasc Interv. 2020 Dec;96(7):1473-1480. doi: 10.1002/ccd.29261. Epub 2020 Sep 9. PMID: 32902126.
10. Weather Averages, North Carolina. www.usclimatedata.com. Updated 2023. Accessed April 26, 2023. https://www.usclimatedata.com/climate/andrews/north-carolina/united-states/usnc0012.
11. Sung KC. Seasonal variation of C-reactive protein in apparently healthy Koreans. Int J Cardiol. 2006;107(3):338-342. doi: 10.1016/j.ijcard.2005.03.045.



{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}