

A Guide To First MPJ Arthrodesis For Active Patients
Surgical recommendations are sparse when evaluating treatment options for the athletic population diagnosed with hallux limitus, hallux rigidus or first metatarsophalangeal (MPJ) osteoarthritis. However, we have found success in treating athletes with first MPJ arthrodesis, and helping them to achieve pain relief and a return to activities. Several surgeons have found similar success as evidenced by a review of the literature on this subject. In 1996, Bouche, et. al., advocated first MPJ arthrodesis in active patients, reporting that it could “relieve pain and allow patients to perform some athletic function (including running).”1 They performed first MPJ arthrodesis for five individuals who ranged from 42 to 57 years old and each patient returned to his or her respective preoperative weightbearing activity. The daily activities of these patients included walking, exercise, race walking, power walking and running. While there is still controversy on whether one should perform first MPJ arthrodesis in the active population, Bouche says the first MPJ arthrodesis is the preferred joint destructive procedure in active patients and is a “definitive, predictable and viable option.”1 In 2005, Brodsky, et. al., presented results of a retrospective study and indicated that “patients with a first MPJ fusion function extremely well and most athletic patients continue participating in sports with the advantage of greatly diminished discomfort.”2 Surgeons performed a first MPJ arthrodesis on 53 patients (60 feet), who ranged between 21 to 79 years old. These patients engaged in weightbearing activities ranging from activities of daily living to recreational sports and exercise.2 The researchers performed postoperative functional testing on 45 patients. Of those 45 patients, 64 percent could stand on their tiptoes, 94 percent could kneel, 87 percent could squat and 98 percent could pick up a small object from the floor.2 The following are the results of patient answers to a functional questionnaire.2 • 100 percent could ascend stairs • 96 percent could descend stairs • 100 percent could walk less than one block • 96 percent could walk one to six blocks • 90 percent could walk over six blocks • 75 percent returned to jogging • 80 percent returned to golfing • 92 percent returned to hiking • 75 percent returned to tennis • 98 percent returned to work • 45 percent had no shoe limitations • 47 percent required comfort shoes • 8 percent required prescription insoles Brodsky, et. al., described arthrodesis of the first MPJ as “a successful surgical procedure that provides relief of pain, correction of deformity and allows a high level of function in everyday life and in recreational activities.”2
Hallux Rigidus: Essential Staging Insights
When staging hallux rigidus, we prefer to use the Modified Regnauld Classification as presented by Vanore, et al., and adapted by the American College of Foot and Ankle Surgeons.3-6 Here are the stages of this classification. Stage I: functional hallux limitus. This includes hallux equinus/flexus, plantar subluxation of the proximal phalanx and metatarsus primus elevatus. There is also joint dorsiflexion that may be normal with non-weightbearing but is limited by first metatarsal elevation secondary to ground reactive forces. The category includes no radiographic degenerative joint changes, hallucal interphalangeal joint hyperextension and pronatory architecture of the foot.3 Stage II: joint adaptation. This includes flattening of the first metatarsal head; osteochondral defect/lesion; cartilage fibrillation and erosion. There is also pain on end range of motion (ROM) with possible limitation of passive ROM; small dorsal exostosis; subchondral eburnation; periarticular lipping of the proximal phalanx, first metatarsal head and sesamoids.3 Stage III: established arthrosis. This includes severe flattening of the first metatarsal head; osteophytosis; asymmetric joint space narrowing; articular cartilage degeneration; erosions, excoriations and subchondral cysts; crepitus and pain on full ROM; associated inflammatory joint flares.3 Stage IV: ankylosis. This includes obliteration of the joint space, exuberant osteophytosis with loose bodies, less than 10 degrees of ROM, deformity and/or malalignment. It also includes possible total ankylosis, possible inflammatory joint flares; local pain often resulting from skin irritation or bursitis secondary to underlying osteophytosis.3 While staging is not an exact science, the clinical and radiographic findings can aid in formulating a treatment plan and educating the patient. (For an overview of conservative management, see “A Guide To Conservative Treatment Options” below.) One should not rigidly tie various stages to specific procedures. When reviewing surgical treatment options, it is prudent to inform the patient that the appropriate surgical intervention may change intraoperatively after one has a direct view of the cartilage. The appropriate surgical intervention may also change after the surgeon completes certain steps of the procedure such as joint decompression, angular correction or joint stabilization.
A Guide To Conservative Treatment Options
Conservative treatment of hallux limitus or rigidus is not the focus of this article. However, it is important to be aware of the various conservative treatment modalities. For example, one may delay or avoid surgical intervention by utilizing a stiff soled shoe, which reportedly reduces “first MPJ dorsiflexion to 25 to 30 degrees without significantly altering gait.”7,8 Non-surgical treatment options include but are not limited to the following: custom orthotics with or without a Morton’s extension to limit first MPJ dorsiflexion, rigid graphite shanks, stiff soled shoes, extra-depth shoes or rocker bottom shoes. Injection options and medications include corticosteroid injections, NSAIDs, glucosamine and chondroitin sulfate and Synvisc injections (Hylan G-F 20 has FDA approval for knee osteoarthritis). Other treatments include joint manipulation post-local anesthesia, physical therapy, ROM exercises, splinting and activity modifications or limitations.3,9
A Primer On Joint Preservation Procedures
Surgical treatment options of hallux limitus or rigidus traditionally focused on two procedures described as joint preservation and joint destructive. More recently, surgeons have utilized specialized techniques such as arthroscopy, arthrodiastasis and the Osteochondral Autograft Transplant System (OATS) independently or in combination with traditional surgical techniques to address hallux limitus or rigidus. Joint preservation procedures include cheilectomy with joint debridement and chondroplasty.10-14 One may also perform joint realignment or decompression via various first metatarsal osteotomies such as the Watermann, Green-Watermann, Youngswick, Modified Reverdin Green, Shortening Scarf, Modified Weil or Modified Hohmann procedures.15-19 Other options for joint preservation are joint realignment or decompression via various proximal phalanx osteotomies (Bonney-Kessell, Off Set L, Akin-Scarf).20-23 Surgeons may choose angular corrections via first metatarsal osteotomies, including Lambrinudi (plantarflexing wedge) and Juvara C (sagittal oblique) and Modified Crescentic). Other options are sagittal translational corrections such as the Off Set V osteotomy, sagittal Z osteotomy and first metatarsocuneiform arthrodesis (Lapidus).12,24 Mulier, et. al., reported 90 percent “good to excellent results when performing cheilectomy in athletes for stage I and II hallux rigidus with a mean five-year follow-up.14 The athletes, who were between 19 and 45, participated in soccer, judo, volleyball, basketball, skating, dancing and tennis. Mulier noted the cheilectomy provides good results in athletes and in cases with cartilage damage to the dorsal aspect of the first metatarsal head.13,25-26 Feltham, et. al., concluded the cheilectomy should be the surgical treatment of choice for patients over 60 years old regardless of the stage of hallux rigidus.27
What You Should Know About Joint Destructive Procedures
Joint destructive procedures include resection arthroplasty with or without soft tissue interposition (Valenti, Keller, Modified Keller, Stone, Mayo), total or hemi-implants and arthrodesis.1-3,25,28-38 Reported objectives of a joint destructive procedure include “to eliminate or minimize pain, stabilize the first MPJ and allow the hallux to bear weight.”1 Bouche noted “the only procedure that achieves such long-term objectives is the first MPJ arthrodesis.”1 DeFrino, et. al., demonstrated through gait analysis and pedobarographic studies that “the stable weightbearing position and function of the first ray is restored via arthrodesis of the first MPJ.”2,39 Lambardi, et. al., reported “the first MPJ arthrodesis reconstitutes the medial column longitudinal arch by plantarflexing and stabilizing the first ray.”40 First MPJ arthroscopy, arthrodiastasis and osteochondral autogenous transplantation are specialized procedures. Surgeons may utilize these procedures independently or combine them with other joint preservation procedures. We limit independent use of these specialized procedures to posttraumatic hallux limitus, hallux rigidus and first metatarsal head osteochondral defects when void of contributing global structural or functional/positional pathology. One may use first MPJ arthroscopy to perform the following procedures: synovectomy; ablation of adhesions, fibrous bands and scar tissue; removal of loose bodies; debridement and drilling of osteochondral defects; cheilectomy and debridement of osteophytes.41-43 Van Dijk reported no improvement in two patients and a slight improvement in three patients following arthroscopy for hallux rigidus. He also reported “good or excellent results in seven of 12 patients post-arthroscopy for first MPJ impingement syndrome with limited ROM and dorsiflexion; and good to excellent results in three of four patients post-arthroscopy for osteochondritis dissecans.”42 Van Dijk also noted “promising results” for professional athletes with first MPJ dorsal impingement syndrome.42 Ferkel reported post-arthroscopy results on 21 patients with various first MPJ pathologies and noted 73 percent had good results, 13.5 percent had fair results and 13.5 percent had poor results.42 Ferkel also noted that the most common indication for first MPJ arthroscopy was “degenerative joint disease including chondromalacia, mild to moderate dorsal osteophytes and mild limitation of motion.”41 One may utilize first MPJ arthrodiastasis to break up scar tissue, reduce contractures, reduce tension of deforming soft tissue structures and promote healing. Talarico, et. al., presented this option as a joint restorative procedure and noted the “purpose of distraction is to stretch the periarticular soft tissue structures in a staged process, causing lengthening and increasing the joints’ functional range of motion.”9 Talarico, et. al., noted excellent long term results in 133 patients who had a mix of stage I, II and III hallux rigidus.9 At one year post-op, the study noted an average score of 8 on the American Orthopedic Foot and Ankle Society Hallux Metatarsophalangeal-Interphalangeal score. The score indicates patients had no limitations of daily activities, including employment responsibilities, or limitation of recreational activities. Intraoperative distraction of 5 mm is desirable and one should maintain this for one week followed by a gradual increase in diastasis up to 8 to 12 mm over a two-week period, according to Talarico. Removing the external fixator is recommended after five to six weeks of joint distraction and one should provide immediate physical therapy for a minimum of two weeks.9 One may use osteochondral autogenous grafting and the Osteochondral Autograft Transplantation System (OATS) to replace regions of isolated first metatarsal head cartilage defects in an attempt to reduce pain and improve function.
Essential Surgical Considerations
Now let us turn our attention to our treatment plan for hallux limitus, hallux rigidus and first MPJ osteoarthritis. We will provide specific surgical treatment recommendations for stage I, II and III hallux rigidus in the presence of first metatarsocuneiform joint hypermobility. We also provide our approach to arthrodesis of the first MPJ in the presence of stage IV hallux rigidus. These recommendations are based upon our experience as well as the literature. However, it is important to remember that each case is unique and it is not uncommon for patients’ pathology as well as their desires and expectations to fall outside of the structured environment of a first MPJ classification system. Accordingly, one must identify the etiology as structural or functional/positional with or without concomitant midfoot, rearfoot, ankle or leg pathology. Give equal attention to the patient’s daily activities, specific athletic event, expectations, goals, past medical history, health and physiological age. Establish realistic expectations and goals, and ensure the patient understands the proposed result of surgical intervention. We believe the etiology of hallux rigidus is usually functional/positional and secondary to pathology at or proximal to the Lisfranc’s joint. Therefore, unless one can accomodate both structural and functional/positional etiologies, surgical intervention is recommended. We favor addressing the global pathology via surgical intervention specific to the first MPJ as well as correcting associated findings such as a hypermobile first ray, structural first metatarsal elevatus, midfoot fault, rearfoot valgus or equinus. Kilmartin presented “a prospective study of age-matched and condition-matched surgically treated patients.” He reported that “neither phalangeal osteotomies or metatarsal decompression osteotomies could be considered a definitive treatment for hallux rigidus.”18 We concur with joint realignment theories proposing that realigned joints, although arthritic, may function free of pain.44 We associate the majority of hallux rigidus to hypermobility of the first metatarsocuneiform joint, and have spared stage III joints by stabilizing the first ray. Therefore, when we have identified first metatarsocuneiform hypermobility in stage I, II or III hallux rigidus, we will often combine the appropriate first MPJ joint preserving procedure with a sagittal Lapidus procedure in order to stabilize the first metatarsocuneiform joint and translate the first metatarsal plantarly. Critics of the Lapidus procedure often cite extended periods of non-weightbearing, malunion and nonunion as reasons to avoid the procedure. The authors recommend this procedure without hesitation.45-48 This recommendation is via Drs. Haro and DiDomenico based on their experience as well as the techniques and fixation utilized by the cited authors. Bednarz and Manoli point out that concerns regarding “prolonged convalescence, dorsal drift of the first metatarsal and the significant incidence of nonunion all stem from the initial use of cat gut suture as fixation.”49,50 Patel, et. al., obtained a 94.7 percent fusion rate in 215 of 227 modified Lapidus arthrodesis procedures with a minimum of six months’ follow-up.51 We recommend the first MPJ arthrodesis for stage IV hallux rigidus and for post-traumatic structural deformities resulting in severe osteoarthritis. Vanore, et. al., noted “the first MPJ arthrodesis provides stability to the medial column and allows efficient weight transfer through the medial portion of the foot.”3 Resection arthroplasties and hemi- or total joint implants are strongly discouraged in the active athletic population. When it comes to this patient populaton, various authors have noted that the resection arthroplasty is fraught with complications and destabilizes the first ray.52-55 Brodsky, et. al., referred to resection arthroplasty as being less favored and believed it deprived the first ray of its weightbearing function.2 Rogers, et. al., noted the procedure “impaired weightbearing function of the hallux with weakening of the foot or toe.”53 Baumhauer, et. al., reported post-resection arthroplasty complications that included lateral metatarsalgia in 75 percent of patients, intractable plantar keratosis in 88 percent of patients, cock-up hallux deformity in 94 percent of patients and marked shortening of the proximal phalanx in 25 percent of patients.52 Yu, et. al., noted that “complications of resection or implant arthroplasty, such as hallux malleolus, hallux extensus, flail toe, hallux abducto valgus and hallux varus, are unlikely with a successful first MPJ arthrodesis.”56 First MPJ implants are also not recommended in the athletic population as the implants do not provide definitive stabilization of the joint. Bouche, et. al., noted that surgeons should not perform joint implantation in active patients “as it is not predictable and the potential for complications is great.”1 Bouche, et. al., also stated that “if a joint implantation is performed, it is better to think in terms of when the implant fails as opposed to if it fails.”1
Pertinent Treatment Insights For The First MPJ Arthrodesis
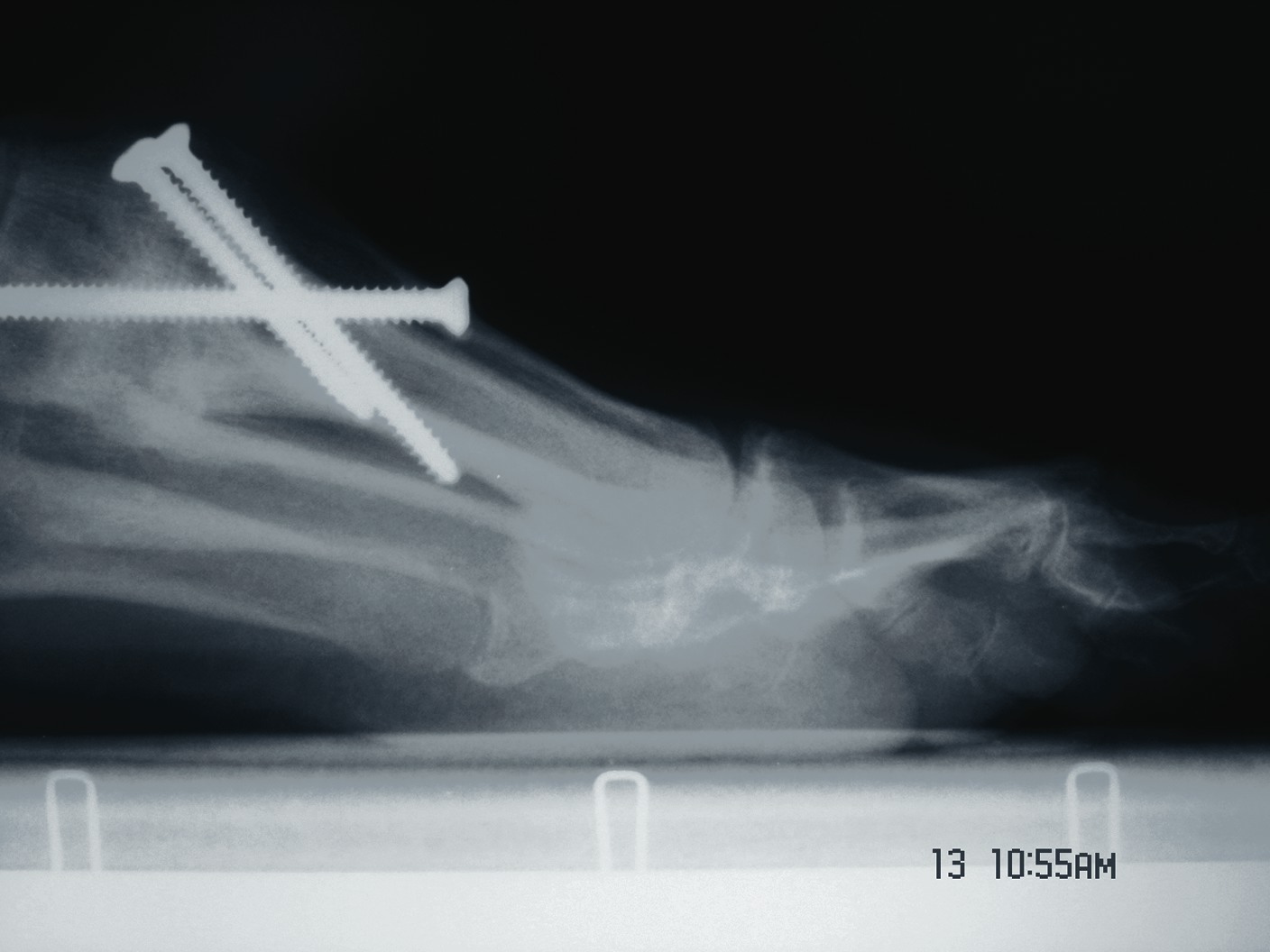
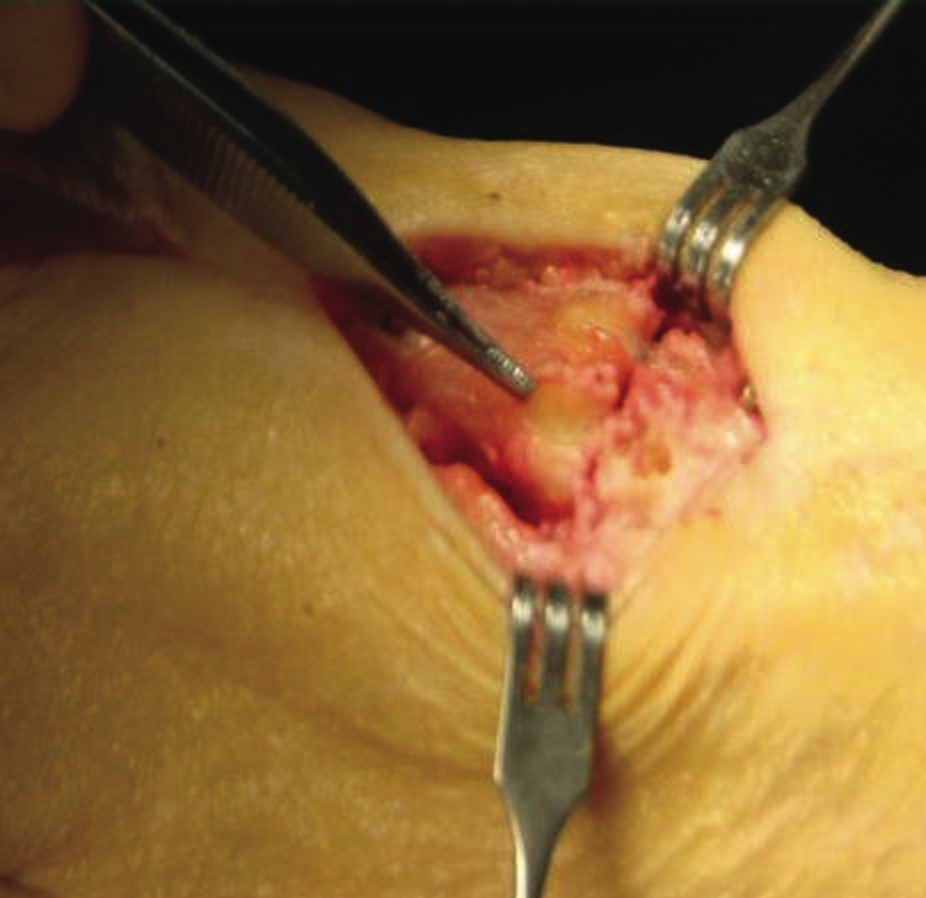
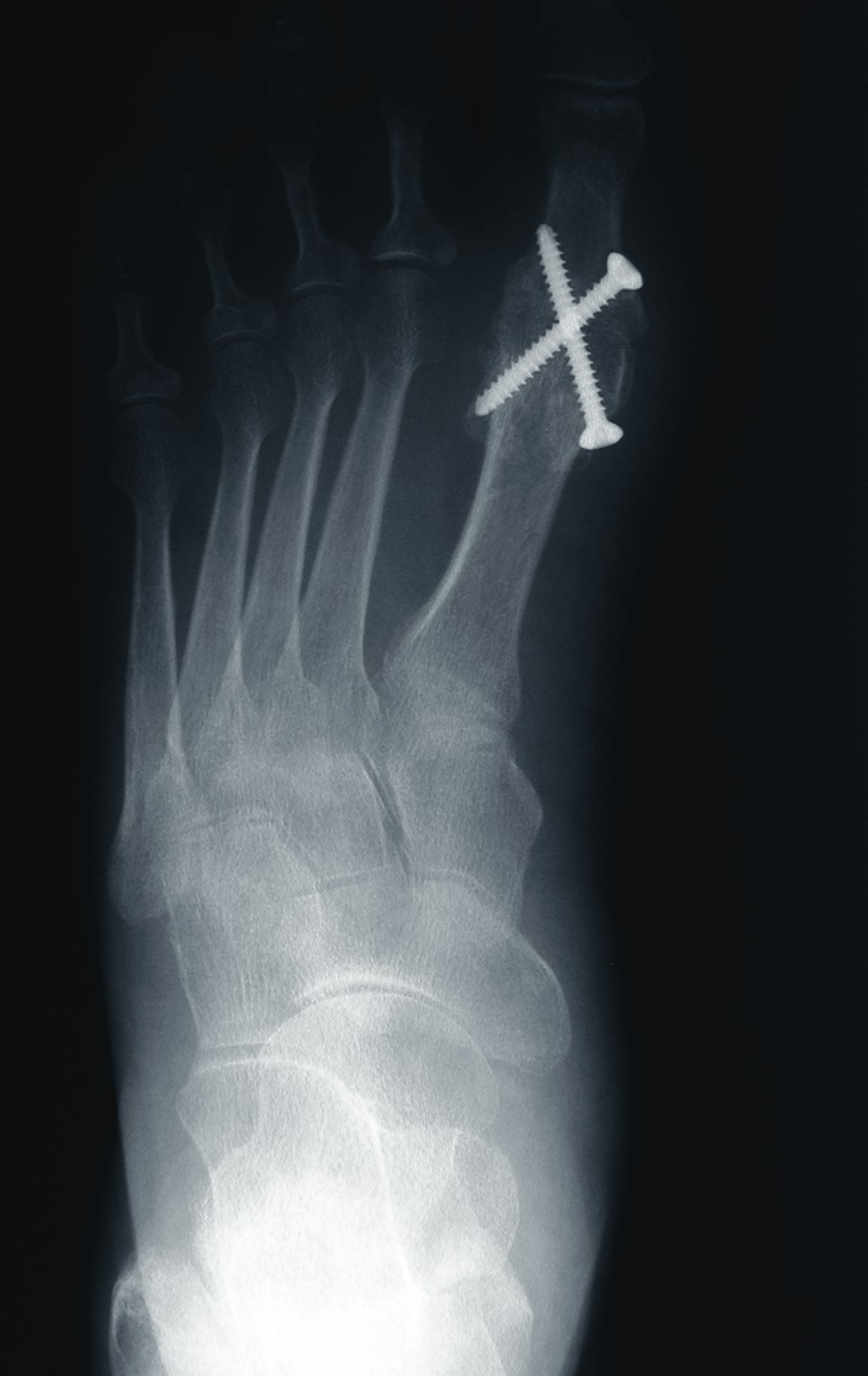
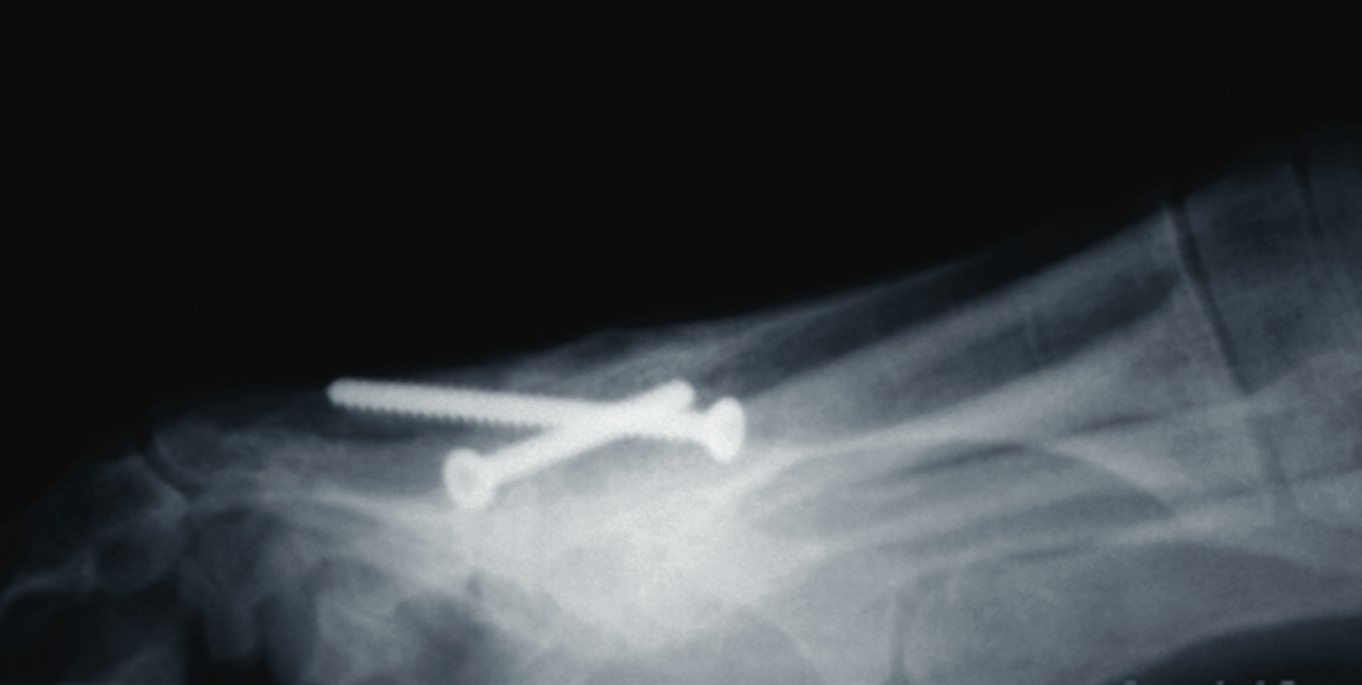
One should place the patient into a supine position and utilize a tourniquet. Evaluate post-anesthesia assessment of the first MPJ range of motion. Manually distract the first MPJ and plantarflex the first metatarsal. Dorsiflex the hallux to determine the obtainable first MPJ range of motion and evaluate for crepitus. If there is first ray hypermobility and no crepitus, one may be able to salvage the first MPJ by translating the first ray plantarly and stabilizing the medial column. Initially, surgeons should address contributing global pathology. Then proceed to the first ray and make a dorsomedial skin incision spanning the first MPJ. Retract the neurovascular structures. Make a longitudinal incision to bone, spanning the distal one-third of the first metatarsal and proximal one-half of the proximal phalanx. Evaluate the adjacent cartilage and make a critical decision to preserve or destroy the joint. It is important to realize that evaluation of cartilage quantity and quality via direct intraoperative visualization weighs heavily upon the final decision to perform a joint preservation or destructive procedure. One should strongly consider joint destructive procedures if greater than 30 percent of the dorsal portion of the first metatarsal head presents as grade III to grade IV chrondromalacia. One must independently evaluate grade III and IV chrondromalacia and osteochondral defects in the remaining 70 percent of the metatarsal head. Small cartilage lesions may yield themselves to debridement, drilling or OATS procedures whereas large cartilage defects will likely result in arthrodesis. If the joint is salvageable and one identifies first metatarsocuneiform hypermobility, perform a cheilectomy and a subsequent, sagittal Lapidus procedure. If one identifies hypermobility or posttraumatic first metatarsal angular pathology, correct it after completing the first MPJ soft tissue and osteophyte debridement. If one decides to perform arthrodesis on the joint, debride identified osteophytes, loose bodies, synovitis and scar tissue. Denude the adjacent cartilaginous surfaces to the healthy level of bleeding bone via curettage or via convex distal and concave proximal reamers. Fenestrate the adjacent bone surfaces with a 1.0- or 1.5-mm drill bit. Temporarily fixate the hallux by utilizing two K-wires in the desired position. The position should be approximately 20 to 30 degrees dorsiflexed in relation to the first metatarsal declination; abducted and parallel to the second digit; and with the nail void of frontal plane varus or valgus rotation. Obtain an AP radiograph to evaluate the bony apposition and alignment of the proposed first MPJ arthrodesis. Also obtain a lateral radiograph with the foot loaded in order to evaluate the hallux and its relationship to the first ray. After obtaining the desired position, utilize two fully threaded (3.5 or 4.0) crossing cortical screws for permanent fixation. Place the first screw from proximal medial to distal lateral and place the second screw from distal medial to proximal lateral across the first MPJ. Ensure the screws do not cross at the level of the joint. Use a 3.5-mm burr to create a dell in the cortical bone where the head of the screws engage the bone as Manloli and Hansen have described.48 After obtaining rigid internal fixation across the first MPJ, utilize a shear strain autograft (harvested via a percutaneous calcaneal grafting technique) at the arthrodesis site.57 Place the autograft in two troughs created by the 3.5-mm burr at the arthrodesis site. Use a bone mallet and tamp to provide a press fit.58
Key Postoperative Pearls
Postoperatively, surgeons may allow protected, partial weightbearing in a post-op shoe or removable walking cast for one week. Transition the patients to protected full weightbearing for an additional two or three weeks. At three to four weeks post-op, allow the patient full weightbearing in a walking shoe as tolerated. Numerous authors support early weightbearing and they report good results in the presence of early weightbearing after a first MPJ arthrodesis.59-65 Dayton, et. al., reported 100 percent union of 47 first MPJ arthrodesis procedures in 42 patients (ranging from 36 to 83 years of age), who began ambulating within one week of surgery.66 Dayton, et. al., also reported the mean time required to return to athletic shoes was 6.23 weeks.66
In Summary
First MPJ arthrodesis with surgical correction of associated pathology via a global approach is our procedure of choice for individuals who engage in an active lifestyle. While presenting each adjunctive surgical procedure is beyond the scope of this article, the authors cannot overemphasize the importance of utilizing a global approach when addressing first MPJ pathology in the presence of contributing midfoot, rearfoot, ankle or leg pathology. Accordingly, when one identifies contributing global pathology, we encourage the use of additional surgical interventions. These include a displacement calcaneal osteotomy, lateral column lengthening calcaneal osteotomy, double calcaneal osteotomy, isolated first ray arthrodesis, medial column arthrodesis, dorsal opening medial cuneiform osteotomy, percutaneous Achilles tendon lengthening, endoscopic gastrocnemius recession and a modified Kidner with or without FDL or FHL tendon augmentation. The first MPJ arthrodesis is an effective surgical procedure and boasts high fusion rates.1,3,38,54,59-74 A cheilectomy and sagittal Lapidus procedure are recommended for athletes diagnosed with stage I, II and III hallux rigidus in the presence of a hypermobile first metatarsocuneiform joint. Judicious use of specialized arthroscopy, arthrodiastasis and osteochondral autograft transplantation procedures is recommended for athletes diagnosed with stage I, II and III hallux rigidus without proximal pathology. Arthrodesis is recommended for athletes diagnosed with stage IV hallux rigidus and severe osteoarthritis. The definitive nature, medial column stabilizing effect, long-term predictability, reliability and durability of the first MPJ arthrodesis are the basis for recommending the procedure for athletic patients and individuals who expect to maintain an active weightbearing lifestyle. Although the literature specifically related to the first MPJ arthrodesis in athletes is limited, academic circles are actively discussing the topic and this should spur additional research and outcome-based studies. Dr. DiDomenico is affiliated with the Forum Health/Western Reserve Care System in Youngstown, Ohio. He is the Director of the Reconstructive Rearfoot and Ankle Surgical Fellowship within the Ankle and Foot Care Centers. Dr. DiDomenico is a Fellow of the American College of Foot and Ankle Surgeons. Dr. Haro is a Fellow of the Ankle and Foot Care Centers. He is a Fellow of the American College of Foot and Ankle Surgeons. References 1. Bouche RT, Adad JMR. Arthrodesis of the first metatarsophalangeal joint in active people. Clin Pod Med Surg 13:461–484, 1996. 2. Brodsky JW, Passmore RN, Pollo FE, Shabat S. Functional outcome of arthrodesis of the first metatarsophalangeal joint using parallel screw fixation. Foot Ankle Int 26:140-146, 2005. 3. Vanore JV, Christensen JC, Kravitz SR, Schuberth JM, Thomas JL, Weil LS, Zlotoff HJ, Couture SD. Clinical Practice Guideline First Metatarsophalangeal Joint Disorders Panel. Diagnosis and treatment of first metatarsophalangeal joint disorders. Section 2: hallux rigidus. J Foot Ankle Surg 42:124-136, 2003 4. Drago JJ, Oloff L, Jacobs AM. A comprehensive review of hallux limitus. J Foot Surg 23:213-220, 1984. 5. Regnauld B. Hallux rigidus. In The Foot, pp 345-359, edited by B Regnauld, Springer-Verlag, Berlin, 1986. 6. Schuberth JM, Elleby DH, Gerbert J, Jolly GP, Oloff JM, Pascalides JT, Vanore JV, White DL. Hallux valgus in the healthy adult. In Preferred Practice Guidelines, p 11, edited by American College of Foot and Ankle Surgeons, ACFAS, Park Ridge, IL, 1992. 7. Kubitz ER. Athletic injuries of the first metatarsophalangeal joint. J Am Podiatr Assoc 93:325-332, 2003. 8. Bojsen-Moller F, Lamoreux L. Significance of free-dorsiflexion of the toes in walking. Acta Orthop Scand 50:471, 1979. 9. Talarico LM, Vito GR, Goldstein L, Perler AD. Management of hallux limitus with distraction of the first metatarsophalangeal joint. J Am Podiatr Med Assoc 95:121-129, 2005. 10. Geldwert JJ, Rock GD, McGrath MP, Mancuso JE. Cheilectomy: still a useful technique for grade I and grade II hallux limitus/rigidus. J Foot Surg 31:154-159, 1992. 11. DeLauro TM, Positano RG. Surgical management of hallux limitus and rigidus in the young patient. Clin Podiatr Med Surg 6:83-92, 1989. 12. Kissel CG, Mistretta RP, Unroe BJ. Cheilectomy, chondroplasty, and sagittal “Z” osteotomy: a preliminary report on an alternative joint preservation approach to hallux limitus. J Foot Ankle Surg 34:312-318, 1995. 13. Mann RA, Clanton TO. Hallux rigidus: treatment by cheilectomy. J Bone Joint Surg 70A:400-406, 1988. 14. Mulier T, Steenwerckx A, Thienpont E, Sioen W, Hoore KD, Peeraer L, Dereymaeker G. Results after cheilectomy in athletes with hallux rigidus. Foot Ankle Int 20:232-237, 1999. 15. Cavolo DJ, Cavallaro DC, Arrington LE. The Watermann osteotomy for hallux limitus. J Am Podiar Med Assoc 69:52-57, 1979. 16. Feldman KA. The Green-Watermann procedure: geometric analysis and preoperative radiographic template technique. J Foot Surg 31:182-185, 1992. 17. Youngswick FD. Modifications of the Austin bunionectomy for treatment of metatarsus primus elevatus associated with hallux limitus. J Foot Surg 21:114-116, 1982. 18. Kilmartin TE. Phalangeal osteotomy versus first metatarsal decompression osteotomy for the surgical treatment of hallux rigidus: a prospective study of age-matched and condition-matched patients. J Foot Ankle Surg 44:2-12, 2005. 19. Gonzalex JV, Garrett PP, Jordan MJ, Reily CH. The modified hohmann ostoetomy: an alternative joint salvage procedure for hallux rigidus. J Foot Ankle Surg 43:380-388, 2004 20. Purvis CG, Brown JH, Kaplan EG, Mann I. Combination Bonney-Kessel and modified Akin procedure for hallux limitus associated with hallux abductus. J Am Podiatr Med Assoc 67:236-240, 1977. 21. Thomas PJ, Smith RW. Proximal phalanx osteotomy for the surgical treatment of hallux rigidus. Foot Ankle Int 20:3-12, 1999. 22. Citron N, Neil M. Dorsal wedge osteotomy of the proximal phalanx for hallux rigidus. Long-term results. J Bone Joint Surg 69B:835-837, 1987. 23. Roukis TS, Hallux proximal phalanx akin-scarf osteotomy. J Am Podiatry Assoc 94:70-72, 2004. 24. Viegas GV. Reconstruction of hallux limitus deformity using a first metatarsal sagittal-Z osteotomy [discussion, pp 261-262]. J Foot Ankle Surg 37:204-211, 1998. 25. Miler SD. Interposition resection arthroplasty for hallux rigidus. Techniques in Foot Ankle Surg 3:158-164, 2004. 26. Mulier T, Steenwerckx A, Thienpont E, Sione W, Hoore KD, Peeraer L, Dereymaeker G. Results after cheilectomy in athletes with Hallux rigidus. Foot Ankle Int 20:232-237, 1999. 27. Feltham GT, Hanks SE, Marcus RE. Age-based outcomes of cheilectomy for the treatment of hallux rigidus. Foot Ankle Int 22:192-197, 2001. 28. Kurtz DH, Harrill JC, Kaczander BI, Solomon MG. The Valenti procedure for hallux limitus: a long-term follow-up and analysis. J Foot Ankle Surg 38:123-130, 1999. 29. Saxena A. The Valenti procedure for hallux limitus/rigidus [discussion, p 511]. J Foot Ankle Surg 34:485-488, 1995 30. Kravitz SR. The Valenti procedure for hallux limitus/rigidus [discussion, pp 180-181]. J Foot Ankle Surg 35:178, 1996. 31. Weil LS. The Valenti procedure for hallux limitus/rigidus [discussion, pp 180-181]. J Foot Ankle Surg 35:179-180, 1996. 32. Grady JF, Axe TM. The modified Valenti procedure for the treatment of hallux limitus. J Foot Ankle Surg 33:365-367, 1994. 33. Keller WL. Surgical treatment of bunions and hallux valgus. NY Med J 80:741, 1904. 34. Hamilton WG, O’Malley MJ, Thompson FM. Capsular interpositional arthroplasty for severe hallux rigidus. Foot Ankle Int 18:68-70, 1997. 35. Cook KD. Capsular interposition for the Keller bunionectomy with the use of soft-tissue anchors. J Am Podiatr Med Assoc 95:180-182, 2005. 36. Leavitt KM, Nirenberg MS, Wood B, Yong RM. Titanium hemi-great toe implant: a preliminary study of its efficacy. J Foot Surg 30:289-293, 1991. 37. Gerbert J, Chang TJ. Clinical experience with two-component first metatarsal phalangeal joint implants. Clin Podiatr Med Surg 12:403-413, 1995. 38. Gregory JL, Childers R, Higgins KR, Krych SM, Harkless LB. Arthrodesis of the first metatarsophalangeal joint: a review of the literature and long-term retrospective analysis. J. Foot Surg. 29:369-374, 1990. 39. DeFrino PF, Brodsky JW, Pollo FE, Crenshaw SJ, Beischer AD. First metatarsophalangeal arthrodesis: a clinical, pedobarographic and gait analysis study. Foot Ankle Int 23:496-502, 2002. 40. Lombardi CM, Silhanek AD, Connolly FG, Dennis LN, Keslonsky AJ. First metatarsophalangeal arthrodesis for treatment of hallux rigidus: a retrospective study. J Foot Ankle Surg 40:137-143, 2001. 41. Ferkel RD. Great-toe arthroscopy. In Arthroscopic Surgery: The Foot and Ankle, pp 255-272, edited by RD Ferkel, 1996. 42. Van Dijk CN. Arthroscopy of the first metatarsophalangeal joint. In Foot and Ankle Arthroscopy, pp 207-214, edited by JF Guhl, JS Parisien, MD Boynton, 2004. 43. Iqbal MJ, Chana GS. Arthroscopic cheilectomy for hallux rigidus. Arthroscopy 14:307-310, 1998. 44. Paley D. Consequences of Malalignment. In Principles of Deformity Correction, pp 446, edited by D Paley with editorial assistance from JE Herzenberg. 45. Hansen Jr. ST. Hallux valgus surgery – Morton and Lapdus were right! Clin Pod Med Surg 13:347-354, 1996. 46. Myerson M, Allon S, McGarvey W. Metarsocuneiform arthrodesis for management of hallux valgus and metatarsus primus varus. Foot Ankle Int 13:107-115, 1992. 47. Hansen Jr. ST. Reconstructive foot surgery for common problems in the forefoot – Use of precise stable fixation borrowed from trauma fixation techniques. AO-ASIF Dialogue. (2)1:3-5, 1989. 48. Manoli II A, Hansen Jr. ST. Screw hole preparation in foot surgery. Foot Ankle Int 11:105-106, 1990. 49. Bednarz PA, Manoli II A. Modified lapidus procedure for the treatment of hypermobilehallux valgus. Foot Ankle Int 21:816-821. 50. Lapidus PW. The author’s bunion operation from 1931 to 1959. Clin Orthop 12:119-135, 1960. 51. Patel S, Ford LA, Etcheverry J, Rush SM, Hamilton GA. Modified lapidus arthrodesis: Rate of nonunion in 227 cases. J Foot Ankle Surg 43:37-42, 2004. 52. Baumhauer JF, DiGiovanni BF. Salvage of first metatarsophalangeal joint arthroplasty complications. Foot Ankle Clin N Am 8:37-48, 2003. 53. Rogers WA, Joplin RJ. Hallux valgus, weak foot and the Keller operation: an end-result study. Surg Clin North Am 27:1295-1302, 1947. 54. Coughlin MJ, Mann RA. Arthrodesis of the first metatarsophalangeal joint as salvage for the failed Keller procedure. J Bone Joint Surg 69:68-75, 1987. 55. Jordan HH, Brodsky AE. Keller operation for hallux valgus and hallux rigidus. An end result study. Arch Surg 62:586-596, 1951. 56. Yu GV, Shook JE. Arthrodesis of the first metatarsophalangeal joint: Current recommendations. J Am Podiatr Med Assoc 84:266-280, 1994. 57. Perren SM. Physical and biological aspects of fracture healing with special reference to internal fixation. Clin Orthop 138:175-196, 1979. 58. Hansen ST, Shear-strain-relieved bone graft. In Functional Reconstruction of the Foot and Ankle, pp, 485-486, edited by ST Hansen, 2000. 59. Zadik FR. Arthrodesis of the great toe. Brit Med J 2:1573-1574, 1960. 60. Mann RA, Oates JC. Arthrodesis of the first metatarsophalangeal joint. Foot Ankle 1:159-166, 1980. 61. Mann RA, Thompson FM. Arthrodesis of the first metatasophalangeal joint for hallux valgus in rheumatoid arthritis. J Bone Joint Surg 66A:687-692, 1984. 62. Johansson JE, Barrington TW. Cone arthrodesis of the first metatarsophalangeal joint. Foot Ankle 4:244-248, 1984. 63. Smith RW, Joanis TL, Maxwell PD. Great toe metatarsophalangeal joint arthrodesis: a user-friendly technique. Foot Ankle 13:367-377, 1992. 64. Niskanen RO, Lehtimaki MY, Hamalainen MMJ, Tormala P, Rokkanen PUR. Arthrodisis of the first metatarsophalangeal joint in rheumatoid arthritis. Acta Orthop Scand 64:100-102, 1993. 65. Myerson MS. Arthrodesis of the midfoot and forefoot joints, In Foot and Ankle Disorders, pp 972-983, edited by MS Myerson, Saunders, 2000. 66. Dayton P, McCall A. Early weightbearing after first metatarsophalangeal joint arthrodesis: A retrospective observational case analysis. J Foot Ankle Surg 43:156-159, 2004. 67. Beauchamp CG, Kirby T, Rudge SR, Worthington, BS, Nelson J. Fusion of the first metatarsophalangeal joint in forefoot arthroplasty. Clinical Orthop 190:249-253, 1984. 68. Coughlin MJ, Abdo RV. Arthrodesis of the first metatarsophalangeal joint with vitallium plate fixation. Foot Ankle 15:18-28, 1994. 69. Fitzgerald JA, Wilkinson JM. Arthrodesis of the metatarsophalangeal joint of the great toe. Clin Orthop 157:70-77, 1981. 70. Mann RA, Katcherian DA. Relationship of metatarsophalangeal joint on the intermetatarsal angle. Foot Ankle 10:8-11, 1989. 71. Bonney G, MacNab I. Hallux valgus and hallux rigidus: a critical survey of operative results. J Bone Joint Surg 34B:366-385, 1952. 72. Coughlin MJ. Arthrodesis of the first metatarsophalangeal joint. Orthop Rev 19:177-186, 1990. 73. Fitzgerald JA. A review of long-term results of arthrodesis of the first metatarsophalangeal joint. J Bone Joint Surg 51B:488-493, 1969. 74. Trnka HJ. Arthrodisis procedures for salvage of the hallux metatarsophalangeal joint. Foot Ankle Clin 5:673-686, 2000. For further reading, check out the archives at www.podiatrytoday.com.
References:
CE Exam #137 Choose the single best response to each question listed below. 1. Stage IV of the Modified Regnauld Classification for hallux rigidus includes how much range of motion? a) Less than 5 degrees b) Less than 10 degrees c) More than 10 degrees d) More than 15 degrees 2. According to the Modified Regnauld Classification for hallux rigidus, the characteristic signs of stage III hallux rigidus include … a) asymmetric joint space narrowing b) no radiographic degenerative joint changes c) periarticular lipping of the proximal phalanx d) All of the above 3. Which of the following is a joint preservation procedure? a) Cheilectomy with joint debridement and chondroplasty b) Resection arthroplasty c) Modified Keller procedure d) First MPJ arthroscopy 4. One may utilize first MPJ arthrodiastasis to … a) break up scar tissue b) reduce contractures c) reduce tension of deforming soft tissue structures d) All of the above 5. When it comes to hallux rigidus, the authors … a) believe the etiology is usually function/positional. b) associate the majority of hallux rigidus to hypermobility of the first metatarsocuneiform joint. c) only use joint destructive procedures for stage II and stage III hallux rigidus. d) a and b 7. Joint destructive procedures are indicated when greater than ___ percent of the dorsal portion of the first metatarsal head presents grade III and IV chrondromalacia. a) 20 percent b) 30 percent c) 50 percent d) 70 percent 8. If the first MPJ is salvageable and one has identified first metatarsocuneiform hypermobility, surgeons should perform … a) first MPJ implantation, especially in the athletic population. b) a cheilectomy and subsequent, sagittal Lapidus procedure. c) osteochondral autogenous grafting. d) None of the above 9. After reviewing radiographs and obtaining the desired position for a first MPJ arthrodesis, which of the following statements is true about the use of subsequent fixation? a) Surgeons should utilize four fully threaded (3.5 or 4.0) crossing cortical screws for temporary fixation. b) Surgeons should place the first screw from distal medial to proximal lateral across the first MPJ. c) Surgeons should ensure that two screws cross at the level of the joint. d) Place the first screw from proximal medial to distal lateral and place the second screw from distal medial to proximal lateral across the first MPJ. 10. After performing first MPJ arthrodesis, surgeons can allow which of the following for the first week postoperatively? a) Full weightbearing b) No weightbearing c) Protected, partial weightbearing in a post-op shoe or removable walking cast d) Full weightbearing in a walking shoe Instructions for Submitting Exams Fill out the enclosed card that appears on the following page or fax the form to NACCME at (610) 560-0502. Within 60 days, you will be advised that you have passed or failed the exam. A score of 70 percent or above will comprise a passing grade. A certificate will be awarded to participants who successfully complete the exam. Responses will be accepted up to 12 months from the publication date.



{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}