

What The Future Holds For Podiatric Care
New technologies abound and there is certainly no shortage of new innovations. There are new medications for diabetic neuropathic pain and antibiotic-resistant infections. There are innovative matrices that may enhance the healing environment for wounds. There are leading advances in the limb salvage arena as well as impressive modalities for facilitating bone healing. With that said, let us take a closer look at several new and emerging innovations that may prove beneficial to podiatrists and their patients. 1. Tigecycline (Tygacil™, Wyeth Pharmaceuticals). Given the prevalence of resistant strains of bacteria in lower extremity infections, podiatrists may want to consider adding a new antibiotic agent to their armamentarium. Tygacil recently received FDA approval as the first in its class of glycylcyclines to treat complicated skin and skin structure infections (cSSSIs). The manufacturer notes that Tygacil is approved for treating adults with both methicillin-resistant and -susceptible Staph aureus. It is also indicated for those with cSSSIs caused by E. coli, Enterococcus faecalis (only vancomycin-susceptible isolates), Streptococcus agalactiae, Streptococcus anginosus group, Streptococcus pyogenes and Bacteroides fragilis, according to the company. Tygacil’s broad spectrum makes it unique from other drugs for resistant gram-positive drugs such as vancomycin, daptomycin or linezolid, according to Warren S. Joseph, DPM. While Tygacil is effective against resistant gram positive cocci such as MRSA, MRSE and VRE, Dr. Joseph points out that the antibiotic is also effective against a broad range of gram-negative organisms and even anaerobic organisms, including strains resistant to many other antibiotics. “Overall, tigecycline appears to be an exciting innovation in antibiotic therapy,” says Dr. Joseph, a Fellow of the Infectious Diseases Society of America. “It may end up being a very useful, single agent therapy for complicated lower extremity infections including severe diabetic foot infections, especially given the tremendous increases in MRSA rates over the past few years.” Dr. Joseph cites a phase II study by Postier, et. al., of 109 clinically evaluable, hospitalized patients with cSSSIs. The study found both the 25 mg IV q12h dose of tigecycline and the 50 mg IV q12h doses effective at 67 percent and 74 percent respectively at the test of cure visit.1 Dr. Joseph says these results are “good but not particularly spectacular.” He believes more studies need to be conducted, particularly studies that examine the drug’s efficacy in treating diabetic foot infections. There are a couple of drawbacks to tigecycline, according to Dr. Joseph, an Attending Podiatrist at the Coatesville Veteran Affairs Medical Center in Coatesville, Pa. Tigecycline is only available via IV. Accordingly, Dr. Joseph says this would limit use of the medication to hospitalized patients or those who can undergo IV therapy at home. He adds that cost may be an issue since parenteral therapy would be more expensive than oral therapy. In clinical trials, Dr. Joseph also cites a “relatively high rate” of GI problems (mostly nausea and diarrhea) with Tygacil so one should monitor this closely.
Will Microdebridement Enhance The Treatment Of Tendon Pathologies?
2. Topaz™ Microdebrider (ArthroCare). Can minimally invasive debridement facilitate a quicker post-op recovery and improved outcomes? Using the microdebridement technology of the Topaz system, Arthrocare says podiatrists can perform minimally invasive soft tissue debridement that can aid in the treatment of tendons and fascia. Bruce Werber, DPM, has used Topaz for the past year and has had “very positive” results. He has used the product to treat various tendon pathologies, such as Achilles tendonitis, peroneal tendonitis, and stage 1 and 2 posterior tibial tendonitis, as well as a limited number of plantar fascia cases. While some of Dr. Werber’s patients take longer to heal than others, he notes that 85 percent of patients experience complete relief of pain and swelling. Out of the remaining patients, Dr. Werber says some patients had partial improvement, some failed to improve, and a small number of patients improved but suffered a recurrence. Overall, however, Dr. Werber is pleased with the results he is seeing. “Topaz provides us with an incredible tool to initiate tendon and fascial healing with minimal disruption of the surrounding tissue,” says Dr. Werber, a Fellow and Past President of the American College of Foot and Ankle Surgeons. “This is microdebridement of the tendon which generates growth factors and promotes the body’s ability to remodel and regenerate tissue.” The modality also stimulates angiogenesis, which promotes healing and very similar cellular changes to that of extracorporeal shockwave therapy, according to Dr. Werber. He adds another key advantage of using the Topaz device is that it obviates the need to release the fascia. Dr. Werber says the procedure requires a small incision, which is somewhat larger than that of the endoscopic procedures. One would make an incision of about 1 inch to expose the involved fascia, according to ArthroCare. Using the tip of the Topaz Microdebrider device, the clinician can make alternate perforations at depths between 3 and 5 mm to create a grid pattern. The small incision allows for rapid patient rehabilitation, according to Dr. Werber. The company notes that post-op care entails patients being immobilized for the first three weeks and subsequently progressing to a night splint or CAM Walker between weeks four and eight. Typically, Dr. Werber says the pain associated with the pathology resolves quickly and the surrounding swelling and pain also resolve in two to three weeks post-op. If the patient has a nodule on the tendon, he says that will usually resolve in 20 weeks.
Painful Diabetic Neuropathy: Can Delayed Release Capsules Provide Relief?
3. Duloxetine hydrochloride (Cymbalta®, Eli Lilly). Last year, Cymbalta became the first selective serotonin and norepinephrine reuptake inhibitor (SSNRI) to garner FDA approval to treat painful diabetic neuropathy. Stephanie Wu, DPM, notes the delayed release capsules sustain the levels of the two neurotransmitters that may inhibit pain. Eli Lilly cites two randomized, double-blind studies that examined Cymbalta’s efficacy in treating neuropathic pain in diabetic patients. Prior to treatment, these patients had a pain score greater than 4 on a pain scale ranging from 0 to 10 with 10 as the worst possible pain. Between the two studies, 568 patients took Cymbalta while 223 took a placebo. The studies concluded that patients taking 60 mg of Cymbalta once or twice a day for 12 weeks experienced a statistically significant reduction in their pain scores. Studies have shown Cymbalta is effective and patients tolerate it well, according to Dr. Wu, an Assistant Professor in the Department of Surgery within the William M. Scholl College of Podiatric Medicine at the Rosalind Franklin University School of Medicine. She says some studies have noted the drug has a rapid onset and sustained effect in reducing diabetic neuropathic pain. Cymbalta’s side effects include nausea, somnolence and dizziness, according to the company. Dr. Wu also notes that Cymbalta is contraindicated in patients taking MAO inhibitors, thioridazine and in those with hepatic insufficiency, end-stage renal disease or uncontrolled glaucoma. Overall, Dr. Wu believes Cymbalta is a “good, safe alternative” for patients with diabetic neuropathic pain. However, she adds that each patient has unique symptoms of neuropathy and will respond differently to treatments, meaning what works for one patient may not work as well for another. “Is Cymbalta the end-all, be-all magic drug that will help everyone with neuropathy?” posits Dr. Wu. “No. However, from the results of the published studies (thus far), Cymbalta appears effective and well tolerated, and is definitely an option that may help alleviate some of the suffering of those with neuropathy.”
Two Wound Dressings Aim To Improve Wound Healing
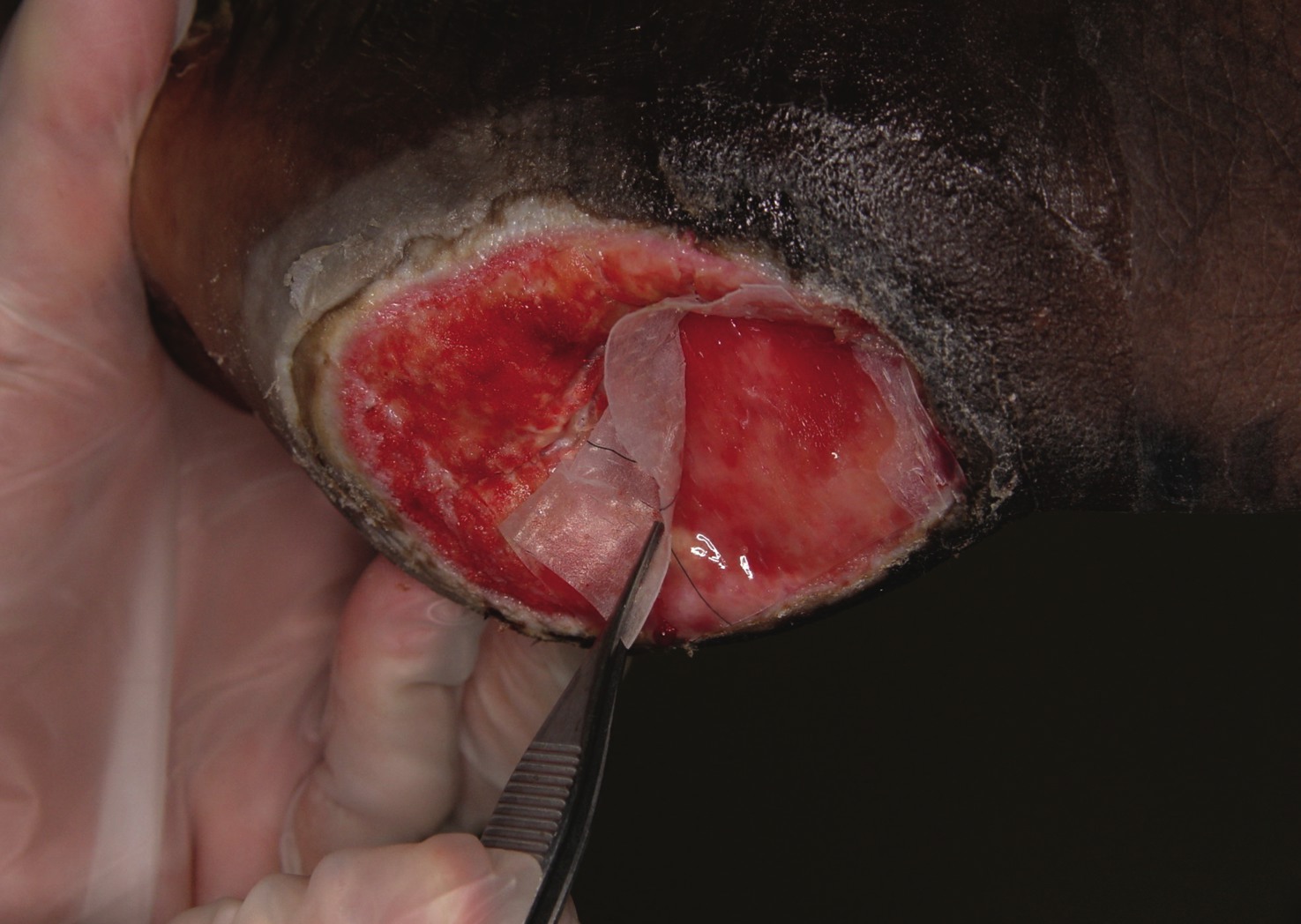
4. Integra™ Bilayer Matrix Wound Dressing (Integra LifeSciences). As more advances emerge in wound healing technology, clinicians are finding more options for patients with various types of wounds. One of the newer options is the Integra Bilayer Matrix Wound Dressing. The Integra dressing is a porous matrix of cross-linked bovine tendon collagen, glycosaminoglycan and a layer of silicone, according to the manufacturer, Integra LifeSciences. The company notes the dressing, which is made for one-time use, is indicated for a variety of wounds, including partial- and full-thickness wounds; pressure, venous, surgical, diabetic and chronic vascular ulcers; and surgical and trauma wounds. Integra cites a study of 158 ulcers in which 92 percent of 107 patients achieved complete healing either with Integra alone or with small subsidiary flaps.2 John Steinberg, DPM, has used Integra to treat patients with complicated wounds with exposed deep tissues including tendon, capsule and even bone. If the wound base has available blood flow, Integra can function as a scaffold for tissue growth, according to Dr. Steinberg, an Assistant Professor in the Department of Surgery at the Georgetown University School of Medicine. He says the ready “off the shelf” availability of Integra is a key advantage. Since the product has a very long room temperature shelf life and is kept in stock in ORs, Dr. Steinberg says Integra is available even when DPMs do not have advance notice of a patient presenting for treatment. When treating burn patients, physicians have been using Integra as a prelude to a split thickness skin graft, points out Dr. Steinberg. He says Integra’s structure serves as a scaffold for angiogenesis and promotes neodermis growth even in deep wounds. Dr. Steinberg adds that Integra functions particularly well when one combines the product with negative pressure dressings. He has had successes and failures with the dressing but maintains that using negative pressure wound dressings over Integra is key to ensuring the success of the matrix dressing. 5. Promogran Prisma™ Matrix (Johnson & Johnson Wound Management). Another wound matrix combines several ingredients into one handy package. Promogran Prisma Matrix is comprised of 55% collagen, 44% oxidized regenerated cellulose (ORC) and 1% silver ORC. Dr. Steinberg, who has used Promogran Prisma for a few months, says this combination of ingredients is an advantage since one does not need to use several different products in one wound. The matrix is innovative in that it combines matrix metalloproteinases (MMPs) with low-dose, slow release silver for an antimicrobial effect, according to Dr. Steinberg, a Fellow of the American College of Foot and Ankle Surgeons. He also points out that Promogran Prisma retains good moisture in the wound and addresses the cause of exudate rather than just absorbing exudate. Promogran Prisma is indicated for diabetic, venous and pressure ulcers as well as ulcers caused by mixed etiologies, according to the company. It is also indicated for full- and partial-thickness wounds, donor sites, abrasions, traumatic wounds and surgical wounds that have dehisced. Although Dr. Steinberg notes the product does not contain a growth factor, he says DPMs can combine Promogran Prisma with becaplermin (Regranex, Johnson & Johnson). When prescribing topical growth factors, he says he uses Prisma adjunctively in order to protect the growth factors from breakdown.
Accelerating The Healing Of Lower Extremity Fractures
6. Exogen™ Bone Healing System (Smith & Nephew). Exogen uses low-intensity ultrasound waves that penetrate into tissue and stimulate the natural process of healing bones, according to the device’s manufacturer, Smith & Nephew. The company says the treatment, which lasts 20 minutes a day, does not cause pin migration or vibration. Ultrasound waves activate the intracellular pathways to regulate the expression of genes, which subsequently synthesize proteins that speed cellular activity and the remodeling of tissue, according to Smith & Nephew. Mark Dollard, DPM, says the ultrasonic waves of Exogen stimulate the integrin receptors of bone and this effect appears to create growth factors that are needed to stimulate osteoblastic function. Reportedly, the effectiveness of growth factors, like transforming growth factor-beta (TGF-beta), insulin-like growth factor (IGF) and bone morphogenic proteins (BMP), “markedly increases” when one uses low-intensity pulsed ultrasound, according to Dr. Dollard. How effective is ultrasound technology in healing lower extremity fractures? As one study notes, Exogen healed 86 percent of non-union fractures in a group of 29 patients who received treatment for an average of four months.3 Citing double-blinded, randomized studies, Dr. Dollard says researchers have shown that Exogen accelerates fracture healing by 38 to 40 percent. He adds that animal studies have shown up to a 65 percent increase in torque strength. “Combining both accelerated healing and increased torque strength allows us to affect a more immediate remedy to the patient’s bone healing problem and return to weightbearing activities with less worry over major complications,” says Dr. Dollard, a Fellow of the American Academy of Podiatric Sports Medicine. Dr. Dollard has used Exogen for four years and says patients have had an “exceptional response” with minimal interruption to their daily lives. He says it is particularly effective in repairing non-unions. Depending upon the duration of the non-union at the time of presentation, Dr. Dollard says healing rates with the Exogen device range between 86 and 93 percent. “Due to the efficacy of this treatment and its rapid response in accelerating the healing of fractures, Medicare has removed the caveat that surgical intervention must be performed prior to approval of low-intensity pulsed ultrasound,” points out Dr. Dollard, who participated in the Centers for Medicare and Medicaid Services (CMS) review of the device.
Clearing Artery Blockages To Prevent Amputations
7. SilverHawk (FoxHollow Technologies). Patients with ischemia and peripheral arterial disease are at a significantly high risk for lower extremity amputation. Two different technologies aim to prevent amputations by clearing atherosclerotic plaque. With the SilverHawk Plaque Excision System, DPMs can treat de novo and restenotic lesions in peripheral arteries in a minimally invasive manner. The product’s tiny rotating blade shaves off plaque from the artery, collecting the plaque in the device’s tip and removing it from the patient, according to manufacturer FoxHollow Technologies. As David G. Armstrong, DPM, PhD, notes, the SilverHawk is advantageous in that it can shave off plaque without damaging the artery. “This leaves the clinician with options for future intervention should it be required,” notes Dr. Armstrong, Professor of Surgery, Chair of Research and Assistant Dean at the William M. Scholl College of Podiatric Medicine at Rosalind Franklin University of Medicine. Peter Blume, DPM, says his team has used SilverHawk for a year at the Yale School of Medicine, where he is an Assistant Clinical Professor of Surgery, Orthopedics and Rehabilitation, as well as the Director of Limb Preservation. He says the device’s advantages include treating long disease segments in a short length of time and preventing barometric trauma. “This device has enabled us to salvage limbs that have been otherwise recommended for major lower extremity amputation,” notes Dr. Blume, a Fellow of the American College of Foot and Ankle Surgeons. “The cost analysis of limb preservation has proven that prevention of limb loss far outweighs that which leads to lower extremity amputation.” FoxHollow cites a study which examined 40 infrapopliteal arteries in 29 patients with non-healing ischemic ulcers of the foot. Study researchers noted that all patients in the study would have required a major amputation if revascularization were not successful. The company notes 93 percent of patients treated with SilverHawk avoided a major amputation. It adds that 41 percent needed a toe amputation, 7 percent had a transmetatarsal amputation and 7 percent had a below-knee amputation. 8. CLiRpath® (Spectranetics). One may also employ an excimer laser to clear lower extremity artery blockages. The laser is part of the treatment of CLiRpath (Cool Laser Revascularization for Peripheral Artery Therapy). The product reaches blockages that are not accessible by standard guidewires, according to the device’s manufacturer, Spectranetics. The laser blasts through obstructions to restore blood flow and also provides an opportunity to traverse the site with a guidewire that can balloon the stenosis, according to Dr. Armstrong, a member of the National Board of Directors of the American Diabetes Association. Last year, CLiRpath’s catheters, available in diameters of 2 mm, 2.3 mm and 2.5 mm, gained FDA approval for treating artery blockages in the leg. Spectranetics cites studies in which a total of 47 patients, who were deemed poor surgical candidates, received treatment with CLiRpath. Researchers were able to achieve limb salvage in 95 percent of patients who survived to six months, according to the company. “These are modalities that now give the vascular surgeon, the interventionalist and the podiatrist greater flexibility in pushing the envelope for treatment of peripheral arterial disease,” says Dr. Armstrong of CLiRpath and SilverHawk. “The more arms we have in our armamentarium, the better equipped we are to fight the scourge of vascular disease and ischemia-related amputation.”
A Topical Solution For Actinic Keratosis?
9. Diclofenac sodium 3% (Solaraze Gel, Doak Dermatologics). Although various products are available for actinic keratosis, these products were previously not promoted to podiatrists. However, diclofenac sodium 3% (Solaraze, Doak Dermatologics) is a gel that patients can apply topically to actinic keratosis lesions on the lower extremities. As Gary Dockery, DPM, notes, the new product is a pioneer in the podiatric market and is the first FDA- approved drug containing the nonsteroidal antiinflammatory drug diclofenac sodium in a 3% formulation to treat actinic keratosis. “No company has promoted podiatry for the treatment of actinic keratosis in the past,” says Dr. Dockery, a Fellow of the American Society of Podiatric Dermatology. “This will help to decrease the conversion of skin cancer in patients as podiatrists become more familiar with this treatment mode.” Prior to the introduction of Solaraze Gel, Dr. Dockery says actinic keratosis treatment options typically included cryosurgery, 5-fluorouracil (5-FU) and aminolevulinic acid. He notes that patients will find Solaraze less irritating on the skin than 5-fluorouracil. Patients will also find that Solaraze treatments are much easier than cryotherapy sessions, according to Dr. Dockery. In terms of adverse events, Doak says the majority of adverse events were “mild to moderate” and cleared up when therapy was discontinued. The product is not indicated for children. Doak recommends using the therapy for 60 to 90 days and adds that complete healing of lesions may not be evident until 30 days after the end of the treatment regimen.
Screw Design Facilitates Enhanced Compression
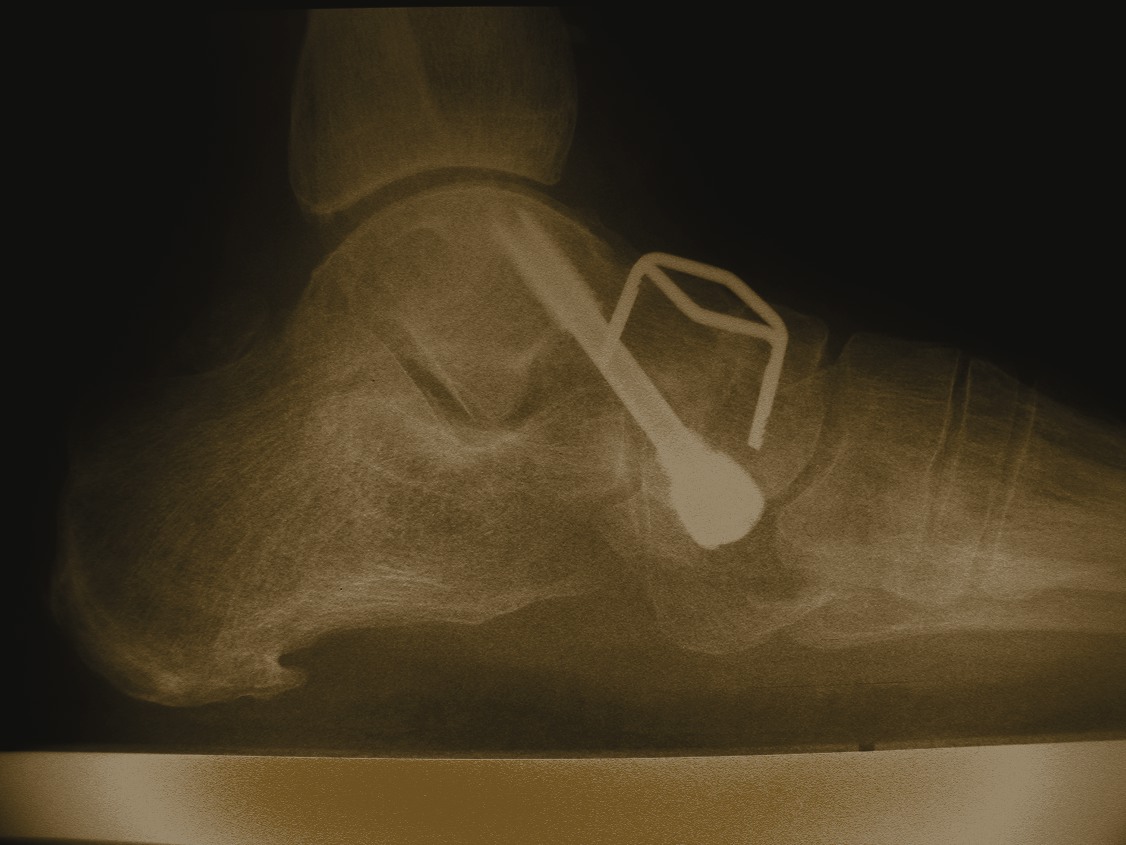
10. I.CO.S® Screw (Integra LifeSciences). Although surgeons performing internal fixation have a choice of screws, the I.CO.S (Ideal Compression) Screw may be worth a second look. Over the past two to three years, Gerard Yu, DPM, says he has had good experiences using the I.CO.S Screw. While he has not seen 100 percent healing with the screw, Dr. Yu says patients have fared well postoperatively. He says the screw seems to be “ideally suited” for major rearfoot fusions involving the subtalar and talonavicular joints, and calcaneal osteotomies. Dr. Yu, a Fellow of the American College of Foot and Ankle Surgeons, maintains the I.CO.S screw is well-designed, facilitates enhanced compression and there is less risk for complications. He says the screw’s better compression and stability are due to the threads on the head and far side of the screw. Limited in vivo testing concluded the screw gives better compression than large cancellous bone screws, according to Dr. Yu, the Director of the Podiatric Surgical Residency Program (PSR-36) and the Chief of the Section of Podiatry of the Division of Orthopedic Surgery at the St. Vincent Charity Hospital in Cleveland. Integra says the I.CO.S screw, which is available in diameters of 4 and 6.5 mm, is indicated for fixating bone fragments, foot and ankle arthrodesis, managing fractures in the foot and mono- or bicortical foot osteotomies. The product has undergone design modifications which have improved its user-friendliness, according to Dr. Yu. In terms of drawbacks, Dr. Yu notes the screw is expensive and can be somewhat difficult and time-consuming to use. There is a small learning curve associated with its use, which he says is common for all new technologies. “Experienced and wise surgeons are careful to evaluate such new products before just jumping on the bandwagon with use,” says Dr. Yu. “Thoughtful and deliberate evaluation and application minimize problems and complications.”
References:
1. Postier RG, Green SL, Klein SR, et.al. Results of a multicenter, randomized, open-label efficacy and safety study of two doses of tigecycline for complicated skin and skin-structure infections in hospitalized patients. Clinical Therapeutics, 26(5)704-714, May 2004
2. Gottlieb M, Furman J. Successful management and surgical closure of chronic and pathological wounds using Integra. Journal of Burns and Surgical Wound Care 3(4), 2004.
3. Nolte, et. al. Low-intensity pulsed ultrasound in the treatment of non-unions. J Trauma 51(4):693-703, 2001.



{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}