

How To Manage Heel Ulcers In Patients With Diabetes
Diabetic heel ulcers constitute one of the most frustrating problems for podiatric physicians. Pressure ulcers affect nearly 2 million people each year and account for annual healthcare costs that range between $2.2 billion and $3.6 billion. The heel is the second leading site for development of pressure ulcers after the sacrum.1 While patients with diabetes are living longer than in the past, the incidence of hospital-acquired heel ulcers increased from 19 percent in 1989 to 30 percent in 1993.2 Costs for heel ulcers are nearly double that of the costs associated with forefoot ulceration.2 Given the higher incidence of osteomyelitis in the calcaneus along with the presence of vascular disease, patients with diabetic heel ulcers present a significant challenge for limb salvage. It is vital to have a thorough understanding of the associated comorbidities that complicate diabetic wounds in order to manage these patients successfully and prevent potential limb loss. Accordingly, a multidisciplinary approach is essential. Initiating appropriate consults and dialogue with vascular surgery, endocrinology and internal medicine is crucial to successful treatment.
Assessing Possible Etiologies
As part of the preliminary evaluation, one should determine the etiology of the ulcer. The most common contributing factors to the development of diabetic heel ulcers include diabetic neuropathy, immobility, structural deformity, peripheral vascular disease, trauma and age. Additional factors may include shearing/friction, temperature, age, edema and anemia.3 Diabetic neuropathy is the most critical component in the development of the diabetic ulcer. Whether precipitated by repetitive stress from poor weight distribution or from dyshidrosis and fissuring from autonomic neuropathy, one must assess the presence and extent of neuropathy in order to prevent these types of ulcers effectively. A lack of mobility can generate excessive levels of pressure to the skin among older patients and those with deformity or illness. Poor mobility in the presence of edema and/or vascular disease can be a major factor in the development of an ulceration. Heel ulcers represent localized areas of cellular necrosis that result from prolonged circulatory interference from pressure or shearing forces. Although pressure is a critical factor involved with skin breakdown, researchers have shown that shearing forces (stretching of blood vessels) compound the ischemic changes produced by external pressure and lead to an increased rate of tissue breakdown.4 If the heel is subjected to prolonged periods of pressure that exceed capillary pressure, ulceration will result. In addition to pressure and friction, the shock absorption in the heel declines with age. The decreased shock absorption contributes to tissue breakdown and increased morbidity. Atrophy of muscle and fat tissues in patients with diabetes has been proposed as one of the possible factors that increases the risk of ulceration. Researchers have determined that heel thickness in non-ulcerated patients with diabetes is 2 mm less than the heel thickness in non-diabetic patients.5 Diabetic patients with a history of ulceration have heel thicknesses 3 to 4 mm less than non-diabetic patients.5
Why It Is Essential To Evaluate The Whole Patient
It is also essential to evaluate the entire patient and not just the wound. Indeed, one must also assess the etiology of the wound as well as the patient’s medical status, nutritional status and any relevant comorbidities. Wound healing and infection control will be significantly impaired in the hyperglycemic diabetic patient. Many studies have shown impaired angiogenesis, impaired formation of coronary collaterals and lower levels of nitric oxide among many other deficits that will impact wound healing among patients with diabetes. When treating heel ulcers in these patients, one must also consider additional comorbidities including edema, anemia, pulmonary and renal insufficiency. Edema interferes with the diffusion rate of oxygen and nutrients from the capillary to the cell while anemia reduces the amount of oxygen carried through the circulatory system. Although a patient may have reduced blood flow, the blood with normal hemoglobin and oxygen content greatly enhances the survival of tissue.6 As treatment for the heel ulceration may require surgical debridement and vascular intervention, addressing these issues via multidisciplinary involvement becomes even more pertinent to prevent or reduce the risk of surgical complications and morbidity.
How Nutritional Status Affects Ulcer Healing
Aside from controlling diabetes, nutrition is a concern for diabetic patients with ulcers. Protein insufficiency is a major factor in the healing of ulcers. Patients with pressure related ulcers should be eating 80 to 100 gm of protein each day. This will involve appropriate supplementation to the patient’s regular three meals a day. Low protein levels slow wound healing, decrease immunocompetence, increase susceptibility to infection and lengthen hospital stays. Specifically, vitamin A deficiency will inhibit the early inflammatory phase. This facilitates a reduction in fibronectin on the wound surface and a decrease in cell chemotaxis, adhesion and tissue repair. Vitamin A supplements can increase collagen synthesis and wound tensile strength along with lymphocyte activation. There are approximately 200 zinc-requiring enzymes in the body. Zinc deficiency will cause delayed closure of wounds and ulcers, and reduced collagen tensile strength. Vitamin C deficiency can lead to the breakdown of already healed wounds. Stress associated with injury and wound healing results in an increased need for vitamin C. Appropriate levels of vitamin C will increase skin strength and fibroblastic content of scar tissue. Vitamin E has an antiinflammatory action due to its ability to decrease the production of prostaglandins. Vitamin E also enhances the immune response and has been shown to enhance the breaking strength of postoperative wounds. Nutrition is just as important for preventing pressure ulcers as it is in treatment. Poor hydration, declining body weight and low serum protein concentrations play a major role in compromised tissue strength. Obtaining timely and appropriate nutritional and hydration status of the patient is essential for preventing skin breakdown.7
Recognizing The Importance Of Vascular Status
When treating ulcers, it is essential to determine the vascular status. A palpable posterior tibial pulse is the best clinical indication of blood flow to the heel. If pulses are not present, obtaining timely non-invasive vascular tests (ankle brachial indexes and arterial Doppler studies) is vital to obtain a more complete picture of the patient’s vascular status. Any significant isolated drop in pressure is evidence of possible stenosis. Normal values in a clinically ischemic limb can be evidence of arterial calcification. If the wound is infected and ischemic, clinical judgment must dictate the timing of surgical intervention versus the performance of ancillary vascular testing. In many cases, one may proceed with surgical intervention in the hospital setting and obtain a vascular surgery consult simultaneously. Clearly, if the patient is septic, surgical intervention is the priority. However, if the patient has no infection or questionable contamination, surgical intervention may not be indicated. Always ensure the vascular surgeon is on board with any decisions that may impact the ability to heal the wound after surgery. Careful planning for coverage of the post-op wound site is vital to ensure you are not creating a worse situation than when you started. Toe photoplethysmography and transcutaneous PO2 and PCO2 levels can also be helpful to evaluate tissue perfusion and the extent of potential microvascular disease. Angiograms and MRAs may be indicated for potential surgical candidates. Palpating pedal pulses is always the first clinical test one should perform. Assessing the posterior tibial pulse is the best indication of flow to the heel. If there is a pre-ulcerative or inflamed area at the heel, assess the presence of blanching or nonblanching with palpation. In toe photoplethysmography tracings (PPGs), normal tracings are usually sufficient to eliminate the possibility of arterial disease contributing to a chronic wound. Flat tracings point to a danger of tissue breakdown. TcPO2 levels below 20 mmHg indicate poor tissue perfusion while levels below 10 mmHg can be indicative of necrosis. Always consider noninvasive testing with segmental blood pressures, pulse volume determinations and Doppler arterial mapping for proper evaluation of the at-risk ischemic patient. If renal function is in doubt and the patient is still a possible candidate for bypass, obtain a MRI arteriogram. Obtaining an arteriogram as a routine test for patients with severe disabilities and others who are not viable candidates for vascular surgery is not recommended. Revascularization of the limb should always be the goal of vascular intervention. However, the presence of multi-segmental occlusive disease below the knee (involving the posterior tibial artery) is often preventative. The sooner revascularization can occur, the sooner healing can begin. There is no benefit in waiting to see if a superficial eschar will become full thickness necrosis. No matter how bad the prognosis, always follow the vascular route as far as it goes. Before surgery or any other treatment, exhaust all vascular options first.
When One Sees Or Suspects Osteomyelitis
If one detects present or potential bone exposure in the wound, obtain radiographs. Although osteomyelitis is a clear indication for surgical excision, be sure to confirm the patient’s ability to heal after surgery and the options for coverage. If the patient has chronic osteomyelitis without an active infection, the best option may be continuing conservative wound care. One must use his or her clinical judgment to determine if surgery is necessary in order to facilitate healing.
Assessing The Wound Characteristics
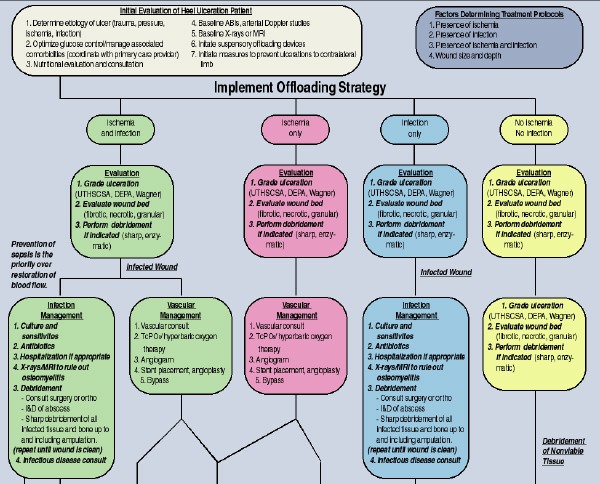
One must closely evaluate several critical factors prior to implementing treatment for the diabetic heel ulcer. Accordingly, one should evaluate the depth of the wound and check for the presence of infection, ischemia or the presence of both. The depth of the wound in the face of infection or ischemia ultimately determines prognosis and treatment. Although the Depth Extent Phase and Associated Etiology score is a helpful tool to grade and classify heel ulcers, we prefer the University of Texas Foot Risk and Wound Classification System for these wounds because of the system’s simplicity and its ease in determining prognosis.8 Our proposed algorithm (see below) attempts to illustrate the importance of coalescing multiple factors in order to plan a logical and concise line of treatment. No matter what classification system one uses, remaining consistent with the wound grading process is important in order to accurately predict outcomes and progress. Appropriate evaluation of the wound site should include a thorough description of the wound bed and the surrounding tissues. In order to provide appropriate treatment for the specific state of the wound, it is important to recognize all wounds are evolving.
Ischemic Heel Ulcers: Should You Pursue Debridement?
For example, consider the presence of the classic black eschar overlying the diabetic heel ulcer. Based on the characteristics of the eschar and the presence of infection, ischemia or both, one can make a judgment as to whether to debride the eschar. Even without the presence of eschar, knowing what to look for in and around the wound is vital. One should assess: • adherence or non-adherence of the eschar to underlying tissues; • odor; • the presence of fluctuance (abscess); • the wound margins (hyperkeratotic, wet, granular or fibrotic); • the presence of drainage (mild, moderate or heavy); • whether there is bone exposure; and • the wound bed (granular, fibrotic, stringy, wet or necrotic). The development of black eschar overlying a heel ulcer (or any ulcer) represents a significant challenge. Eschar formation has been described as a process in which skin necrosis occurs due to either a focal prolonged period of excessive pressure to the area or a more generalized peripheral arterial occlusive disease. With the presence of fluctuation or abscess formation under the eschar, one must perform debridement to prevent sepsis and osteomyelitis. Although the prevention of sepsis takes priority over the immediate restoration of impaired vascular status, this does not warrant being overly aggressive in the operating room. Moreover, despite the presence of infection, one should still pursue an appropriate vascular workup. Obtaining a vascular surgery consult is highly recommended when considering surgical intervention of the infected heel ulcer. Clinically, the infected “wet” heel eschar can present in many ways but the most common findings include drainage, malodor, non-adherence of the eschar from the wound base and a fluctuance or “soupy” feel upon palpation. One should consider obtaining X-rays or a MRI to rule out osteomyelitis in these patients. If one is going to perform surgical debridement, consider getting a bone biopsy. If the infection is not cleared in a timely manner, a calcanectomy or further lower leg amputation becomes inevitable. Often, the ischemic heel ulceration can present in a state in which the eschar is only partially adhered with only marginal subcutaneous fluctuance. These ulcers are often challenging as they have not yet become grossly infected but do reflect a pre-abscess/infected state. When treating these patients, one should implement prophylactic infection control with attempts to dry the wound and accordingly prevent the formation of wet, necrotic tissue. In the vast majority of these cases, conservative treatment of these “marginal eschars” should take precedence over surgical intervention. When treating patients with adequate blood flow, clinicians should debride any necrotic nonviable tissue that may impair wound healing. One may need to perform debridement on a regular basis along with offloading in order to maintain a healthy wound. Unnecessary debridement of the ischemic wound can increase the wound size and the demand for blood flow to the area. This inevitably will result in exposure of bone and/or tendon, increasing the risk of osteomyelitis and tendon deterioration. With any ischemic eschar, maximizing vascular flow should be the primary goal prior to any debridement unless there is infection. While not as common, it is possible for black eschar to form in the presence of adequate systemic arterial circulation (excessive focal pressure to the heel). If these ulcers develop as a result of localized skin necrosis from prolonged periods of pressure that exceed the capillary pressure of the skin, offloading and local wound care can often facilitate healing. In these cases, careful debridement may be indicated as the eschar sloughs. Whether from focal pressure or from severe arterial occlusive disease, one must implement an immediate and effective offloading and revascularization strategy in order to have success in healing these complicated wounds.
How Offloading Can Benefit The Patient
It is not easy to address pressure reduction in the heel. If an offloading device is not properly fit, it may create pressure in other places or make an existing ulcer worse. While it may not be appropriate in all cases, researchers have shown that using a standard hospital head pillow beneath the legs to suspend the heels off the bed surface is more effective than many specialty products.9 Immediate offloading is imperative to initiate wound healing and protect the heel throughout the healing process. There are a wide variety of devices available for preventative therapy but once the ulceration occurs, a pure suspensory device such as a Multi Podus boot is the most appropriate. Once a heel ulcer has developed, any pressure is too much pressure. Maintaining full-time use of a suspensory boot can be a challenge as it requires educating the patient and the nursing staff to monitor and ensure that the boot is being used 24 hours a day. Without relieving the pressure, the wound will fail.
An Overview Of Advanced Wound Care Options
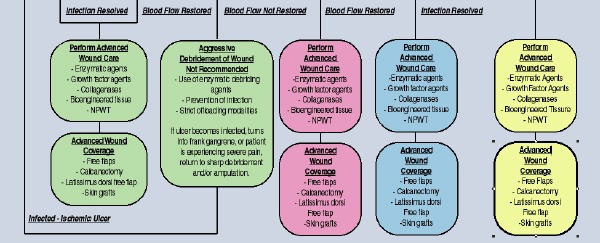
Once one has achieved revascularization and eradicated infection, one can proceed to employ good wound care healing principles. Advanced wound care options may include the use of enzymatic debriding agents, collagenases, growth factors, bioengineered tissues or the use of negative pressure wound therapy (NPWT). For those patients with adequate circulation, NPWT is our treatment of choice for heel ulcerations. Under some circumstances, hyperbaric oxygen (HBO) may be an adjunctive option along with surgical debridement and antibiotic therapy for anaerobic or polymicrobial infections of the soft tissues. One may achieve improved tissue oxygenation during HBO therapy. Researchers have shown that HBO helps support poorly perfused and hypoxic areas. Although much more could be said about these modalities (among others), the key point is to know the options and be prepared. Revascularization can often have limited results among patients with diabetes and it is essential to implement the right wound care solution at the right time. Also keep in mind that if one does not ensure adequate offloading during this or any phase of healing, no treatment will work. Advanced wound coverage can include calcanectomy with primary closure, free flaps, latissimus dorsi free-flap and skin grafts. However, one would usually reserve this type of wound coverage for the younger, more active and ambulatory patient who has adequate blood flow. Those patients with poor blood flow have a significantly higher risk of procedure failure and subsequent limb loss. Lastly, amputation should always remain an option for those with severe infection with bone involvement or those with gangrenous tissues in and around the heel. In many of these cases, amputation may allow patients to move on with their lives and, in some cases, allow them to regain their quality of life.
Seven Ways To Prevent Ulcerations To The Contralateral Limb
The same factors that cause an ulceration on one foot may cause ulceration on the other foot. Be sure to check the other foot routinely for preulcerative changes. Recognizing early skin changes indicating impending skin breakdown is critical. Initial changes are indicated by inflammation of the skin that blanches upon digital pressure and may remain blanched several hours after pressure is relieved. Without offloading, this area will progress into increasing inflammation and into non-blanching erythema that is followed by induration of the underlying tissue. Without intervention, the area will rapidly progress into ulceration. It only takes 30 to 60 minutes of ischemia to initiate heel necrosis. Therefore, one must emphasize the following preventative measures to the patient or the patient’s caregiver for the contralateral limb. • Make sure the patient’s bed is positioned so the hips are higher than the toes. • Make sure the foot is entirely offloaded in bed or while the patient is sitting. The weight of the foot itself is enough to impede blood flow into the skin, resulting in skin breakdown. • Utilize foot boards, pillows or other modalities to prevent sheets or bedding from applying pressure to the toes. • Make sure bandages are changed one to four times a day. Wet or moist bandages can cause maceration and facilitate infection. Furthermore, blood to the skin can be impeded by dressings that are too tight. • Keep patients warm. Even in normal legs, healing is slowed in cold tissue. • Avoid wetting open heel ulcers in showers or tubs. Patients should clean their open wounds separately to prevent contamination, especially by Pseudomonas and fecal elements common in showers or baths. • Avoid exposing the wound to extreme temperatures. Excess heat can increase tissue metabolism and increase the need for oxygen. Heat may promote the death of borderline tissue.
In Summary
Treating the diabetic heel ulcer can be a daunting task with unique challenges. Although many of these patients often require amputation, aggressive vigilance and monitoring of these wounds is vital in order to stay one step ahead. The authors hope this algorithm for treating the diabetic heel ulcer can at least help facilitate appropriate clinical decision-making when it comes to addressing these complicated wounds. The most important thing to remember is that it is a lot easier to prevent these wounds than to treat them. Everyone involved in the care of an at-risk patient must be made aware of not only the causes of pressure ulcers, but also the devastating consequences that can develop along with associated patient morbidity. For patients who are in wheelchairs, those who are bedridden or those patients who have diabetic neuropathy, one must explain and strongly emphasize to the patients the importance of daily home inspection of their feet. One can prevent heel ulcers but high tech gadgets or devices will never be a substitute for thorough and conscientious skin care. Dr. Moore has a Master’s degree in medical education and is a former University of Texas Diabetic Foot Fellow practicing in Somerset, Ky. Dr. Jensen is the Director of Lower Extremity Care at the Russell County Wound Care Center and works with Dr. Moore in private practice in Somerset, Ky. References 1. Bloomgarden ZT. The diabetic foot. Diabetes Care 2001;24(5):946-51. 2. Tourtual DM, Riesenberg LA, Korutz CJ, et. al. Predictors of hospital acquired heel pressure ulcers. Ost/Wound Manage 1997; 43(9):24-40. 3. Younes NA, Albsoul AM, Awad H. Diabetic Heel Ulcers: A Major Risk Factor for Lower Extremity Amputation. Ost/Wound Manage, Issue Number: 6 4. Reichel SM. (1958). Shearing Force as a Factor in Decubitus Ulcers in Paraplegics. Journal of the American Medical Association, 166, 762-763. 5. Kinoshita H, Francis PR, Murase T, Kawai S, Ogawa T. The mechanical properties of the heel pad in elderly adults. Eur J Appl Physiol Occup Physiol. 1996;73(5):404-409. 6. Armstrong DG, Nguyen HC. Improvement in healing with aggressive edema reduction after debridement of foot infection in persons with diabetes. Arch Surg. 2000;135(12):1405-1409. 7. Leininger SM. The role of nutrition in wound healing. Critical Care Nursing Quarterly. 05-01-2002 8. Ovington LG. Prediction, Prevention of Heel Pressure Ulcers. Wound Care newsletter, November 1998. 9. Armstrong, DG, Lavery, LA, Harkless, LB. Validation of a diabetic wound classification system. The contribution of depth, infection, and ischemia to risk of amputation. Diabetes Care 1998; 21: 855-859. Additional Reference 10. Laing P. The development and complications of diabetic foot ulcers. Am J Surg 1998;176(Suppl 2A):11S–19S. CE Exam #128 Choose the single best response to each question listed below: 1. The heel thickness of non-diabetic patients is ___ thicker than in diabetic patients with a history of ulceration. a) 3 to 4 mm b) 1 to 2 mm c) 2 to 3 mm d) 2 to 4 mm 2. Common findings with an infected, wet heel eschar include: a) Fluctuance upon palpation b) Malodor c) Non-adherence of the eschar from the wound base d) All of the above 3. When determining vascular status, what can an isolated, significant decrease in pressure signify? a) Microvascular disease b) Possible stenosis c) Erythema d) Arterial calcifcation 4. With toe photoplethysmography (PPG) tracings, what would flat tracings signify? a) Sepsis b) A danger of tissue breakdown c) Superficial eschar d) Osteomyelitis 5. What is the initial sign for ulcerations to the contralateral limb? a) Non-blanching erythema b) Induration c) Poor pedal pressure d) Inflammation of the skin that blanches after digital pressure 6. What is the primary goal when one finds ischemic eschar? a) Debridement b) Offloading c) Maximizing vascular flow d) None of the above 7. Which advanced wound care treatment may be effective in treating anaerobic infections in soft tissue? a) Hyperbaric oxygen b) Negative pressure wound therapy c) Growth factors d) Amputation 8. TcPO2 levels below __ may indicate necrosis. a) 30 mmHg b) 20 mmHg c) 10 mmHg d) 5 mmHg 9. Unnecessary debridement of the ischemic wound … a) Can increase the wound size b) Decreases the demand for blood flow to the area c) May lead to exposed bone and/or tendon d) a and c 10. How much protein should patients with pressure ulcers eat a day? a) 60 to 80 gm b) 60 to 90 gm c) 80 to 100 gm d) 100 to 120 gm Instructions for Submitting Exams Fill out the enclosed card that appears on the following page or fax the form to the NACCME at (610) 560-0502. Within 60 days, you will be advised that you have passed or failed the exam. A score of 70 percent or above will comprise a passing grade. A certificate will be awarded to participants who successfully complete the exam. Responses will be accepted up to 12 months from the publication date.



{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}