

MRSA: Where Do We Go From Here?
Foot ulcers are a major predictor of future lower limb amputations. Fourteen to 24 percent of patients with diabetes with foot ulcers eventually require an amputation and more than 60 percent of nontraumatic lower extremity amputations occur in those with diabetes.1,2 Although risk factors may vary, the majority of diabetes-related amputations result from peripheral arterial disease, peripheral neuropathy or infection.3 The healthcare costs associated with diabetic foot infections are staggering. In an analysis of medical and pharmacy insurance claims filed by more than 7 million people during a two-year period, Holzer, et. al., reported that the direct medical expenditures associated with lower extremity ulcers in patients with diabetes exceeded $16 million and 80.7 percent of those costs were hospital-related.4 Overall, 6 percent of diabetic patients with foot ulcers require hospitalization.3 According to data from the 1983-1990 National Hospital Discharge Surveys (NHDS), chronic ulcers were present in 2.7 percent of all hospitalized patients with diabetes.5 The average hospital length of stay for patients with an extremity ulcer was 59 percent longer than for those without an ulcer. Patients without ulcers remained in the hospital about 10 days whereas those with ulcers stayed approximately 15 days. Although up to 90 percent of ulcers will heal when they are treated aggressively with a comprehensive approach, recovery can be slow.6 Ulcers may take weeks or months to heal, and patients remain at high risk for ulcer recurrences.7 Ramsey, et. al., reported that diabetic foot ulcers are predictive of increased mortality.8 Among 8,905 patients with either type 1 or type 2 diabetes, the cumulative three-year survival rate was 72 percent for patients with a foot ulcer versus 87 percent for those without ulcers. While not all diabetic foot ulcers become infected, delayed or inadequate treatment can result in an infection that may lead to gangrene, osteomyelitis or even limb amputation. The risk of infection remains high in these cases even when lesions are treated quickly and appropriately.
What The Literature Reveals About The Rise Of MRSA
Antibiotic resistance is a growing problem in diabetic foot infections. In particular, methicillin-resistant Staphylococcus aureus (MRSA) pathogens have been isolated with increasing frequency from wound and skin infections that commonly affect the lower extremities of patients with diabetes. For these individuals, foot infections caused by MRSA organisms have been associated with poorer outcomes related to an increased risk of amputations and infection-related mortality. Wheat, et. al., collected 54 specimens from infected foot ulcers in diabetic patients and identified Staphylococcus isolates in 34 (64 percent) specimens and Streptococcus isolates in 16 (30 percent) specimens.9 In another study involving 111 patients with diabetic foot infections, El-Tahawy reported that S. aureus was identified in 28 percent of cases and was the most common pathogen isolated.10 Other isolated organisms included Pseudomonas aeruginosa (22 percent), Proteus mirabilis (18 percent) and anaerobic gram-negative bacteria (11 percent). Enterococci have frequently been cultured from infections in patients who have been previously treated with cephalosporins whereas Pseudomonas species are often identified in patients whose ulcers have been soaked or treated with wet dressings.11 The prevalence of infections caused by MRSA organisms continues to rise. MRSA has become a major nosocomial pathogen and has caused up to 12 percent of all bacteremias, 28 percent of surgical wound infections and 21 percent of skin infections.12 There is also an increasing prevalence of skin and soft tissue infections caused by community-acquired MRSA, which greatly differs from nosocomial MRSA strains. At an outpatient foot clinic, MRSA accounted for 30.2 percent of infections in about one-third of patients with infected foot ulcers, a nearly twofold increase over a three-year period.13 The increase in MRSA infection rates occurred even though prescribers had changed their antibiotic prescribing practices. Despite the rising prevalence of MRSA infections in the study population, the overall proportion of infections caused by S. aureus remained unchanged during the same three-year period. An investigation by Tentolouris, et. al., among outpatients reported that S. aureus was the most prevalent pathogen of gram-positive aerobes isolated from wounds and MRSA organisms comprised 40 percent of S. aureus isolates.14 Researchers found that infections caused by MRSA were more common among patients who were previously treated with antibiotics than in those who were antibiotic naïve. Among hospitalized patients, El-Tahawy found that 30 percent of all S. aureus pathogens isolated from diabetic foot lesions were methicillin resistant.10
Does MRSA Have A Significant Impact On Mortality Rates?
Overall, MRSA infections have been associated with increased morbidity, extended hospital stay and increased costs. However, literature on the effect on mortality has been mixed. When it comes to diabetic foot infections, the presence of MRSA may lead to poorer outcomes, an increased risk of amputations, higher treatment costs and increased mortality.13,15 Fejfarova, et. al., reported an association between the presence of resistant pathogens and the frequency of lower limb amputations in patients with diabetes.16 They found that resistant Staphylococcus species were isolated in 21 percent of all patients in their cohort (38 of 181 patients) and were present in significantly higher rates among those who underwent amputations (43 percent or 18 out of 42 patients) as opposed to individuals without amputations (14 percent or 20 out of 139 patients). When comparing patients with infections caused by methicillin-susceptible S. aureus (MSSA) to those with MRSA infections, Tentolouris, et. al., noted that patients with ulcers infected by MRSA had longer healing times (a mean range of 35.4 weeks versus a mean range of 17.8 weeks in the MSSA patients).14 After the initial culture, infections caused by MRSA persisted up to four months. However, there was no difference between ulcers infected by MRSA and MSSA in terms of size, etiology or the rate of amputation. When comparing MRSA patients to those whose infections were caused by other pathogens, Wagner, et. al., reported those with MRSA infections: • responded more poorly to conservative treatment (20 percent versus 61.5 percent respectively); • had a higher rate of minor amputation (52 percent versus 30.5 percent respectively); • had a higher rate of major amputation (22 percent versus 4.5 percent respectively); and • had a higher death rate (6 percent versus 3.5 percent respectively).15 In an outpatient study, Dang, et. al., reported that, in the absence of a systemic infection, patients with infections caused by MRSA could be successfully treated in the outpatient setting.13 Despite a MRSA prevalence of 30 percent in their cohort, researchers found that the presence of MRSA did not increase the rate of hospitalization or of osteomyelitis, and antibiotics specific for MRSA were not required to successfully treat the infection.
Pertinent Points On Debridement And Minor Surgical Measures
Some type of surgical intervention is often indicated for diabetic foot infections in order to minimize tissue loss, preserve foot function and manage soft tissue infection and necrosis.17 It is an integral part of wound management and, depending on the severity of the ulceration, can range from incision and local debridement to wide area ablation of tissue and amputation. Wound debridement, which is usually the first step in treating a diabetic foot infection, involves removing necrotic tissue, exudates and metabolic waste.18 The presence of exudates is most often due to an infection by a pathogen, such as S. aureus, which can produce a fibrin-rich biofilm that makes the bacterial colony more resistant to the body’s natural immune response. Surgical debridement is a quick and effective method of removing debris and necrosis. It is highly suitable for diabetic foot ulcers, which tend to have large areas of necrotic tissue and a high propensity toward infection.19 Early debridement can minimize the bacterial load, prevent and control wound infection, accelerate the healing process and ultimately help prevent a lower limb amputation. One should repeat debridement as long as new necrotic tissue continues to form.20 Debriding an ulcer also allows for better determination of wound depth, which can be difficult due to necrotic tissue or an overlying callus. However, keep in mind that wound debridement is contraindicated in cases of ischemic or neuroischemic ulcers that are not infected.20 When it comes to ulcers that are uncomplicated by gangrene, osteomyelitis or extensive soft tissue involvement, one can often treat these ulcers successfully in an outpatient setting. In one study, 58 patients with less severe infections were treated at an outpatient clinic with oral antibiotics and surgical intervention as needed. Upon evaluation, the researchers cleaned all the wounds and performed blunt or minimal sharp debridement to remove necrotic tissue and excess callus.21 Aerobic gram-positive cocci were the sole pathogen isolated in 43 percent of cases and were present in 87 percent of the cultured wounds. Nineteen patients required minor surgical procedures, which included incision and drainage, callus trimming, nail removal and sharp debridement. Initial treatment was successful in all but five infections. In an outpatient setting, Tentolouris, et. al., reported that non-limb-threatening infections caused by MRSA could also be successfully eradicated by regular debridement, dressings, patient isolation and antimicrobial therapy.14 There were similar results from a second study in which 30 percent of the wounds were infected by MRSA.16 In the absence of a systemic infection, ulcers infected by MRSA were effectively treated outside the hospital setting with regular debridement in conjunction with other therapies. Patients with either type 1 and 2 diabetes have a high prevalence of macrovascular disease.22 Due to frequent vascular dysfunction in the lower extremities and the high-pressure distribution over ulcerated areas of the foot, infections in these patients often require other surgical interventions to promote healing. Surgery may be needed to drain deep pockets of pus, which otherwise could lead to a spread of infection. In ischemic cases, a revascularization procedure is usually indicated in order to save the foot. One should attempt to treat limb-threatening infections with conservative modalities before resorting to amputation as the latter is associated with significant morbidity and mortality. In a five-year, retrospective cohort study, Pittet, et. al., evaluated outcomes of 105 patients who were admitted for foot lesions.23 Out of these patients, 74 percent had ulcers that were complicated by contiguous osteomyelitis, deep tissue involvement and/or gangrene. Although 14 patients (13 percent) required immediate amputation, researchers implemented conservative treatment in the remainder of the cohort. This consisted of daily wound dressing, debridement, bed rest, removing pressure from the affected area and parenteral antibiotics. This approach was successful in 63 percent of the remaining 91 patients. While cultures revealed the majority of infections in this cohort were polymicrobial, S. aureus was the predominant microorganism isolated.
When More Aggressive Surgery Is Warranted
When osteomyelitis is present in deep ulcers, aggressive debridement of devitalized bone is necessary. In a retrospective study, Bodegom et. al., analyzed the results of surgical treatment of chronic osteomyelitis in the toe of 47 patients with diabetes on antibiotic therapy.24 In all cases, they removed the metatarsophalangeal joint and 37 patients (79 percent) fully recovered after primary surgery. Seven patients required a second procedure and four patients eventually underwent an amputation. Results showed that a cure rate as high as 94 percent is possible with a combination of early surgical treatment and antibiotic therapy. When infections become limb- or life-threatening, amputation is the modality of choice. Patients with diabetes have a rate of lower extremity amputation that is 15 to 46 times higher than that of the general population and about half of these procedures are performed at the level of the foot.25,26 Fejfarova, et. al., examined the role that resistant organisms, particularly MRSA, play in the incidence of amputation.16 Out of 191 patients treated at a foot clinic, 50 (26 percent) eventually underwent varying degrees of amputation. Those who had undergone amputations were more likely to have had infected ulcers caused by resistant pathogens. Researchers found resistant strains of S. aureus in 21 percent of all patients and in 43 percent of those who required amputations. Obtaining intraoperative cultures can assist in antibiotic selection or modification. While both superficial swabbing and deep-culture biopsy yield similar results, intraoperative specimens run a lower risk of contamination. Pellizzer, et. al., found that swabbing and tissue biopsy sampling were relatively equal in reliability when comparing specimens in patients with severe polymicrobial infections.27 Both are useful for monitoring antimicrobial treatment, but deep tissue cultures appeared more sensitive for monitoring resistant pathogens.
When One Should Emphasize Antibiotic Therapy
Following necessary debridement and other surgical interventions, such as bone resection and revascularization, appropriate antibiotic therapy is a cornerstone of managing diabetic foot infections. One may manage most of these infections with initial broad-spectrum antibiotic therapy and, in many cases, follow it with a more specific therapy. However, the increasing prevalence of antibiotic resistance can be a significant barrier to successfully treating these infections. Moderate-to-severe diabetic foot infections generally require hospitalization and parenteral antibiotic therapy. Since these infections are frequently polymicrobial, one should emphasize treatment that provides coverage against both gram-positive and gram-negative bacteria as well as anaerobes. Keep in mind that MRSA may be present in both polymicrobial and monomicrobial infections. The most important pathogen involved in diabetic foot infections is S. aureus, whether it is alone or part of a mixed infection.28 Given that the increasing incidence of MRSA infections is often associated with previous antibiotic therapy for treating foot ulcers, patients at risk for developing an MRSA infection should be treated with an antimicrobial agent with activity against this pathogen.
What You Should Know About Vancomycin
Vancomycin has been traditionally recommended for treating MRSA infections but it can be problematic. Its efficacy in treating patients with osteomyelitis caused by S. aureus is less than optimal and patients on vancomycin therapy have higher rates of infection recurrence compared to those treated with ceftriaxone and cefazolin.29 Vancomycin also appears to be less effective than beta-lactams in treating bone infections.30 It also must be given parenterally, thus making outpatient treatment more difficult and increasing both the expense and risk of complications. Vancomycin is associated with relatively frequent and occasionally severe adverse events. Also be aware that the incidence of vancomycin-resistant Staphylococcus aureus, while still relatively rare, is growing. A recent study suggests that S. aureus isolates that are completely resistant to vancomycin may become a major problem much sooner than anticipated.31
A Closer Look At Quinupristin/Dalfopristin
Investigators have been developing new agents with activity against gram-positive cocci, particularly against MRSA. Three new agents with demonstrated activity against MRSA are currently available. They include quinupristin/dalfopristin, linezolid and daptomycin. A fourth agent, dalbavancin, has also shown activity against several strains of gram-positive bacteria, including several resistant strains. Quinupristin/dalfopristin is the first formulation of a class of antibiotics known as the streptogramins.32 It was approved for the treatment of serious or life-threatening infections, and complicated skin and skin structure infections (cSSTIs) caused by gram-positive cocci. Like vancomycin, quinupristin/dalfopristin can only be given by intravenous infusion. Nichols, et. al., reported on the results of two studies that compared the safety, efficacy and tolerance of quinupristin/dalfopristin with that of cefazolin, oxacillin or vancomycin in the treatment of hospitalized adult patients with cSSTIs caused by gram-positive organisms.33 These two randomized, open-label trials enrolled a total of 893 patients (450 in the quinupristin/dalfopristin group, 443 in the comparator group). In both treatment groups, S. aureus was the most frequently isolated pathogen although the rate of MRSA isolates was low (2.7 percent).33 The clinical success rate was equivalent between the two treatment groups (68.2 percent for the quinupristin/dalfopristin group and 70.7 percent for the comparator group) despite a shorter mean duration of treatment for patients in the quinupristin/dalfopristin group. The by-patient and by-pathogen bacteriologic eradication rates were somewhat lower for quinupristin/dalfopristin (65.8 percent and 66.6 percent respectively) than for the comparator regimens (72.7 percent and 77.7 percent respectively). However, the researchers attributed the lower bacteriological response rates, in part, to a higher rate of polymicrobial infections and an increased number of patients classified as clinical failures. Quinupristin/dalfopristin had a higher rate of bacterial eradication in monomicrobial infections (72.6 percent) than for polymicrobial infections (63.3 percent), but the opposite was true for the comparators. Their regimen was less effective in monomicrobial infections (70.8 percent) than it was in polymicrobial infections (83.1 percent). Overall, quinupristin/dalfopristin was effective in treating cSSTIs caused by gram-positive pathogens including MRSA. Quinupristin/dalfopristin is associated with a high rate of side effects.33 While tolerance was similar, patients who were given quinupristin/dalfopristin reported a higher rate of drug-related adverse events (91.3 percent) than those in the comparator group (41.5 percent). Almost one fifth of patients in the quinupristin/dalfopristin group discontinued their treatment early, primarily due to the agent’s side effects. In other studies, drug-related arthralgia and myalgia have led to patients discontinuing quinupristin/dalfopristin therapy. Another study showed that quinupristin/dalfopristin may be more susceptible to drug resistance than either vancomycin or linezolid.34 While it was highly active against S. aureus, it had resistance rates of 2.5 percent for MRSA and 1.5 percent for MSSA, whereas vancomycin and linezolid were fully active against all organisms.
Assessing The Possible Merits Of Linezolid
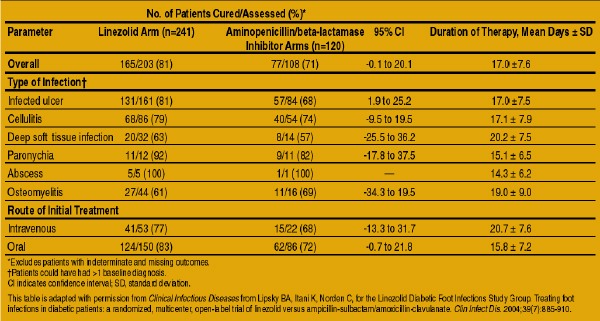
Oxazolidinones are novel synthetic compounds that have demonstrated extensive antimicrobial activity against a broad range of gram-positive bacteria, including MRSA and glycopeptide intermediate-resistant S. aureus strains.35 Linezolid is the first agent in this class and is available in both oral and parenteral formulations, making it highly suitable for outpatient therapy or as an effective switchover from intravenous to oral therapy in hospitalized patients. Data have shown that orally administered doses have 100 percent bioavailability and plasma concentrations comparable with the parenteral formulation.35 Linezolid also has achieved therapeutic concentrations in bone as well as in soft tissue.36 Initially, linezolid was approved for use in the treatment of patients with infections such as skin and soft tissue infections. Recently, it was approved by the Food and Drug Administration (FDA) for treating patients with diabetic foot infections.37 This approval was based on a study by Lipsky, et. al., that compared the safety and efficacy of parenteral and oral formulations of linezolid with intravenous ampicillin/sulbactam, and intravenous and oral amoxicillin/clavulanate.38 (See “What One Study Revealed About Linezolid” below.) A total of 371 patients were enrolled in a trial that was conducted at 45 sites in eight countries.38 Of this patient cohort, 241 received linezolid, 120 received aminopenicillin beta-lactamase inhibitors and 10 received no treatment. The most common type of infection was infected ulcers (190 linezolid, 93 comparator) followed by cellulitis (101 linezolid, 60 comparator). Researchers also saw deep soft tissue infections and osteomyelitis in the study group. In the linezolid group, 70 patients (45 percent) had infections caused by only gram-positive aerobic pathogens, 5 patients (3 percent) had mixed infections with both a gram-positive pathogen and an anaerobe, and 81 patients (52 percent) had polymicrobial infections with both gram-positive and gram-negative pathogens. Overall, clinical cure rates between the linezolid and the comparator arms were statistically equivalent (81 percent versus 71 percent respectively).38 In addition, when the researchers analyzed the findings by subgroup, patients with an infected ulcer treated with linezolid had a statistically superior response (81 percent) than those in the comparator group (68 percent). Those in the linezolid group also showed statistically higher cure rates (87 percent) than the comparator group (72 percent) among patients without osteomyelitis. Clinical cure rates among patients with monomicrobial gram-positive infections, with or without the presence of anaerobes, were 79 percent for the linezolid group (59 of 75 patients) and 73 percent for patients receiving aminopenicillin beta-lactamase inhibitors (38 of 52 patients). Parenteral treatment was of shorter duration for patients receiving linezolid whereas oral treatment was of similar length. Among patients in the linezolid group, MRSA accounted for 18 infections and 13 (72 percent) of these patients were cured.38 In the comparator group, MRSA accounted for seven infections and four of these patients were cured (57 percent). Researchers added vancomycin to the regimen in four of the seven patients and three of these patients were cured. The authors of the study did not identify resistance to linezolid by a gram-positive organism either at baseline or during treatment. Adverse events were similar for both groups (55 percent for the linezolid group versus 53 percent for the comparator group) and were generally mild to moderate and of limited duration.38 Overall, patients in the aminopenicillin/beta-lactamase inhibitor group experienced significantly fewer adverse effects (10 percent) than those using linezolid (27 percent). While rare, treatment failure has occurred because of linezolid resistance. There have been reports of vancomycin-resistant Enterococcus faecium and S. aureus, which also have demonstrated resistance to linezolid.35,39 The SENTRY Surveillance Program in the United States reported isolating eight linezolid-resistant strains among Enterococcus faecalis, E. faecium, Streptococcus epidermidis and Streptococcus oralis, with vancomycin resistance found in two of them.40 Most cases of linezolid resistance occurred with prolonged treatment courses longer than 21 days. While it is still extremely uncommon, linezolid resistance has apparently spread beyond enterococcal bacteria. However, as linezolid is thus far the only available drug in its class, cross resistance with other antibiotics will likely be a rare occurrence.35
Can Daptomycin Have An Impact?
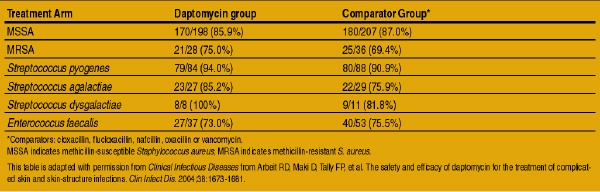
Daptomycin, a novel lipopeptide antibiotic derived from the fermentation of a strain of Streptomyces roseosporus, received FDA approval in September 2003. Like linezolid, it is the first formulation in a new class of drugs called the cyclic lipopeptides.41 One can only administer daptomycin by intravenous infusion, and, like linezolid and quinupristin/dalfopristin, the drug only exhibits antimicrobial activity against gram-positive organisms (see “Comparing Daptomycin Against Other Agents For cSSTIs” below). To date, there have been no reports of bacterial resistance. The development of resistance in clinical trials was rare as it only occurred in two of more than 1,000 patients treated with daptomycin.42 In two large clinical trials with a cohort of more than 1,000 patients with cSSTIs, researchers compared the safety and efficacy of daptomycin with penicillinase-resistant penicillins or vancomycin.43 The trial included 61 patients (11 percent) with infected ulcers in the daptomycin group and 72 (13 percent) in the comparator group. There were 40 patients with MRSA (9.3 percent) in the daptomycin group and 47 patients with MRSA (10 percent) among patients receiving comparator agents. The success rates for the clinically evaluable population were 83.4 percent for those in the daptomycin group and 84.2 percent for those in the comparator group.43 Clinical success rates for patients with infections caused by both S. aureus and hemolytic streptococci were 76 percent for those treated with daptomycin and 70 percent for patients treated with comparator drugs. In the subgroup of patients with an infected ulcer, there was a 66 percent success rate in the daptomycin group versus a 70 percent rate in the comparator group. Clinical success rates for cSSTIs caused by MRSA were 75 percent for patients receiving daptomycin and 69.4 percent for the comparator group. Safety and tolerability were similar in both arms of the trial. Only 15 participants (2.8 percent) receiving daptomycin discontinued treatment due to adverse events as did a similar number (17 patients or 2.8 percent) in the comparator group.
Dalbavancin: Does This Emerging Agent Have Promise?
Currently in development, dalbavancin is a novel intravenous semisynthetic glycopeptide that has shown activity against a wide range of gram-positive bacteria including staphylococci, streptococci, enterococci, Corynebacteria species, selected strains of vancomycin-resistant enterococci (VRE), vancomycin-intermediate S. aureus and MRSA.44-46 Although its mechanism of action is similar to that of other glycopeptides, dalbavancin has not demonstrated the same degree of cross resistance to vancomycin and appears to have activity against vancomycin-resistant van-beta phenotypic enterococci.45 A unique feature of dalbavancin is its very long half life, which results from extensive and reversible binding to plasma protein, primarily albumin.47-49 The mean plasma concentration of dalbavancin is greater than 35 mg/L for one week, following a single intravenous dose of 1 gram.47 In a randomized, controlled, open-label, phase II trial by Seltzer, et. al., the researchers randomized 62 patients with a cSSTI — suspected or known to be caused by gram-positive bacteria — to receive either a single dose of dalbavancin, two doses of dalbavancin given a week apart or a treatment with a comparator regimen.50 Researchers isolated a gram-positive organism in 41 of the patients and the majority of these were monomicrobial. S. aureus was the most frequent organism isolated, comprising 83 percent of pathogens. Clinical success rates for patients infected with MRSA were 80 percent (four of five patients) in the group that received two doses of dalbavancin; 50 percent (three of six patients) for those who received a single dose; and 50 percent (one of two patients) for the comparator regimens. In another study, researchers tested dalbavancin and selected comparators against 6,336 clinical isolates of gram-positive organisms, which included oxacillin-resistant S. aureus, VRE and penicillin-nonsusceptible pneumococci.51 The minimum inhibitory concentration (MIC) values of dalbavancin ranged from less than or equal to 0.015 g/mL to greater than 32 g/mL. However, more than 99 percent of MIC results were at less than or equal to 1 g/mL. S. aureus and coagulase-negative staphylococci were extremely susceptible to dalbavancin (the minimum concentration required to inhibit 90 percent of organisms [MIC90] was 0.06 g/mL), despite exhibiting resistance patterns to other antimicrobial agents.
Final Notes
The growing prevalence of MRSA-related infections worldwide, both among hospitalized patients and those in the community, coincides with the increasing infection rates now seen among patients with diabetes with foot ulcers. Research suggests that infections due to MRSA increase morbidity, extend hospital stay and incur higher costs and higher amputation rates. Properly diagnosing an infection, assessing its severity and determining the causative pathogens and their antibiotic susceptibilities are all critical components to successful management of these infections. When seeing at-risk patients, one should consider the possibility of MRSA when selecting initial empiric antimicrobial therapy. However, there is still a need for further studies not only to assess the growing problem of foot infections in diabetic patients that are caused by MRSA, but for developing improved strategies in dealing with this disease. Dr. Armstrong is a Professor of Surgery, Chair of Research and Assistant Dean at the William M. Scholl College of Podiatric Medicine at Rosalind Franklin University of Medicine in Chicago. He is also a member of the National Board of Directors of the American Diabetes Association. For more information on Scholl’s Center for Lower Extremity Ambulatory Research (CLEAR), check out www.rosalindfranklin.edu/scpm/clear or www.diabeticfoot.net. Editor’s Note: For related articles, see the April 2004 supplement, “Treating MRSA Infections,” or the Wound Care Q&A column, “Key Insights On Managing Infected Diabetic Ulcers,” in the September 2004 issue. One can also check out the archives at www.podiatrytoday.com.
References:
1. American Diabetes Association. Consensus Development Conference on Diabetic Foot Wound Care: 7-8 April 1999, Boston, Massachusetts. Diabetes Care. 1999;22:1354-1360.
2. Centers for Disease Control and Prevention. National Diabetes Fact Sheet. Available at: https://www.cdc.gov/diabetes/pubs/general.htm. Accessed November 26, 2003.
3. Levin ME. Management of the diabetic foot: preventing amputation. South Med J. 2002;95:10-20.
4. Holzer SE, Camerota A, Martens L, Cuerdon T, Crystal-Peters J, Zagari M. Costs and duration of care for lower extremity ulcers in patients with diabetes. Clin Ther. 1998;20:169-181.
5. Reiber GE, Boyko EJ, Smith DG. Lower extremity foot ulcers and amputations in diabetes: NIH Pub; 1995. 95-1468-1995.
6. Caputo GM, Cavanaugh PR, Ulbrecht JS, Gibbons GW, Karchmer AW. Assessment and management of foot disease in patients with diabetes. N Engl J Med. 1994;331:854-860.
7. Lipsky BA, Berendt AR. Principles and practice of antibiotic therapy of diabetic foot infections. Diabetes Metab Res Rev. 2000;16 (suppl 1):S42-S46.
8. Ramsey SD, Newton K, Blough D, et al. Incidence, outcomes, and cost of foot ulcers in patients with diabetes. Diabetes Care. 1999;22:382-387.
9. Wheat LJ, Allen SD, Henry M, et al. Diabetic foot infections. Bacteriologic analysis. Arch Intern Med. 1986;146:1935-1940.
10. El-Tahawy AT. Bacteriology of diabetic foot infections. Saudi Med J. 2000;21:344-347.
11. Lipsky BA. A current approach to diabetic foot infections. Curr Infect Dis Rep. 1999;1:253-260.
12. Baquero F. Gram-positive resistance: challenge for the development of new antibiotics. 1997:1-4.
13. Dang CN, Prasad YD, Boulton AJ, Jude EB. Methicillin-resistant Staphylococcus aureus in the diabetic foot clinic: a worsening problem. Diabet Med. 2003;20:159-161.
14. Tentolouris N, Jude EB, Smirnof I, Knowles EA, Boulton AJ. Methicillin-resistant Staphylococcus aureus: an increasing problem in a diabetic foot clinic. Diabet Med. 1999;16:767-771.
15. Wagner A, Reike H, Angelkort B. Highly resistant pathogens, especially methicillin-resistant Staphylococcus aureus, in diabetic patients with foot infections. Dtsch Med Worchenschr. 2001;126:1353-1356.
16. Fejfarova V, Jirkovska A, Skibova J, Petkov V. Pathogen resistance and other risk factors in the frequency of lower limb amputations in patients with diabetic foot syndrome. Vnitr Lek. 2002;48:302-336.
17. Mitchell DC. The role of surgery in the management of the diabetic foot. Diabetic Foot. 2003;6(Winter).
18. Singhal A, Reis ED, Kerstein MD. Options for nonsurgical debridement of necrotic wounds. Adv Skin Wound Care. 2001;14:96-103.
19. Sibbald RG, Williamson D, Orsted HL, et al. Preparing the wound bed–debridement, bacterial balance, and moisture balance. Ostomy Wound Manage. 2000;46:14-35.
20. Apelqvist J, Bakker K, van Houtum WH, Schaper NC. International consensus and practical guidelines on the management and the prevention of the diabetic foot. Diabetes Metab Res Rev. 2000;16 (suppl 1)(S84-S92).
21. Lipsky BA, Pecoraro RE, Wheat LJ. Outpatient management of uncomplicated lower-extremity infections in diabetic patients. Arch Intern Med. 1990;150:790-797.
22. Boulton AJ, Meneses P, Ennis WJ. Diabetic foot ulcers: a framework for prevention and care. Wound Rep Reg. 1999;7:7-16.
23. Pittet D, Wyssa B, Herter-Clavel C, Kursteiner K, Vaucher J, Lew PD. Outcome of diabetic foot infections treated conservatively. Arch Intern Med. 1999;159:851-856.
24. Bodegom ME, Jahrome AK, Raymakers JTF, van Baal JG. Surgical treatment of chronic osteomyelitis of the neuropathic toe–surgery. Diabetic Foot. 2004(Spring).
25. Lavery LA, Ashry HR, van Houtum WH, Pugh JA, Harkless LB, Basu S. Variation in the incidence and proportion of diabetes-related amputations in minorities. Diabetes Care. 1996;19:48-52.
26. Armstrong DG, Lavery LA, Quebedeaux TL, Walker SC. Surgical morbidity and the risk of amputation due to infected puncture wounds in diabetic versus nondiabetic adults. Southern Med J. 1997;90.
27. Pellizzer G, Strazzabosco M, Presi S, et al. Deep tissue biopsy vs. superficial swab culture monitoring in the microbiological assessment of limb-threatening diabetic foot infection. Diabet Med. 2001;18:822-827.
28. Lipsky BA, Pecoraro RE, Wheat LJ. The diabetic foot: soft tissue and bone infection. Infect Dis Clin North Am. 1990;4:409-432.
29. Tice AD, Hoaglund PA, Shoultz DA. Outcomes of osteomyelitis among patients treated with outpatient parenteral antimicrobial therapy. Am J Med. 2003;114:723-728.
30. Lipsky BA. Osteomyelitis of the foot in diabetic patients. Clin Infect Dis. 1997;25:1318-1326.
31. Howe RA, Monk A, Wootton M, Walsh TR, Enright MC. Vancomycin susceptibility within methicillin-resistant Staphylococcus aureus lineages. Emerg Infect Dis. 2004;10:855-857.
32. Synercid [package insert]. Bristol, Tenn: Monarch Pharmaceuticals, Inc; 2003.
33. Nichols RL, Graham DR, Barriere SL, et al. Treatment of hospitalized patients with complicated gram-positive skin and skin structure infections: two randomized, multicentre studies of quinupristin/dalfopristin versus cefazolin, oxacillin or vancomycin. J Antimicrob Chemother. 1999;44:263-273.
34. Millan L, Cerda P, Rubio MC, et al. In vitro activity of telithromycin, quinupristin/dalfopristin, linezolid and comparator antimicrobial agents against Staphylococcus aureus clinical isolates. J Chemother. 2004;16:230-237.
35. Raghavan M, Linden PK. Newer treatment options for skin and soft tissue infections. Drugs. 2004;64:1621-1642.
36. Lovering AM, Zhang J, Bannister GC, et al. Penetration of linezolid into bone, fat, muscle and haematoma of patients undergoing routine hip replacement. Antimicrob Chemother. 2002;50:73-77.
37. CDER New and Generic Drug Approvals. US Food and Drug Administration Web Site. Available at: https://www.fda.gov/cder/approval/index.htm. Accessed November 26, 2004.
38. Lipsky BA, Itani K, Norden C, for the Linezolid Diabetic Foot Infections Study Group. Treating foot infections in diabetic patients: a randomized, multicenter, open-label trial of linezolid versus ampicillin-sulbactam/amoxicillin-clavulanate. Clin Infect Dis. 2004;38:17-24.
39. Tsiodras S, Gold HS, Sakoulas G, et al. Linezolid resistance in a clinical isolate of Staphylococcus aureus. Lancet. 2001;358:207-208.
40. Mutnick AH, Enne V, Jones RN. SENTRY Antimicrobial Surveillance Program. Ann Pharmacother. 2001;37:769-774.
41. Tedesco KL, Rybak MJ. Daptomycin. Pharmacotherapy. 2004;24:41-57.
42. Cubicin [package insert]. Lexington, Mass: Cubist Pharmaceuticals, Inc: 2003.
43. Arbeit RD, Maki D, Tally FP, et al. The safety and efficacy of daptomycin for the treatment of complicated skin and skin-structure infections. Clin Infect Dis. 2004;38:1673-1681.
44. Candiani G, Abbondi M, Borgonovi M, Romanò G, Parenti F. In-vitro and in-vivo antibacterial activity of BI 397, a new semi-synthetic glycopeptide antibiotic. J Antimicrob Chemother. 1999;44:179-192.
45. Jones RN, Biedenbach DJ, Johnson DM, Pfaller MA. In vitro evaluation of BI 397, a novel glycopeptide antimicrobial agent. J Chemother. 2001;13:244-254.
46. Goldstein EJC, Citron DM, Merriam CV, Warren Y, Tyrrell K, Fernandez HT. In vitro activities of dalbavancin and nine comparator agents against gram-positive species and Corynebacteria. Antimicrob Agents Chemother. 2003;47:1968-1971.
47. Leighton A, Mrosczcak E, White R, et al. Dalbavancin: phase I single and multiple-dose placebo controlled intravenous safety, pharmacokinetic study in health volunteers. Paper presented at: 41st Interscience Conference on Antimicrobial Agents and Chemotherapy, 2001; Chicago, Ill.
48. Dorr MB, Henkel T, Dowell J, Stogniew M. Rationale for once weekly dosing of dalbavancin, a new semisynthetic glycopeptide. Paper presented at: 40th Annual Meeting of the Infectious Diseases Society of America, 2002; Chicago, Ill.
49. Dowell JA, Gottlieb AB, van Saders C, et al. The pharmacokinetics and renal excretion of dalbavancin in healthy subjects. Paper presented at: 42nd Interscience Conference on Antimicrobial Agents and Chemotherapy, 2002; San Diego, Calif.
50. Seltzer E, Dorr MB, Goldstein BP, et al. Once-weekly dalbavancin versus standard-of-care antimicrobial regimens for treatment of skin and soft-tissue infections. Clin Infect Dis. 2003;37:1298-1303.
51. Streit JM, Fritsche TR, Sader HS, Jones RN. Worldwide assessment of dalbavancin activity and spectrum against over 6,000 clinical isolates. Diagn Microbiol Infect Dis. 2004;48:137-143.



{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}