

Exploring The Potential Of Growth Factors In Chronic Wounds
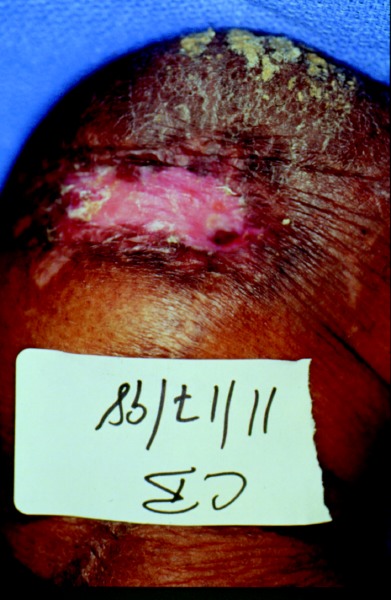
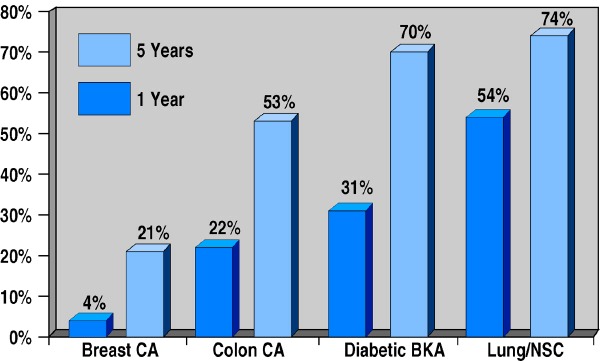
Do growth factors improve the rate of wound healing? When is it appropriate to use them on chronic wounds? Is the cost of growth factor modalities worth the results? Our expert panelists answer these key questions, share their experiences and ponder the future of these modalities with their discussion about the efficacy of growth factors in chronic wound care. Without further delay, here is what they had to say … Q: When, why and how do you utilize growth factors in the treatment of foot and ankle wounds? A: Wound bed preparation is the first step in approaching all wounds, notes Thomas E. Serena, MD, FACS. This includes primary and serial debridement, ensuring proper moisture balance and reducing bacterial burden. Jason Weber, DPM, concurs, emphasizing that one may employ growth factors in conjunction with proper wound care, including frequent debridement. Quoting a 1996 study by Steed, Dr. Weber says “wound debridement is a vital adjunct in the care of … diabetic foot ulcers.” Barry Rosenblum, DPM, and Susan G. Woods, MD, say they consider using growth factors in non-infected foot and ankle wounds when they have failed to heal in a reasonable period of time and other variables (such as arterial blood supply, debridement and offloading) are at optimal levels. Growth factors are an important part of the wound healing phases and Dr. Woods notes platelet-derived growth factor (PDGF) is one of the earliest growth factors to be identified in the process by researchers. “Growth factors help stimulate fibroblasts to make collagen, angiogenesis and chemotaxis, which is especially important in the proliferative phase of wound healing,” explains Dr. Woods. PDGF, a topical gel (Regranex, Johnson and Johnson) which one applies directly to the wound, is the only growth factor approved by the FDA for diabetic ulcers, notes Dr. Woods. She adds that studies have found the combination of ulcer debridement and PDGF has a synergistic effect on healing. Recently, Lawrence G. Karlock, DPM, says he has been utilizing topical growth factors “in an earlier period” than he traditionally used them in the last decade. While he notes an initial reluctance to use this modality due to cost concerns, Dr. Karlock says he has been “pleasantly surprised” that these topical growth factors can actually “kickstart a chronic wound into epithelialization.” If a patient presents with an uninfected granulating wound, Dr. Serena says he may use PDGF on the first visit. Dr. Karlock does not employ topical growth factors initially for any acute wounds. However, Dr. Serena has found that in treating acute wounds in healthy patients, PDGF worked best when applied every other day. He cautions against extrapolating this timetable into chronic wound care. Q: Are there any new theories or science about the role of PDGF in wound care? Specifically, how long does it take for PDGF to work in the wound? A: In theory, PDGF should work on all chronic wounds, posits Dr. Woods. However, she notes that science has shown the success of PDGF in the diabetic wound is due to the “persistence of biological activity of this peptide in the wound microenvironment. “The microenvironment of these chronic wounds can be very hostile to proteins and breakdown of PDGF by proteases is likely,” explains Dr. Woods. “Therefore, discovering an optimal delivery system is key to the success of PDGF.” When it comes to healing chronic foot and ankle wounds, Dr. Rosenblum says he also considers bioengineered skin as “a delivery system of a variety of growth factors as opposed to applying a single growth factor.” In his experience, Dr. Rosenblum has found that if PDGF is effective, one will see results within 12 to 20 weeks. He points out this is the same healing time one would see with living skin equivalents or bioengineered skin. While studies measuring wound healing are challenging due to many variables, Dr. Woods cites two noteworthy studies in regard to PDGF. In the study by Steed, et. al., 48 percent of the patients achieved healing in 20 weeks. Dr. Woods also cites a larger study by Wieman, et. al., which showed that PDGF decreased the time to complete healing by 32 percent (86 days versus 127 days). The adjunctive combination of PDGF and vacuum-assisted closure (VAC therapy, KCI) has been intriguing, according to Dr. Serena. He says they apply PDGF in a thin layer, wait five minutes for the PDGF to “saturate receptors” and then apply VAC therapy. Dr. Serena says he is frequently asked if the VAC vacuums out the PDGF. This is no longer an issue five minutes after one has applied PDGF, counters Dr. Serena. He says the biologic agent stimulates receptors and initiates a cascade of cellular events that lead to cell stimulation and proliferation. “This mechanism of action suggests that the wound only needs to be exposed to PDGF briefly to exert PDGF’s full effect,” explains Dr. Serena. “As a result, we have broadened our use of PDGF, particularly in combination with other wound care products.” However, Dr. Rosenblum says he cautions patients that there is no magic bullet and emphasizes the importance of patient compliance. “Failure to comply with explicit instructions to remain completely offloaded will predictably result in failure, which, in turn, would never justify the costs associated with application of topical growth factor therapy,” maintains Dr. Rosenblum. Q: Do the results of these growth factor products justify the costs? A: All the panelists believe the costs are justified. Dr. Serena suggests most would say chemotherapy for colon and breast cancer patients justifies the costs. He notes the one- and five-year mortality rates of diabetic patients who undergo a below-the-knee amputation (BKA) are higher than the mortality rates of patients with breast or colon carcinoma (see chart above). “PDGF is ‘chemotherapy’ for the diabetic foot,” says Dr. Serena. “The cost of PDGF in limb preservation in the diabetic patient is not only justified but it seems unconscionable not to use these agents when the patient’s survival is in jeopardy.” Dr. Woods says the cost is justified with appropriate patient selection. When patients with diabetes have a debrided and uninfected foot or ankle wound, and adequate peripheral circulation, they should have a reasonable result, according to Dr. Woods. Dr. Weber points out that multiple studies have proven the efficacy of PDGF in treating diabetic foot ulcers. “PDGF has been shown to increase the incidence of complete healing as well as the healing rate of diabetic foot ulcers,” explains Dr. Weber. Although it may cost more in the short run to heal a chronic wound more quickly, Dr. Rosenblum believes the short-term costs may be justified by the results of growth factors and the earlier return to work and reduced risk of infection since the wound heals faster. He says the costs are also justified by the decreased requirements for surgical intervention and prolonged dressing care along with the decreased costs associated with manpower. Dr. Karlock concurs and notes that he has had success using Dermagraft (Smith and Nephew) and Apligraf (Organogenesis) to close wounds. Q: What new growth factors do you see on the horizon for possible use in wound care? A: Dr. Woods believes growth factors that stimulate keratinocytes and the epithelium will also have a future in wound healing. “Whereas PDGF stimulates fibroblasts, which lay down a collagen matrix, other growth factors such as epidermal growth factor (EGF) and GMCSF could work in conjunction to lay down the epithelium that covers the collagen,” explains Dr. Woods. According to Dr. Rosenblum, there has been some promising work with basic fibroblast growth factor (bFGF), the aforementioned EGF and transforming growth factor beta (TGF-beta). Dr. Weber concurs. He notes that researchers have shown EGF enhances the healing of diabetic foot ulcers and TGF-beta promotes wound healing. The FGF family, which contains at least 23 members, is known to regulate angiogenesis, cell growth, cell migration, neurotrophic effects and other aspects of tissue repair, according to Dr. Weber. Dr. Weber says other potentially promising growth factors include: vascular endothelial growth factor (VEGF), which induces angiogenesis and endothelial cell proliferation; tumor necrosis factor (TNF), which stimulates fibroblasts and promotes angiogenesis; keratinocyte growth factor-2 (KGF-2), which has been studied in chronic venous ulcers; and insulin growth factor (IGF), which is known to promote tissue growth. All of the panelists would like to see more studies on combination therapy with growth factors. Dr. Weber is an Associate of the American College of Foot and Ankle Surgeons. He is an Attending Podiatric Surgeon at Washington Hospital Center in Washington, D.C. Dr. Rosenblum is an Assistant Clinical Professor of Surgery at Harvard Medical School and is the Director of Podiatric Residency Training at the Beth Israel Deaconess Medical Center in Boston. Dr. Serena is the founder and Medical Director of the Penn North Centers for Advanced Wound Care, NewBridge Medical Research and Oxygen-8 Hyperbaric Centers in western Pennsylvania and southern New York. Dr. Serena is also a Professor at Gannon University and serves on the board of the Wound Healing Society. Dr. Woods is a Fellow of the American Academy of Dermatology and practices in Austintown, Ohio. She is the founder of the Wound Clinic at Forum Health in Youngstown, Ohio. Dr. Karlock is a Fellow of the American College of Foot and Ankle Surgeons, and practices in Austintown, Ohio. He is a member of the Editorial Advisory Board for WOUNDS, a Compendium of Clinical Research and Practice.



{kind=link}
{kind=link}
{kind=link}