

The Power of Collateral Circulation: A Case of Asymptomatic Chronic Total Occlusion of the Left Main Coronary Artery
ABSTRACT: Total occlusion of the left main coronary artery predominantly presents with recurrent angina or myocardial infarction. Long-term survival and myocardial function depends on the well-developed right to left collaterals. We report a case of a 46-year-old man who was referred because of incidental finding of low ejection fraction during work-up for syncope 5 months prior. The patient denied any recurrence or any other symptom after that episode and claimed an unchanged exercise capacity. He had hypertension, hyperlipidemia, and history of 15-pack/year smoking. Except for class II morbid obesity, he had completely normal vital signs, physical examination, and lab tests on admission. The echocardiogram was suggestive of previous anterior wall myocardial infarction and demonstrated a low left ventricle ejection fraction with diffuse hypokinesis of the left ventricle. The patient underwent cardiac catheterization, which revealed total occlusion of the left main coronary artery, dominant right coronary artery with a 95% stenosis in the proximal segment, and collaterals from the right to the left coronary arteries. The patient was immediately referred for coronary artery bypass surgery.
This case demonstrates the power of collateral circulation in protecting the patient from symptoms and death despite total occlusion of the left main coronary artery and severe stenosis of the proximal right coronary artery.
J INVASIVE CARDIOL 2012;24(9):E196-E198
Key words: coronary artery disease, left main coronary disease, total occlusions, diagnostic cardiac catheterization
_____________________________________________________
The exact prevalence of total occlusion of the left main coronary artery is unknown. Different studies have shown a frequency between 0.04% to 0.1%.1,2 The predominant presentation of these patients is usually either recurrent angina or myocardial infarction (MI)3 and the patients long-term survival and myocardial function depends on the well-developed right to left collateral.4,5
This case demonstrate the power of the coronary arteries collateral circulation in protecting the patient from symptoms and death, despite total occlusion of the left main coronary artery and severe stenosis of the proximal right coronary artery (RCA).
 Case Report. A 46-year-old man was referred by his primary care physician to the cardiology clinic because of incidental finding of low ejection fraction (25% to 35%) on echocardiogram during work up for syncope, which occurred 5 months prior. On the day of the syncopal event, the patient felt lightheaded, diaphoretic, and lost consciousness for 5 minutes. Since the syncope event, the patient has had no recurrence and denied any further medical symptoms. A cardiac catheterization was performed for coronary evaluation.
Case Report. A 46-year-old man was referred by his primary care physician to the cardiology clinic because of incidental finding of low ejection fraction (25% to 35%) on echocardiogram during work up for syncope, which occurred 5 months prior. On the day of the syncopal event, the patient felt lightheaded, diaphoretic, and lost consciousness for 5 minutes. Since the syncope event, the patient has had no recurrence and denied any further medical symptoms. A cardiac catheterization was performed for coronary evaluation.
The patient did not have any history of shortness of breath on exertion, chest pain, orthopnea, or paroxysmal nocturnal dyspnea. His exercise capacity had not changed for the last 6 months and was about 10 blocks without any symptoms. He had hypertension, hyperlipidemia, and history of 15-pack/year smoking. He had no history of diabetes and no family history of coronary artery disease. The patient was not on any medications prior to the event.
His body mass index was 36.6 kg/m2 (morbid obesity class II), blood pressure was 110/80, pulse rate was 70 and regular, and the pulse oxymeter showed 100% on room air. Physical examination showed no jugular venous distention. The heart and lung examination did not reveal any abnormality. There was no hepatomegaly or peripheral edema.
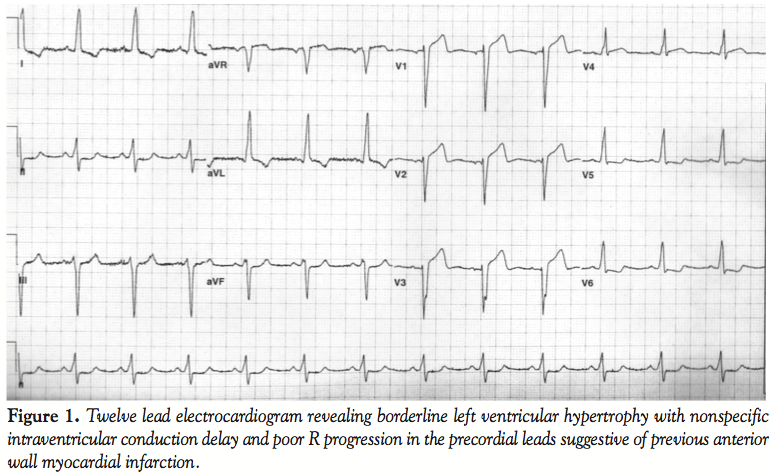
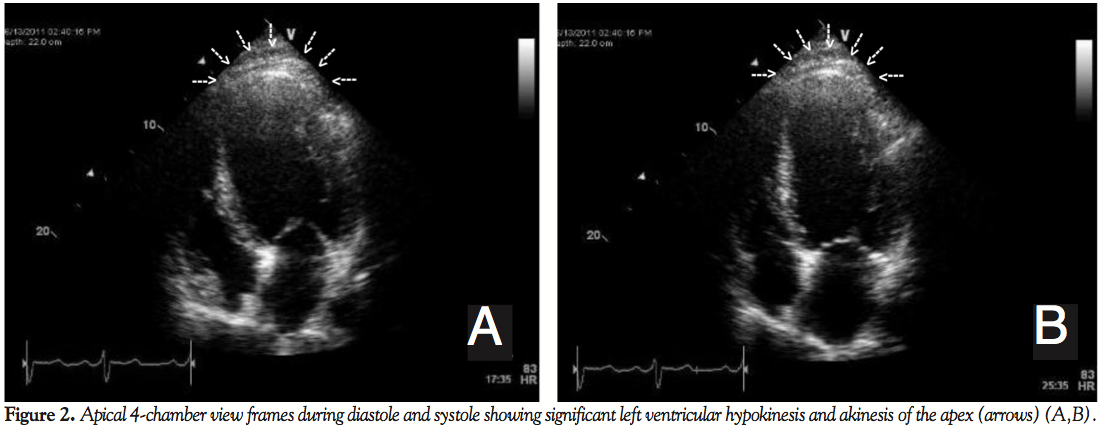 The patient’s laboratory results revealed a hemoglobin value of 13.4 gm/dL. The ECG shows normal sinus rhythm, left axis deviation, borderline left ventricular hypertrophy with nonspecific intraventricular conduction delay, and poor R progression in the precordial leads, suggestive of previous anterior wall MI (Figure 1). The echocardiogram (Figures 2A and 2B, Videos 2A-2C) demonstrated a severely depressed left ventricle ejection fraction of 25%-35% with diffuse hypokinesis of the left ventricle mild segmental wall motion abnormalities, and akinesis of the apex. There was no significant valvular pathology identified.
The patient’s laboratory results revealed a hemoglobin value of 13.4 gm/dL. The ECG shows normal sinus rhythm, left axis deviation, borderline left ventricular hypertrophy with nonspecific intraventricular conduction delay, and poor R progression in the precordial leads, suggestive of previous anterior wall MI (Figure 1). The echocardiogram (Figures 2A and 2B, Videos 2A-2C) demonstrated a severely depressed left ventricle ejection fraction of 25%-35% with diffuse hypokinesis of the left ventricle mild segmental wall motion abnormalities, and akinesis of the apex. There was no significant valvular pathology identified.
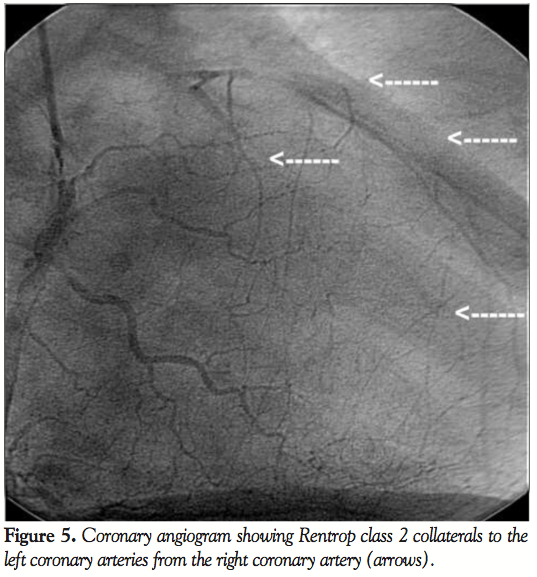
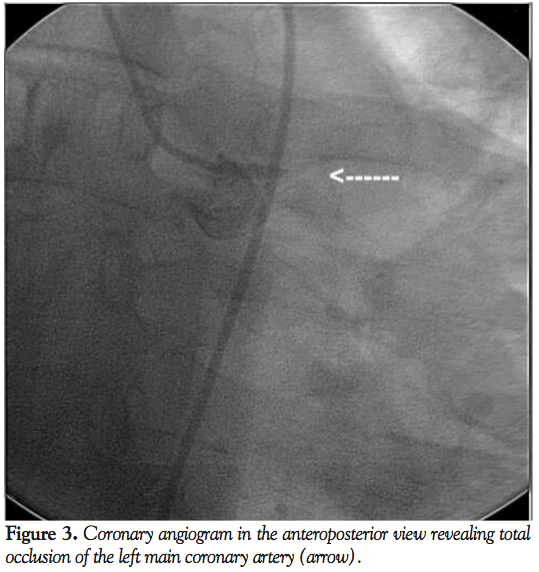 The cardiac catheterization revealed total occlusion of the left main coronary artery (Figure 3, Video 3A) and a dominant RCA with a 95% stenosis in the proximal segment (Figure 4, Video 4A). There were Rentrop class 2 collaterals from the right to the left coronary arteries (Figure 5, Video 5A).
The cardiac catheterization revealed total occlusion of the left main coronary artery (Figure 3, Video 3A) and a dominant RCA with a 95% stenosis in the proximal segment (Figure 4, Video 4A). There were Rentrop class 2 collaterals from the right to the left coronary arteries (Figure 5, Video 5A).
The patient was immediately referred for coronary artery bypass surgery (CABG) and was successfully bypassed with a left internal mammary artery to left anterior descending, saphenous vein graft to first obtuse marginal, and saphenous vein graft to right posterior descending.
 An automatic implanted cardioverter defibrillator was placed due to an in-hospital episode of ventricular fibrillation cardiac arrest, which was promptly treated by defibrillation to normal sinus rhythm. He recovered without further events and no neurological injury was noted on discharge.
An automatic implanted cardioverter defibrillator was placed due to an in-hospital episode of ventricular fibrillation cardiac arrest, which was promptly treated by defibrillation to normal sinus rhythm. He recovered without further events and no neurological injury was noted on discharge.
One month after CABG, the patient remained asymptomatic without any further episodes of ventricular arrhythmias. However an improvement of the left ventricular ejection fraction was not yet appreciated on the first follow-up echocardiogram.
 Discussion. Review of the literature indicates a frequency of 0.04% to 0.1% of chronic total occlusion of the left main coronary artery (LMCA) on cardiac catheterization.1-3 Most patients with acute or subacute occlusion of the LMCA have a high mortality, thus finding a chronic totally occluded LMCA is rare and survival depends on the size and dominance of the RCA and the formation of collateral supply to the left coronary system.2,6,7 The degree of collateral supply likely influences the amount of symptoms, which the patients experience. One study suggested that collateral circulation can prevent ischemia and preserve ventricular function, but collateral circulation does not appear to protect against exercise induced ischemia.4,5 It has also been observed that in patients with significant right to left collaterals, undergoing coronary bypass grafting does decrease symptoms and improve survival.5 RCA disease in these situations is variable. A review of published reports showed that 20 out of 40 patients had more than 50% stenosis of RCA.8 As CABG is the treatment of choice in left main disease, visualization of the distal left coronary arteries and decision regarding the possibility and placement of grafts are pivotal.9
Discussion. Review of the literature indicates a frequency of 0.04% to 0.1% of chronic total occlusion of the left main coronary artery (LMCA) on cardiac catheterization.1-3 Most patients with acute or subacute occlusion of the LMCA have a high mortality, thus finding a chronic totally occluded LMCA is rare and survival depends on the size and dominance of the RCA and the formation of collateral supply to the left coronary system.2,6,7 The degree of collateral supply likely influences the amount of symptoms, which the patients experience. One study suggested that collateral circulation can prevent ischemia and preserve ventricular function, but collateral circulation does not appear to protect against exercise induced ischemia.4,5 It has also been observed that in patients with significant right to left collaterals, undergoing coronary bypass grafting does decrease symptoms and improve survival.5 RCA disease in these situations is variable. A review of published reports showed that 20 out of 40 patients had more than 50% stenosis of RCA.8 As CABG is the treatment of choice in left main disease, visualization of the distal left coronary arteries and decision regarding the possibility and placement of grafts are pivotal.9
A rare finding of chronic total occlusion of the left main coronary artery and severe right coronary disease (95% stenosis) in our patient with no angina or angina equivalent symptoms is likely due to extensive right to left collaterals and adjustment of his lifestyle. This patient had significant wall motion abnormalities noted on transthoracic echocardiography. This finding is highly specific for underlying coronary disease, yet not very sensitive.10 Performing coronary angiography is mandatory for this reason.
Conclusion
This case emphasizes the importance of the coronary collateral supply in symptom freedom and survival of a patient with total occlusion of the left main coronary artery.
References
- Ward DE, Valantine H, Hui W. Occluded left main stem coronary artery. Report of five patients and review of published reports. Br Heart J. 1983;49(3):276-279.
- Greenspan M, Iskandrian AS, Segal BL, Kimbiris D, Bemis CE. Complete occlusion of the left main coronary artery. Am Heart J. 1979;98(1):83-86.
- Kanjwal MY, Carlson DE Jr, Schwartz JS. Chronic/subacute total occlusion of the left main coronary artery--a case report and review of literature. Angiology. 1999;50(11):937-945.
- Ha JW, Cho SY, Jang YS, Chung N, Shim WH, Kim SS. Collateral circulation in total occlusion of the left anterior descending or right coronary artery. Yonsei Med J. 1994;35(2):132-141.
- Slunga L, Eriksson P, Osterman G. Complete occlusion of the left main coronary artery: clinical and angiographic observations in five cases. J Intern Med. 1989;225(2):123-127.
- Sugishita K, Shimizu T, Kinugawa K, et al. Chronic total occlusion of the left main coronary artery. Intern Med. 1997;36(7):471-478.
- Valle M, Virtanen K, Hekali P, Frick MH. Survival with total occlusion of the left main coronary artery. Significance of the collateral circulation. Cathet Cardiovasc Diagn. 1979;5(3):269-275.
- Zimmern SH, Rogers WJ, Bream PR, et al. Total occlusion of left main artery: the Coronary Artery Surgery Study (CASS) experience. Am J Cardiol. 1982;49(8):2003-2010.
- Crosby IK, Wellons HA Jr, Bruwell L. Total occlusion of left main coronary artery. Incidence and management. J Thorac Cardiovasc Surg. 1979;77(3):389-391.
- ACC/AHA guidelines for the clinical application of echocardiography. A report of the American College of Cardiology/American Heart Association Task Force on Assessment of Diagnostic and Therapeutic Cardiovascular Procedures (Subcommittee to Develop Guidelines for the Clinical Application of Echocardiography). Circulation. 1990;82(6):2323-2345.
_____________________________________________________
From the 1Division of Cardiology, Department of Medicine, Brookdale University Hospital and Medical Center and the 2Department of Medicine, State University of New York-Downstate Medical Center, Brooklyn, New York.
Disclosure: The authors have completed and returned the ICMJE Form for Disclosure of Potential Conflicts of Interest. The authors report no conflicts of interest regarding the content herein.
Manuscript submitted March 22, 2012 and accepted April 14, 2012.
Address for correspondence: Ricardo Castillo, MD, FACC, Assistant professor of Medicine, SUNY-Downstate Medical Center, Associate Director of the Cardiac catheterization laboratory, Brookdale University Hospital and Medical Center, One Brookdale Plaza, Brooklyn, NY 11212, USA. E-mail: ric_castillo@hotmail.com



