

ADVERTISEMENT
Orbital Atherectomy: Device Evolution and Clinical Data
Abstract: A number of atherectomy devices were developed in the last few years. Among them, the DiamondBack 360° Peripheral Orbital Atherectomy System (Cardiovascular Systems, Inc) was specifically designed to work in severely calcified plaque. This article reviews the history, mechanism of action, evolution, clinical data, and future applications of this particular atherectomy device.
J INVASIVE CARDIOL 2014;26(5):215-219
____________________________
The endovascular treatment of lower-extremity peripheral arterial disease (PAD) has rapidly evolved in the last decade. The initial approach was extrapolated from the coronary field and involved plain old balloon angioplasty (POBA) alone. Despite its excellent immediate technical success, POBA was limited by its high mid- and long-term failure rates due to inadequate luminal gain and accelerated restenosis rates.1,2 The advent of stenting technology decreased later lumen loss and provided more durable results compared to POBA.3,4 However, stents in the peripheral circulation have also been predisposed to unique challenges, including fracture and neointimal hyperplasia.5
Calcified plaques with significant luminal narrowing remain among the most difficult lesions for percutaneous interventions in either the coronary or peripheral vessels. In human atherosclerotic plaque, calcium precipitation develops a complete skeletal architecture, histologically indistinguishable from trabecular bone.6 This process of “skeletonization” is initially developed through an active process of endochondrial ossification and progresses finally to mature lamellar bone formation,7 leading to lesions that are stiff, non-compliant, and difficult to dilate. As a result, angioplasty of calcified lesions carries an increased risk of dissection, perforation, or inadequate stent expansion.8 As the primary goal of POBA with or without stenting is to achieve lumen enlargement, it follows that these techniques may be suboptimal as stand-alone therapy in calcified vessels without adequate lesion preparation.
In this regard, various endovascular technologies have been developed to improve the safety and efficacy of revascularization of calcified plaques that lead to symptomatic PAD.5 Among them, a number of plaque-modification modalities were introduced with the postulated benefit of reducing the total atheroma burden, changing the arterial compliance, and lessening vessel wall trauma. One such atherectomy device, the DiamondBack 360°Peripheral Orbital Atherectomy System (OAS; Cardiovascular Systems, Inc), was specifically designed to modify the surface of calcified plaque while preserving the more elastic arterial wall. This differential sanding property could in turn lead to a more favorable result with POBA, as further plaque fracture and luminal enlargement can now be achieved using very low balloon inflation pressure, which will in turn minimize injury to the vessel wall. Lesion pretreatment with the OAS has translated into a decreased need for bail-out stenting,9 which preserves the opportunity for future revascularization treatments, especially with some of the promising new local drug therapies. Herein, this article reviews the history, evolution, clinical data, and future applications of this particular atherectomy device.
Engineering of the DiamondBack 360° Peripheral Orbital Atherectomy System
Over the years, the OAS went through a series of design stages that were predicated on the need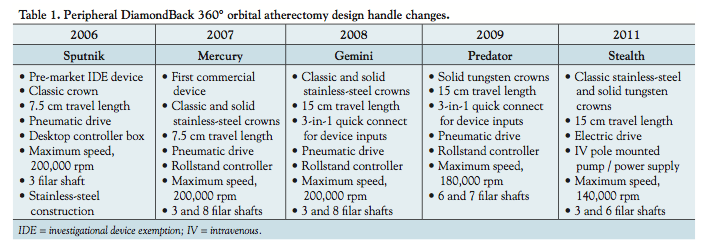 to develop a product that was easy to use, reliable, and safe (Table 1). These design changes went through several iterations based upon findings from clinical data, with the goal of determining the optimal treatment algorithm for calcified lesions.
to develop a product that was easy to use, reliable, and safe (Table 1). These design changes went through several iterations based upon findings from clinical data, with the goal of determining the optimal treatment algorithm for calcified lesions.
Sputnik Handle. The initial design of the OAS included a stainless-steel, machined metal handle (the Sputnik Handle) and the eccentrically-placed classic crown with its narrow strip of 30 micron diamond coating. A pneumatic turbine provided the power to rotate the abrasive crown at speeds of up to 200,000 rpm. A simple pneumatic control system with limited feedback was used to regulate air supply to the handle turbine.
Mercury Handle. After the United States Food and Drug Administration (FDA) approved its use in the peripheral arteries in 2007, the OAS was redesigned. The remodeled product initially affected the design handle, by introducing the Mercury Handle, but kept the same classic crown with its 30 micron diamond coating. This Mercury Handle design maintained the same functionality as the Sputnik, but improved manufacturability. An integrated control feedback system was implemented to automatically monitor and adjust the speed of the pneumatic turbine. The Upright Controller console was also enhanced to provide speed and treatment interval information.
Later on, a different crown type, the solid crown, was introduced into the armamentarium. The solid crown was characterized by the same diamond coating, but covered a much broader surface area, thus allowing for greater plaque-crown interface. Furthermore, by increasing the mass of this particular crown type, the radial force was increased, thus improving the lesion-sanding efficiency. Alongside the introduction of the solid crown, the helically-wound wire Drive Shaft that drove the crown rotation was also changed to improve torque transmission.
From a clinical standpoint, during these preliminary engineering changes, there were few trial data available at that time to guide operators regarding individual OAS run time and total treatment duration. The common practice was to treat the lesions for longer run times with the belief that longer individual and total OAS treatment times would result in larger luminal diameter.
Gemini Handle. The third iteration of the control handle, the Gemini Handle, was developed to treat longer lesions without the need for device repositioning. This was accomplished by simply increasing the control knob travel length from 7.5 cm to 15 cm. The Gemini Handle also incorporated a single air, saline, fiberoptic connector that significantly reduced saline handle leakage.
The crowns used with the Gemini Handle also underwent further revisions. A Predator tungsten solid crown with a 30 micron diamond coating was created. As tungsten was heavier than the traditional material, it increased sanding efficiency so that the device speed could be reduced. This was considered an important development in light of a few case reports alluding to hemolysis related to device usage. Hemolysis was conjectured to be the result of higher device spin rates. In an attempt to further enhance luminal gain and sanding capability, especially in lesions with softer plaque morphology, a model of the Gemini Handle with a 70 micron diamond coating on the crown was also developed. In the endovascular laboratories, however, the improved sanding efficiency came with the cost of increased procedural complications, specifically slow flow. The slow flow was not thought to be related to increased particulate size, but rather to the absolute increase in the volume of particles. This was based upon extensive porcine, cadaver, and carbon block testing demonstrating that there was no statistically significant difference in the resulting particulate size.
Stealth Handle. The fourth and latest iteration of the OAS is the Stealth Electric Handle (Figure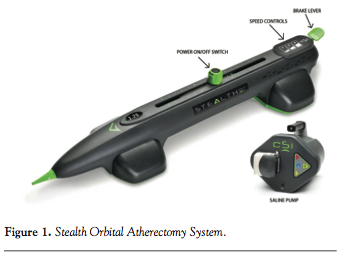 1). The development of this handle was motivated by physician feedback indicating that a faster, easier, and more efficient system was needed. The goals with this particular design were to eliminate the expensive capital equipment, reduce overall procedure time, and provide physicians with all device controls integrated into the handle, while maintaining the current mechanism of action and crown configuration that demonstrated the clinical safety of the previous designs.
1). The development of this handle was motivated by physician feedback indicating that a faster, easier, and more efficient system was needed. The goals with this particular design were to eliminate the expensive capital equipment, reduce overall procedure time, and provide physicians with all device controls integrated into the handle, while maintaining the current mechanism of action and crown configuration that demonstrated the clinical safety of the previous designs.
A number of specific product improvements were implemented to achieve these goals. The electric drive system eliminated the need for compressed air and a large pneumatic controller. This significantly decreased the amount of time needed to set up the equipment and improved ease of use in the catheterization laboratory. A device start and stop button, control knob with spin control, and speed setting selector were all incorporated onto the handle, thus eliminating the need for the foot pedal to activate the device and the need for a second person to simultaneously operate the Upright Controller outside the sterile field. The lower-profile micro crown was also added and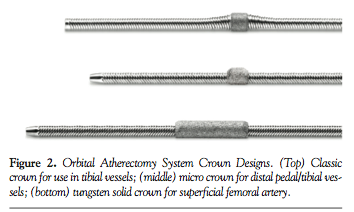 allowed increased flexibility through tortuous vessels and tight bends in the tibial vessels (Figure 2).
allowed increased flexibility through tortuous vessels and tight bends in the tibial vessels (Figure 2).
Clinical data evaluating the safety and efficacy of the DiamondBack 360° Peripheral OAS. The primary data regarding the safety and efficacy of the OAS for treating peripheral lesions in all lower-extremity arterial beds derive from analysis of both single- and multicenter registries and randomized clinical trials (Table 2).
The initial clinical experience with the Orbital Atherectomy System (PAD I) was completed by Zeller et al in 2004. The technical success rate (including postdilatation) was achieved in 94% of the patients (16/17) and in 92% of the lesions (22/24). In the successful cases, the average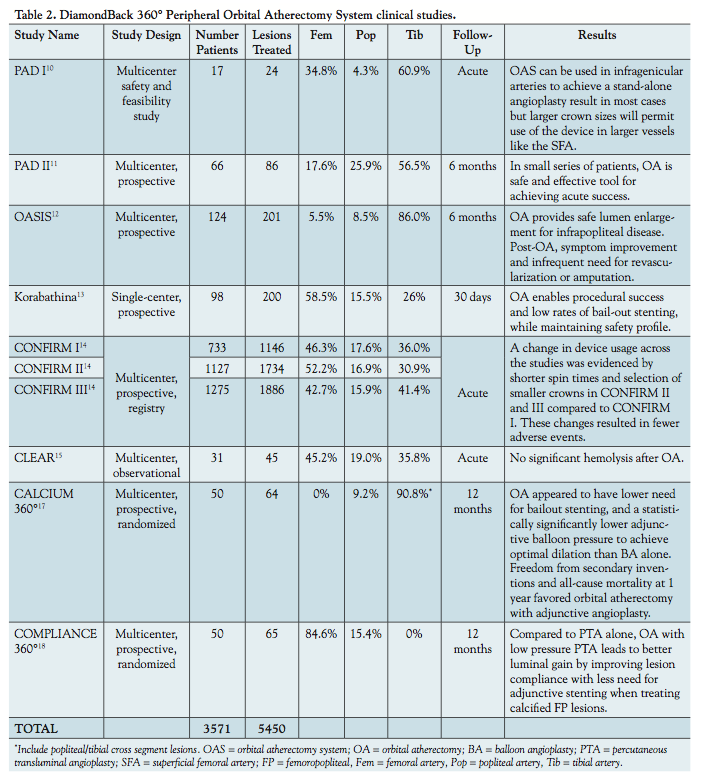 percent stenosis was reduced from 86% to 44% following OAS and then to 6% after adjunctive therapy.10
percent stenosis was reduced from 86% to 44% following OAS and then to 6% after adjunctive therapy.10
The Study of the Orbital Atherectomy System for the Treatment of Peripheral Vascular Disease (PAD II) was conducted in Europe in subjects with infrapopliteal disease treated with the OAS. Procedural success, defined as <30% residual stenosis post OAS and any adjunctive treatment, was achieved in 91% of the 66 cases. There were 4 device-related serious adverse events by 30 days post procedure, and the target lesion revascularization (TLR) rate at 6 months was 13.6%. The results of PAD II formed the impetus for the larger OASIS (Orbital Atherectomy System for the Treatment of Peripheral Vascular Stenosis) trial.11
The OASIS study was a prospective, non-randomized multicenter registry conducted from 2006 to 2007 at 17 sites in the United States.12 Data from this study fulfilled the FDA requirements for product clearance in 2007. The objective of this study was to evaluate 30-day and 6-month outcomes after orbital atherectomy (OA). On average, subjects were 70 years old and about two-thirds were male. Sixty-eight percent of patients (n = 84) had claudication (Rutherford class 1-3), and 32% (n = 40) had critical limb ischemia (CLI) with ischemic rest pain or non-healing ulcers (Rutherford class 4 and 5, respectively). OA was performed on 201 infrapopliteal lesions (55% calcified) altogether. Procedural success was achieved in 90.1% of lesions (n = 188) with a final diameter stenosis (primary efficacy endpoint) of 17.8 ± 13.5%. The mean ankle-brachial index (ABI) increased significantly from 0.68 ± 0.20 at baseline to 0.82 ± 0.10 at 6 months (P<.001). In terms of 30-day major adverse events (MAE), these occurred in a total of 4 patients (3.2%), including death (n = 2), myocardial infarction (n = 1), and TLR (n = 1). The 2 deaths and the MI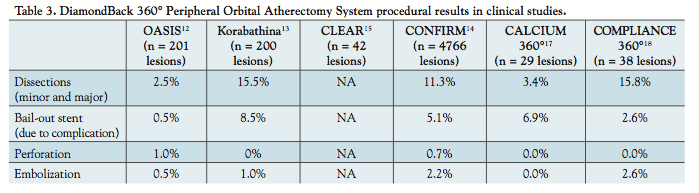 were not related to the procedure. At 6-month follow-up, cumulative MAEs occurred in 13 patients (10.4%), including death (n = 3), planned minor amputation (n = 3), and target vessel revascularization (n = 7) (Table 3).
were not related to the procedure. At 6-month follow-up, cumulative MAEs occurred in 13 patients (10.4%), including death (n = 3), planned minor amputation (n = 3), and target vessel revascularization (n = 7) (Table 3).
The results from the OASIS study established the safety and efficacy of OA for the treatment of infrapopliteal disease, setting the stage for the use of the device in the femoropopliteal tree. Once approved by the FDA, the OAS was widely adopted by the endovascular community and even more data became available, mostly from single-center reports.13
The largest of such reports was from Korabathina et al,13 who reported an experience treating 200 peripheral lesions with the OAS at a single center. Lesion lengths ranged from 15 mm to 300 mm, and approximately one-third of the lesions were total occlusions, with calcification present in 77.5%. This report extended the efficacy data from the OASIS trial to femoral and popliteal lesions, as a residual stenosis of <30% post OA with or without adjunctive therapy was achieved in 86.3% of the femoral, 64.7% of the popliteal, and 92.5% of the tibial lesions.
In terms of device safety, this report supported the overall safety of the OAS (Table 3). Most dissections were minor and occurred in the treatment of femoral lesions in cases where the crown-to-reference vessel diameter ratio was less than 0.6, or when the total atherectomy time exceeded 360 seconds. These investigators also measured serum and urine markers of hemolysis and reported abnormal levels in approximately one-third of the cases.
The latest efficacy and safety data of the OAS comes from the CONFIRM registry series,14 which was funded by Cardiovascular Systems, Inc. These registries were conducted prospectively under a common protocol from 2009 to 2011. Patients undergoing OA at over 200 United States institutions were enrolled on an “all-comers” basis, and there were no exclusion criteria. Because each of the registries addressed the same patient population with the same data points collected, the data were combined into a large, single database representing 3135 patients with 4766 lesions. Of the 3135 patients presenting for treatment, 60% were male with a mean age of 72 years. Hypertension, hyperlipidemia, and coronary artery disease were each observed in over two-thirds of the patients in the series, 60% were diabetic, and 36% had renal disease. Based on angiographic estimation, 81% of the lesions were moderately to severely calcified. Treatment with the OAS and adjunctive balloon angioplasty ultimately resulted in a reduction in stenosis from an average of 88% to about 10%, with a very low percentage (5.1%) of bail-out stenting (due to dissection) reported.
Based upon all of these early reports, the lessons learned were that the OAS could perform safely and could effectively achieve luminal gain, especially in conjunction with balloon angioplasty alone. However, there were still some concerns regarding the laboratory evidence of hemolysis that was observed. This prompted a clinical trial specifically designed to prospectively evaluate the clinical significance of hemolysis during OA.15
The CLEAR (Study to Determine the CLinical Significance of HEmolysis During Orbital AtheRectomy) study was designed to prospectively evaluate the frequency, extent, and clinical significance of red blood cell hemolysis during OA treatment of symptomatic PAD.15
The primary endpoint was the first occurrence of clinically significant hemolysis 24 hours post atherectomy or just prior to discharge. Secondary endpoints included any clinical symptoms or signs potentially related to hemolysis. Participants were on average 71 years old, with 58% having Rutherford class 2-3 symptoms and 39% falling into the Rutherford class 4-6 categories.
Laboratory evidence of hemolysis was observed in 35.5% of subjects (11/31 patients). Mean levels of plasma-free hemoglobin (PfHgb) started at 17.6 ± 24.7 mg/dL at baseline, increased to 169.5 ± 169.7 mg/dL immediately post OA, and then decreased to 31.6 ± 22.7 mg/dL 12 hours post OA. More importantly, none of the subjects met criteria for any clinically significant event that was likely caused by hemolysis. Multivariate analysis revealed several predictors that were associated with a maximum rise in PfHgb, including calcified (as opposed to fibrous) plaque morphology, use of solid 70 micron crown (versus a classic crown), low baseline glomerular filtration rate, and longer OA run times. The data collected from this report were not only used to modify the device itself, but also to propose guidelines regarding the optimal technique for OA.16
After demonstrating the OAS safety profile, two prospective, multicenter, randomized studies were conducted in order to demonstrate the effectiveness of OA in calcified lesions. First, the CALCIUM 360°17 study evaluated short-term and 1-year outcomes in 50 CLI patients with calcified lesions below-the-knee randomized to OA followed by POBA versus POBA alone. All patients had severe PAD in the popliteal and tibial arteries (>50% stenosis and Rutherford class 4-6). The primary endpoint was procedural success, defined as achieving a final residual stenosis <30% with no bail-out stenting and no arterial dissections of types C through F. Procedural success was higher at 93.1% (27/29 lesions) for OA plus POBA patients compared to 82.4% (28/34 lesions) for POBA alone, although not statistically significant (P=.27). Bail-out stenting was required in 6.9% of the OA plus POBA lesions versus 14.3% of the POBA only treated lesions (P=.44). At 1-year follow-up, there were no amputations in either group related to the index procedure. Freedom from target vessel revascularization and all-cause mortality was seen in 93.3% and 100%, respectively, in the OA plus POBA group, compared to 80.0% (P=.14) and 68.4% (P=.01), respectively, for the same endpoints in the POBA group. The authors concluded that this small pilot trial demonstrated a trend toward fewer dissections and a lower rate of bail-out stenting with an OA-first strategy to treat below-the-knee calcified lesions, but this would have to be further supported in a larger confirmatory trial.
The second randomized trial was the COMPLIANCE 360°18 study, which examined the effect of OA prior to POBA on changing vessel compliance. Fifty patients with 65 symptomatic, femoropopliteal calcified lesions were equally randomized to OA plus POBA versus POBA alone. Mean lesion length for the study was 68 mm. Eighty-seven percent of the 38 lesions in the OA plus POBA arm compared to 19% of 27 lesions in the POBA arm met the angiographic endpoint of ≤30% residual stenosis after primary therapy (P<.001). Mean maximum balloon pressure was 4.0 ± 1.3 atm in the OA plus POBA arm versus 9.1 ± 3.5 atm in the POBA arm (P<.001). Two lesions in the OA plus POBA arm (5.3%) versus 21 lesions in the POBA arm (77.8%) required adjunctive stenting due to residual stenosis >30% (P<.001). TLR or duplex ultrasound-guided restenosis (defined as a peak systolic velocity ratio ≥2.5) at 12 months occurred in 5/23 lesions in the POBA arm and 6/32 lesions in the OA plus POBA arm (P=.10).
These two randomized studies, although small, provide the foundation for the concept of plaque modification prior to POBA. Importantly, they clearly confirm the original notion that pretreatment with OA reduces the need for further stenting, which is a technology that has shown to have limitations in the lower-extremity arterial bed.19
Conclusions and future trends. In recent times, there has been a resurgence of interest in the use of local pharmacology to prevent neointimal proliferation following initial endovascular therapy. Using novel drug delivery platforms, drug-coated balloons (DCBs) have shown promise in randomized clinical trials. In both the THUNDER and FEMPAC trials,20,21 the use of paclitaxel-eluting balloon angioplasty was superior to POBA for the treatment of de novo and restenotic femoropopliteal lesions in terms of both 6-month late lumen loss as well as TLR, with durability out to 2 years. Seemingly, the combination of DCB with OA for calcified stenoses is ideal, with respect to first modifying the plaque in a fashion that preserves medial integrity and then locally delivering antiproliferative drug directly to the vessel wall. While no confirmatory data are yet available, trials are underway to investigate the efficacy and safety of directional and laser atherectomy with adjunctive DCB technology (ie, the DEFINITIVE AR and PHOTOPAC trials).
The evolution of the OAS has been considerable, as evidenced by the numerous device modifications that have occurred since the technology’s inception as a direct result of lessons learned from clinical trials. As a result, the endovascular community has the advantage to use a refined technology that has proven to be safe and effective in calcified vessels, not only as a stand-alone therapy but also as a means to alter plaque morphology for adjunctive low-pressure balloon angioplasty or even stent expansion if desired. Orbital atherectomy may also serve as a prerequisite to vessel preparation that will allow for more effective administration of future technologies.
References
- Schillinger M, Haumer M, Schlerka G, et al. Restenosis after percutaneous transluminal angioplasty in the femoropopliteal segment: the role of inflammation. J Endovasc Ther. 2001;8(5):477-483.
- Cejna M, Thurnher S, Illiasch H, et al. PTA versus Palmaz stent placement in femoropopliteal artery obstructions: a multicenter prospective randomized study. J Vasc Interv Radiol. 2001;12(1):23-31.
- Schillinger M, Sabeti S, Loewe C, et al. Balloon angioplasty versus implantation of nitinol stents in the superficial femoral artery. N Engl J Med. 2006;354(18):1879-1888.
- Laird JR, Katzen BT, Scheinert D, et al. Nitinol stent implantation versus balloon angioplasty for lesions in the superficial femoral artery and proximal popliteal artery: twelve-month results from the RESILIENT randomized trial. Circ Cardiovasc Interv. 2010;3(3):267-276.
- Rogers JH, Laird JR. Overview of new technologies for lower extremity revascularization. Circulation. 2007;116(18):2072-2085.
- Mohler ER 3rd, Gannon F, Reynolds C, et al. Bone formation and inflammation in cardiac valves. Circulation. 2001;103(11):1522-1528.
- Bostrom K, Watson KE, Horn S, et al. Bone morphogenetic protein expression in human atherosclerotic lesions. J Clin Invest. 1993;91(4):1800-1809.
- Moussa I, Di Mario C, Colombo A. Plaque removal prior to stent implantation in native coronary arteries: why? When? And how? Semin Interv Cardiol. 1998;3(2):57-63.
- Makam P. Use of orbital atherectomy treatment in a high-volume clinical practice modifies non-compliant plaque to deliver durable long-term results. J Invasive Cardiol. 2013;25(2):85-88.
- Zeller T, Sievert H, Frank U, et al. TCT 40: Initial clinical experience with the “orbital atherectomy system.” Am J Cardiol. 2005;96:19H.
- Scheinert D, Sievert H, Maleux G, et al. TCT-612: final results of a european study of orbital atherectomy: a new technology for treating occlusive peripheral arterial disease. Am J Cardiol. 2008;102:230i.
- Safian RD, Niazi K, Runyon JP, et al. Orbital atherectomy for infrapopliteal disease: device concept and outcome data for the OASIS trial. Catheter Cardiovasc Interv. 2009;73(3):406-412.
- Korabathina R, Mody KP, Yu J, et al. Orbital atherectomy for symptomatic lower extremity disease. Catheter Cardiovasc Interv. 2010;76(3):326-332.
- Das T, Mustapha J, Indes J, et al. Technique optimization of orbital atherectomy in calcified peripheral lesions of the lower extremities: the CONFIRM series, a prospective multicenter registry. Catheter Cardiovasc Interv. 2014;83(1):115-122. Epub 2013 Oct 7.
- Staniloae CS, Korabathina R, Lane TA, et al. Study to determine the clinical significance of HEmolysis During Orbital AtheRectomy (CLEAR study). J Endovasc Ther. 2011;18(1):57-63.
- Adams GL, Khanna PK, Staniloae CS, et al. Optimal techniques with the Diamondback 360 degrees system achieve effective results for the treatment of peripheral arterial disease. J Cardiovasc Transl Res. 2011;4(2):220-229.
- Shammas NW, Lam R, Mustapha J, et al. Comparison of orbital atherectomy plus balloon angioplasty vs. balloon angioplasty alone in patients with critical limb ischemia: results of the CALCIUM 360 randomized pilot trial. J Endovasc Ther. 2012;19(4):480-488.
- Dattilo R, Himmelstein SI, Cuff RF. The COMPLIANCE 360° trial: a randomized, prospective, multicenter, pilot study comparing acute and long-term results of orbital atherectomy to balloon angioplasty for calcified femoropopliteal disease. J Invasive Cardiol. 2014 (in press).
- Scheinert D, Scheinert S, Sax J, et al. Prevalence and clinical impact of stent fractures after femoropopliteal stenting. J Am Coll Cardiol. 2005;45(2):312-315.
- Tepe G, Zeller T, Albrecht T, et al. Local delivery of paclitaxel to inhibit restenosis during angioplasty of the leg. N Engl J Med. 2008;358(7):689-699.
- Werk M, Langner S, Reinkensmeier B, et al. Inhibition of restenosis in femoropopliteal arteries: paclitaxel-coated versus uncoated balloon: femoral paclitaxel randomized pilot trial. Circulation. 2008;118(13):1358-1365.
_________________________________
From the 1Heart and Vascular Institute, New York University Medical Center, New York, New York and 2Bayfront Cardiovascular Associates, Bayfront Health, St. Petersburg, Florida.
Disclosure: The authors have completed and returned the ICMJE Form for Disclosure of Potential Conflicts of Interest. Cezar S Staniloae has received consultant / proctorship fees from CSI. Ravikiran Korabathina has disclosed no conflict of interests regarding this publication.
Manuscript submitted September 26, 2013, provisional acceptance given October 18, 2013, final version accepted November 12, 2013.
Address for correspondence: Cezar S. Staniloae, MD, 530 First Avenue, New York, NY 10016. Email: cezar.staniloae@nyumc.org





