

ADVERTISEMENT
The Impact of Proximal Vessel Tortuosity on the Outcomes of Chronic Total Occlusion Percutaneous Coronary Intervention: Insights From a Contemporary Multicenter Registry
Abstract: Introduction. We examined the impact of proximal vessel tortuosity on the outcomes of chronic total occlusion (CTO) percutaneous coronary intervention (PCI). Methods. The baseline clinical and angiographic characteristics and procedural outcomes of 1618 consecutive CTO-PCIs performed between 2012 and 2016 at 14 United States centers in 1589 patients were reviewed. Results. Mean patient age was 65.3 ± 10.0 years and 85% were men. Moderate/severe proximal vessel tortuosity was present in 35.7% of target lesions. Compared with non-tortuous lesions, tortuous lesions had longer length (30 mm [interquartile range, 20-50 mm] vs 28 mm [interquartile range, 16-40 mm]; P<.001), more proximal cap ambiguity (36% vs 28%; P<.01), and more frequent utilization of the retrograde approach (52% vs 37%; P<.001). Moderate/severe proximal vessel tortuosity was associated with lower technical success rates (84.1% vs 91.3%; P<.001) and procedural success rates (82.3% vs 89.9%; P<.001), but similar incidence of major cardiac adverse events (3.0% vs 2.5%; P=.59). Moderate/severe tortuosity was associated with longer procedure time and fluoroscopy time, higher air kerma radiation dose, and larger contrast volume. Conclusion. In a contemporary multicenter registry, moderate/severe proximal vessel tortuosity was present in approximately one-third of target CTO lesions and was associated with more frequent use of the retrograde approach and lower success rates, but similar complication rates.
J INVASIVE CARDIOL 2017;29(8):264-270. Epub 2017 May 15.
Key words: tortuosity, chronic total occlusion, percutaneous coronary intervention
Coronary tortuosity can hinder vessel wiring and equipment delivery and has been associated with lower success rates and higher complications rates in percutaneous coronary intervention (PCI).1-3 Coronary tortuosity affects the efficiency and success of chronic total occlusion (CTO)-PCI and is included both in the Japanese chronic total occlusion (J-CTO) score for predicting successful guidewire crossing within the first 30 minutes of the procedure,4 and the Progress-CTO score5 for predicting technical success. We examined a multicenter United States registry to determine the impact of tortuosity on outcomes of contemporary CTO-PCI.
Methods
Patient population. We examined the baseline clinical and angiographic characteristics and outcomes of CTO-PCIs performed between 2012 and 2016 at 14 United States centers: Appleton Cardiology, Appleton Wisconsin; Baylor Hamilton Heart and Vascular Hospital, Dallas, Texas; Central Arkansas VA Healthcare System, Little Rock, Arkansas; Columbia University, New York, New York; Henry Ford Hospital, Detroit, Michigan; Massachusetts General Hospital, Boston, Massachusetts; Medical Center of the Rockies, Loveland, Colorado; Piedmont Heart Institute, Atlanta Georgia; St. Joseph Medical Center, Bellingham Washington; St. Luke’s Health System’s Mid-America Heart Institute, Kansas City, Missouri; Torrance Memorial Center, Torrance, California; University of Pittsburgh Medical Center, Presbyterian University Hospital, Pittsburgh, Pennsylvania; VA North Texas Health Care System, Dallas, Texas; and University of California, San Diego Healthcare System, San Diego, California.
Enrollment was performed during only part of the study period in some centers due to participation in other studies. Data collection was performed both prospectively and retrospectively and was recorded in a dedicated online database (Progress CTO: Prospective Global Registry for the Study of Chronic Total Occlusion Intervention; Clinicaltrials.gov Identifier: NCT02061436).5-9 The study was approved by the institutional review board of each site.
Definitions. Coronary CTOs were defined as coronary lesions with Thrombolysis in Myocardial Infarction (TIMI) grade 0 flow of at least 3-month duration. Estimation of the occlusion duration was based on first onset of anginal symptoms, prior history of myocardial infarction in the target-vessel territory, or comparison with a prior angiogram. Calcification was assessed by angiography as mild (spots), moderate (involving ≤50% of the reference lesion diameter), or severe (involving >50% of the reference lesion diameter).
Moderate proximal vessel tortuosity was defined as the presence of at least 2 bends >70° or 1 bend >90° and severe tortuosity as 2 bends >90° or 1 bend >120° in the CTO vessel.
The J-CTO score was calculated as described by Morino et al.4 The Progress CTO score was calculated as described by Christopoulos et al.5Technical success was defined as successful CTO revascularization with achievement of <30% residual diameter stenosis within the treated segment and restoration of TIMI grade 3 antegrade flow. Procedural success was defined as achievement of technical success with no in-hospital major adverse cardiac event (MACE). In-hospital MACE included any of the following adverse events prior to hospital discharge: death, myocardial infarction, urgent repeat target-vessel revascularization with either PCI or coronary artery bypass graft (CABG) surgery, tamponade requiring either pericardiocentesis or surgery, and stroke. Myocardial infarction was defined using the Third Universal Definition of Myocardial Infarction.10
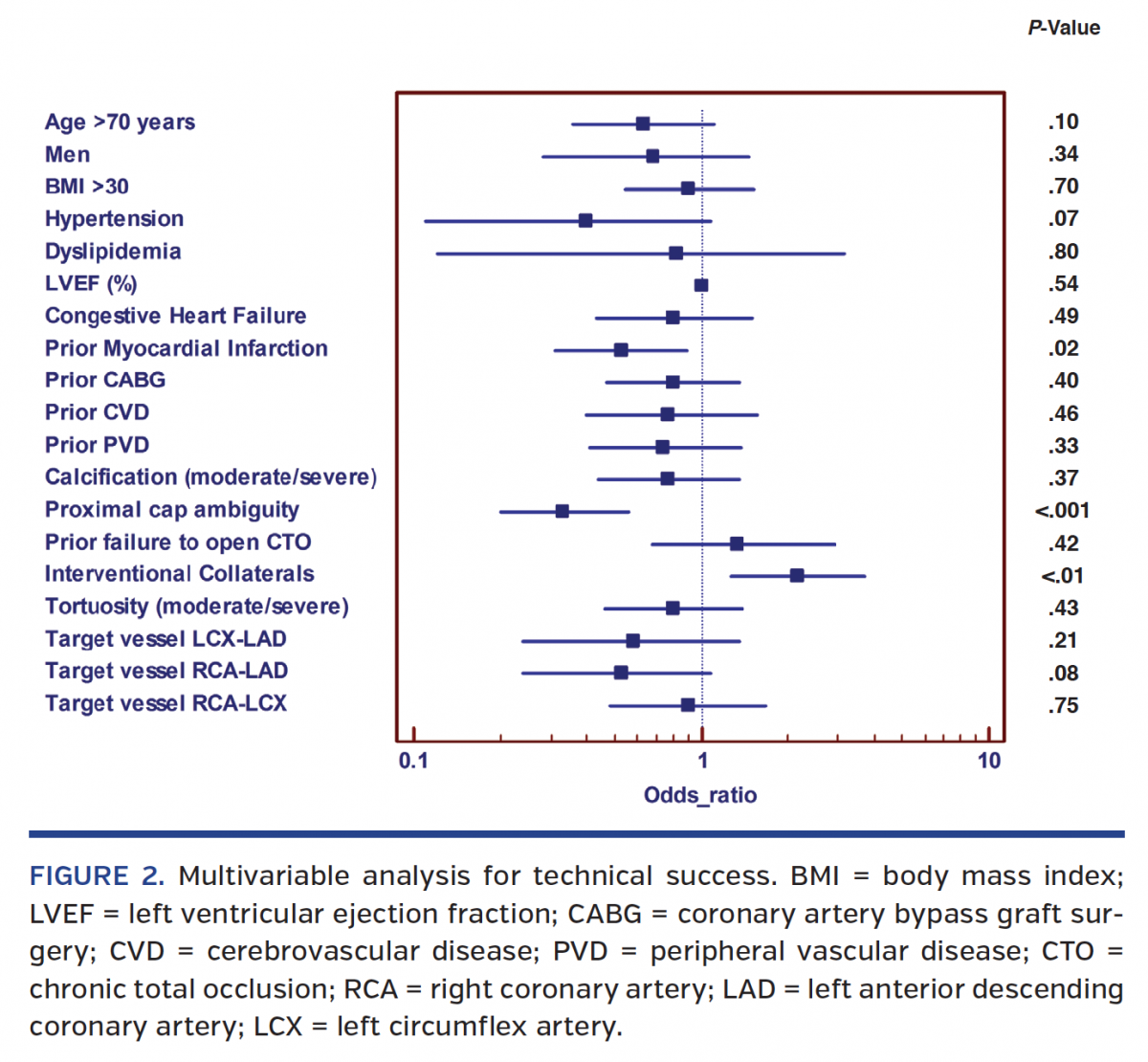
Statistical analysis. Comparisons were performed between CTO-PCI procedures classified into two groups according to whether moderate or severe proximal tortuosity was present in the CTO target vessel or not. Continuous variables were presented as mean ± standard deviation or median (interquartile range) and were compared using the Student’s t-test or Wilcoxon rank-sum test, as appropriate. Categorical data were reported as frequencies or percentages and compared using the Chi-squared test or Fisher’s exact test, as appropriate. Logistic regression analysis was performed to identify clinical and angiographic parameters associated with technical success. Variables with P<.10 on univariate analysis (age >70 years, gender, hypertension, dyslipidemia, left ventricular ejection fraction in units, congestive heart failure and myocardial infarction, prior CABG, peripheral arterial disease and cerebrovascular disease, presence of moderate or severe calcification, proximal cap ambiguity, prior failed CTO-PCI, presence of interventional collaterals, moderate or severe proximal vessel tortuosity, and CTO target vessel) were included in a multivariate model. All statistical analyses were performed with JMP 11.0 (SAS Institute). Two-sided P-values <.05 were considered statistically significant.
Results
Baseline clinical characteristics. We analyzed 1618 consecutive CTO-PCIs performed in 1589 patients. The baseline clinical characteristics of the study patients are presented in Table 1. Mean age was 65.3 ± 10.0 years and 85% of the study subjects were men. Nearly one-half of the patients had diabetes mellitus or prior myocardial infarction and approximately one-third had prior heart failure and prior CABG. Patients with moderate/severe tortuosity were more likely to have diabetes mellitus and prior CABG.

Angiographic characteristics. The angiographic characteristics of the CTO target lesions are summarized in Table 2. Moderate or severe proximal vessel tortuosity was present in 35.7%. The most common target vessel was the right coronary artery (56%) followed by the left anterior descending artery (23%) and the circumflex (21%). The most common final successful crossing strategy was antegrade wire escalation (41%) followed by retrograde (25%) and antegrade dissection and reentry (23%). Moderate or severe calcification was present in more than one-half of the lesions (57%), and interventional collaterals were present in 57%.

Lesions with moderate or severe proximal vessel tortuosity were more complex, with higher J-CTO and Progress CTO scores and moderate or severe calcification. Moreover, tortuous lesions were longer and more likely to exhibit proximal cap ambiguity and to require retrograde crossing attempts (Table 2).
Procedural outcomes. Procedural outcomes are shown in Table 3 and Figure 1. Overall technical and procedural success rates were 89% and 87%, respectively, and the MACE rate was 2.7%. Lesions with moderate or severe tortuosity had lower technical success rates (84% vs 91%; P<.001) and procedural success rates (83% vs 90%; P<.001), but similar MACE rates (3.0% vs 2.5%; P=.59) as compared with cases with mild or no tortuosity. There was no difference between the various components of MACE (death, myocardial infarction, repeated PCI, stroke, emergency CABG, and pericardiocentesis). However, on multivariable analysis, moderate or severe tortuosity was not independently associated with technical success (Figure 2). PCI of lesions with moderate or severe tortuosity required longer procedure and fluoroscopy times, higher air kerma radiation doses, and higher contrast volumes.



The most common guide-support technique to address proximal vessel tortuosity was use of guide-catheter extensions followed by side-branch anchor and distal-anchor techniques (Table 2; Figure 3). Among the cases with moderate or severe proximal vessel tortuosity, the most commonly used antegrade guide catheter was AL 1 (54 cases; 29.4%), while the most commonly used retrograde guide catheter was the EBU 4.0 (Figure 4).


Discussion
 The main findings of this study are that significant proximal vessel tortuosity: (1) was present in approximately one-third of target CTOs; (2) was associated with lower technical and procedural success, but similar complication rates; (3) required more supportive guide catheters and guide-catheter techniques to address tortuosity; and (4) required use of the retrograde approach more frequently to obtain success.
The main findings of this study are that significant proximal vessel tortuosity: (1) was present in approximately one-third of target CTOs; (2) was associated with lower technical and procedural success, but similar complication rates; (3) required more supportive guide catheters and guide-catheter techniques to address tortuosity; and (4) required use of the retrograde approach more frequently to obtain success.
Tortuosity is common among complex coronary lesions. Okamura et al reported 34.2% prevalence of proximal vessel tortuosity in a Japanese multicenter CTO-PCI registry.11 In an analysis of 1582 retrograde CTO-PCIs from the EuroCTO club, Galassi et al reported moderate tortuosity in 28.5% and severe tortuosity in 9.7%.12 Baykan et al reported a lower prevalence of severe 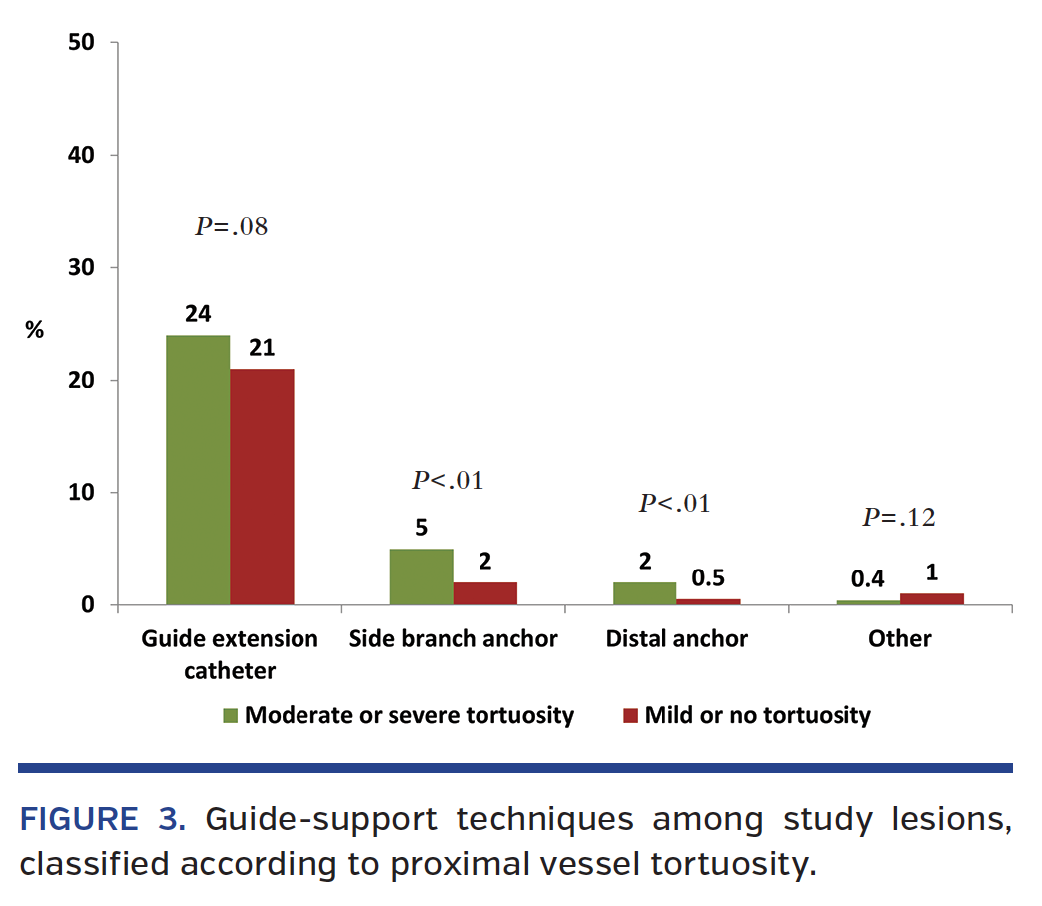 tortuosity (10.4%) among 173 CTO-PCIs, although tortuosity was associated with technical failure (odds ratio: 0.085; 95% confidence interval, 0.013-0.579; P=.01), where severe tortuosity was defined as ≥1 bend of 90° or more, or ≥3 bends of 45°-90° proximal to the diseased segment.1
tortuosity (10.4%) among 173 CTO-PCIs, although tortuosity was associated with technical failure (odds ratio: 0.085; 95% confidence interval, 0.013-0.579; P=.01), where severe tortuosity was defined as ≥1 bend of 90° or more, or ≥3 bends of 45°-90° proximal to the diseased segment.1
The pathogenesis of coronary tortuosity remains unclear, but tortuosity is associated with increasing age, hypertension, atherosclerosis, and genetic predisposition.13-16 Han created a biomedical model of arterial buckling, demonstrating that arteries buckle due to high blood pressure, reduced axial stretch, or changes in the arterial wall stiffness and dimensions, lending support to the association of tortuosity with hypertension, aging, atherosclerosis and other pathological arterial changes.14,17
Several techniques have been developed to overcome the challenges associated with PCI of tortuous lesions. Wiring of such lesions can be hindered by decreased wire torquability after passing the first curves and can be facilitated by using large size and supportive-shaped guide catheters and/or guide-catheter extensions, advancing wires through a microcatheter and using new-generation, composite-core wires or polymer-jacketed guidewires.18 Use of stiff wires, however, could straighten the vessel and possibly lead to the development of coronary “pseudolesions.”3 In our study, the most commonly used guide catheters in moderate or severe proximal vessel tortuosity were the Amplatz left and extra back-up guides, which provide strong guide-catheter support. Moreover, use of dissection/reentry crossing techniques can facilitate crossing of tortuous CTOs by tracking the vessel bends with low risk of exiting the adventitia and leading to perforation. The prevalence of moderate/severe calcification was high (72%) in the majority of patients with proximal vessel tortuosity and likely contributed to the use of the retrograde approach in over one-half of the study cohort. Ultimately, the use of the above techniques resulted in >80% procedural and technical success rates in this challenging group of CTO patients.
Study limitations. There was no core laboratory analysis of the study angiograms and no independent event adjudication, and therefore assessment of angiographic characteristics was susceptible to operator-related bias. The CTO-PCI procedures were performed by centers with significant expertise in CTO-PCI; hence, these findings may not be generalizable to less experienced centers and operators. No follow-up data were available for analysis and the long-term outcomes associated with coronary tortuosity would require additional investigation. Lastly, the presence of tortuosity was determined by visual estimate.
Conclusion
In summary, moderate or severe proximal vessel tortuosity is common in CTO target lesions and is associated with lower efficiency and procedural success, but similar complication rates as compared with lesions with mild or no tortuosity.
Acknowledgment. Study data were collected and managed using REDCap electronic data capture tools hosted at University of Texas Southwestern Medical Center.19 REDCap (Research Electronic Data Capture) is a secure, web-based application designed to support data capture for research studies, providing: (1) an intuitive interface for validated data entry; (2) audit trails for tracking data manipulation and export procedures; (3) automated export procedures for seamless data downloads to common statistical packages; and (4) procedures for importing data from external sources.
References
1. Baykan AO, Gur M, Acele A, et al. Predictors of successful percutaneous coronary intervention in chronic total coronary occlusions. Postepy Kardiol Interwencyjnej. 2016;12:17-24.
2. Ellis SG, Vandormael MG, Cowley MJ, et al. Coronary morphologic and clinical determinants of procedural outcome with angioplasty for multivessel coronary disease. Implications for patient selection. Multivessel Angioplasty Prognosis Study Group. Circulation. 1990;82:1193-1202.
3. Saeed B, Banerjee S, Brilakis ES. Percutaneous coronary intervention in tortuous coronary arteries: associated complications and strategies to improve success. J Interv Cardiol. 2008;21:504-511.
4. Morino Y, Abe M, Morimoto T, et al. Predicting successful guidewire crossing through chronic total occlusion of native coronary lesions within 30 minutes: the J-CTO (Multicenter CTO Registry in Japan) score as a difficulty grading and time assessment tool. JACC Cardiovasc Interv. 2011;4:213-221.
5. Christopoulos G, Kandzari DE, Yeh RW, et al. Development and validation of a novel scoring system for predicting technical success of chronic total occlusion percutaneous coronary interventions: the PROGRESS CTO (Prospective Global Registry for the Study of Chronic Total Occlusion Intervention) score. JACC Cardiovasc Interv. 2016;9:1-9.
6. Danek BA, Karatasakis A, Karmpaliotis D, et al. Development and validation of a scoring system for predicting periprocedural complications during percutaneous coronary interventions of chronic total occlusions: the Prospective Global Registry for the Study of Chronic Total Occlusion Intervention (PROGRESS CTO) complications score. J Am Heart Assoc. 2016;5.
7. Karmpaliotis D, Karatasakis A, Alaswad K, et al. Outcomes with the use of the retrograde approach for coronary chronic total occlusion interventions in a contemporary multicenter US registry. Circ Cardiovasc Interv. 2016 Jun;9(6).
8. Christopoulos G, Karmpaliotis D, Alaswad K, et al. Application and outcomes of a hybrid approach to chronic total occlusion percutaneous coronary intervention in a contemporary multicenter US registry. Int J Cardiol. 2015;198:222-228.
9. Christopoulos G, Menon RV, Karmpaliotis D, et al. The efficacy and safety of the “hybrid” approach to coronary chronic total occlusions: insights from a contemporary multicenter US registry and comparison with prior studies. J Invasive Cardiol. 2014;26:427-432.
10. Thygesen K, Alpert JS, Jaffe AS, et al. Third universal definition of myocardial infarction. Circulation. 2012;126:2020-2035.
11. Okamura A, Yamane M, Muto M, et al. Complications during retrograde approach for chronic coronary total occlusion: sub-analysis of Japanese multicenter registry. Catheter Cardiovasc Interv. 2016;88:7-14.
12. Galassi AR, Sianos G, Werner GS, et al. Retrograde recanalization of chronic total occlusions in Europe: procedural, in-hospital, and long-term outcomes from the Multicenter ERCTO registry. J Am Coll Cardiol. 2015;65:2388-2400.
13. Li Y, Shen C, Ji Y, Feng Y, Ma G, Liu N. Clinical implication of coronary tortuosity in patients with coronary artery disease. PLoS One. 2011;6:e24232.
14. Pancera P, Ribul M, Presciuttini B, Lechi A. Prevalence of carotid artery kinking in 590 consecutive subjects evaluated by echo color Doppler. Is there a correlation with arterial hypertension? J Intern Med. 2000;248:7-12.
15. Satish G, Nampoothiri S, Kappanayil M. Images in cardiovascular medicine. Arterial tortuosity syndrome: phenotypic features and cardiovascular manifestations. Circulation. 2008;117:e477-e478.
16. Jakob M, Spasojevic D, Krogmann ON, Wiher H, Hug R, Hess OM. Tortuosity of coronary arteries in chronic pressure and volume overload. Cathet Cardiovasc Diagn. 1996;38:25-31.
17. Han HC. A biomechanical model of artery buckling. J Biomech. 2007;40:3672-3678.
18. Khalili H, Vo MN, Brilakis ES. Initial experience with the Gaia composite core guidewires in coronary chronic total occlusion crossing. J Invasive Cardiol. 2016;28:E22-E25.
19. Harris PA, Taylor R, Thielke R, Payne J, Gonzalez N, Conde JG. Research electronic data capture (REDCap) – a metadata-driven methodology and workflow process for providing translational research informatics support, J Biomed Inform. 2009;42:377-381.
From the 1VA North Texas Healthcare System and UT Southwestern Medical Center, Dallas, Texas; 2Division of Invasive Cardiology, Second Department of Internal Medicine and Cardiology Center, University of Szeged, Szeged, Hungary; 3Columbia University, New York, New York; 4Henry Ford Hospital, Detroit, Michigan; 5Massachusetts General Hospital and Harvard Medical School, Boston, Massachusetts; 6Beth Israel Deaconess Medical Center, Boston, Massachusetts; 7VA San Diego Healthcare System and University of California San Diego, San Diego, California; 8Medical Center of the Rockies, Loveland, Colorado; 9University of Pittsburgh Medical Center Presbyterian, Pittsburgh, Pennsylvania; 10Central Arkansas Veterans Health System, Little Rock, Arkansas; 11Baylor Heart and Vascular Hospital, Dallas, Texas; 12University of Washington, Seattle, Washington; 13Piedmont Heart Institute, Atlanta, Georgia; 14Minneapolis VA Healthcare System and University of Minnesota, Minneapolis, Minnesota; 15Torrance Memorial Medical Center, Torrance, California; 16Boston Scientific, Natick, Massachusetts; and 17Minneapolis Heart Institute, Minneapolis, Minnesota.
Funding: The Progress CTO registry is supported by the Abbott Northwestern Hospital Foundation. REDCap (Research Electronic Data Capture) is supported by CTSA NIH Grant UL1-RR024982.
Disclosure: The authors have completed and returned the ICMJE Form for Disclosure of Potential Conflicts of Interest. Dr Karacsonyi reports no disclosures. Dr Karmpaliotis reports speaker bureau, Abbott Vascular, Medtronic, and Boston Scientific. Dr Alaswad reports consulting fees from Terumo and Boston Scientific; consultant (non-financial), Abbott Laboratories. Dr Jaffer reports consultant fees from Abbott Vascular and Boston Scientific. Dr Yeh reports personal fees from Abbott Vascular; personal fees and grant funds from Boston Scientific; receipt of the Career Development Award (1K23HL118138) from the National Heart, Lung, and Blood Institute. Dr Patel reports consulting fees from Abbott Vascular. Dr Mahmud reports clinical events committee for St. Jude; grant support and personal fees from Corindus; speaker’s bureau and advisory board for Medtronic; educational program honoraria from Abbott Vascular; and clinical trial support from Medinol. Dr Choi reports advisory board fees from Medtronic and Abbott Vascular; speaker’s bureau for Boston Scientific. Dr Toma reports consulting fees from Abbott Vascular. Drs Doing, Uretsky, and Moses report no disclosures. Dr Kirtane reports institutional research grants to Columbia University from Boston Scientific, Medtronic, Abbott Vascular, Abiomed, St. Jude Medical, Vascular Dynamics, Glaxo SmithKline, and Eli Lilly. Dr Parikh reports membership on the speakers bureau for Abbott Vascular, Medtronic, CSI, Boston Scientific; advisory boards for Medtronic, Abbott Vascular, and Philips. Dr Ali reports grant support, consultant fees from St. Jude Medical; grant support from CSI; personal fees from Medtronic. Dr Lombardi reports equity with Bridgepoint Medical. Dr Kandzari reports research/grant support and consulting honoraria from Boston Scientific and Medtronic Cardiovascular, and research/grant support from Abbott. Dr Lembo reports speaker’s bureau for Medtronic; advisory board for Abbott Vascular, Medtronic. Dr Garcia reports no disclosures. Dr Wyman reports honoraria/consulting fees from Boston Scientific, Abbott Vascular, and Spectranetics. Drs Martinez-Parachini, Karatasakis, Danek, Alame, and Resendes report no disclosures. Dr Rangan reports research grants from InfraReDx, Inc., and the Spectranetics Corporation. Dr Ungi reports no disclosures. Dr Thompson is an employee of Boston Scientific. Dr Banerjee reports research grants from Gilead and the Medicines Company; consultant/speaker honoraria from Covidien and Medtronic; ownership in MDCare Global (spouse); intellectual property in HygeiaTel. Dr Brilakis reports consulting/speaker honoraria from Abbott Vascular, Asahi Intecc, Cardinal Health, Elsevier, GE Healthcare, and St Jude Medical; research support from Boston Scientific and InfraRedx; spouse is an employee of Medtronic.
Manuscript submitted January 20, 2017 and accepted February 3, 2017.
Address for correspondence: Emmanouil S. Brilakis, MD, PhD, Minneapolis Heart Institute, 920 E. 28th Street #300, Minneapolis, MN 55407. Email: esbrilakis@gmail.com
