

The Evolution and Prognostic Value of N-Terminal Brain Natriuretic Peptide in Predicting 1-Year Mortality in Patients Following Transcatheter Aortic Valve Implantation
Download a PDF of this article.
Abstract: Aims. N-terminal pro-brain natriuretic peptide (NT-proBNP) has been found to correlate with the severity of aortic valve stenosis and to provide prognostic information in aortic stenosis patients undergoing surgical aortic valve replacement. There is a paucity of data describing the association between clinical outcomes after TAVI and NT-proBNP levels. We investigated the evolution and prognostic value of NT-proBNP levels after TAVI. Method and Results. We prospectively collected data on the baseline characteristics, NT-proBNP levels (baseline, post-treatment and discharge) and adverse clinical outcomes of patients undergoing TAVI from 2007 to 2010. Using a univariable and multivariable Cox regression model, pre- and postimplantation NT-proBNP tertile levels were correlated to 30-day and 1-year mortality. A total of 373 patients underwent TAVI with either the Medtronic CoreValve or Edwards SAPIEN prosthesis. The cumulative 30-day and 1-year mortality was 7.3% and 18%, respectively. Rehospitalization for heart failure was observed in 0.8% at 30 days and 7.8% at 1 year. The tertile baseline NT-proBNP levels were identified as ≤1570 ng/L, 1571 to 4690 ng/L and ≥4691 ng/L. In the univariable analysis, baseline (HR, 1.01; 95% CI, 1.001-1.02; P=.02) and post-treatment NT-proBNP (HR 1.02; 95% CI, 1.002-1.04; P=.04) were predictors for 1-year mortality. In the multivariable analysis, however, only baseline NT-proBNP and atrial fibrillation were identified as predictors for the 1-year mortality (HR, 1.02; 95% CI, 1.01-1.05; P=.006 and HR, 3.4; 95% CI, 1.25-9.5; P=.017, respectively). Conclusions. NT-proBNP and atrial fibrillation were predictors for 1-year mortality, offer independent prognostic information, and identify patients being at increased risk for mortality. Thus, NT-proBNP reveals more incremental value for patient selection and should be included in the risk stratification of patients undergoing TAVI.
J INVASIVE CARDIOL 2013;25(1):38-44
Key words: NT-proBNP, TAVI, prognostic value of BNP, biomarkers in TAVI
_________________________________________________
Brain type natriuretic peptide (BNP) is an amino acid protein synthesized by the myocardium that is cleaved into two fragments yielding BNP and NT-proBNP. The 2008 European Heart Failure Guidelines highlight BNP as a diagnostic and prognostic marker in heart failure patients.1 In patients with aortic stenosis, BNP levels correlate with functional status and can also serve as a prognostic marker for patients with asymptomatic or symptomatic aortic valve stenosis undergoing surgical aortic valve replacement (SAVR)2-6 or those undergoing balloon aortic valvuloplasty.7
There is very little information, however, about the prognostic implications of BNP levels from patients undergoing transcatheter aortic valve implantation (TAVI). The aims of this study are to: (1) characterize pre- and postprocedural BNP levels in patients with severe AS undergoing TAVI; and (2) to examine the correlation between NT-proBNP levels and clinical outcomes.
Abbreviations
- NT-proBNP N-terminal brain natriuretic peptide
- SAVR surgical aortic valve replacement
- AS aortic stenosis
- TAVI transcatheter aortic valve implantation
- NYHA New York Heart Association
- LVEF left ventricular ejection fraction
Methods
Study population. From November 2007 to April 2010 we prospectively collected the pre- and post-treatment data of 373 consecutive patients with severe aortic valve stenosis who underwent TAVI with either the Medtronic CoreValve (Medtronic CoreValve) or Edwards SAPIEN (Edwards Lifesciences) prosthesis. Patient screening and TAVI (including feasibility and safety, vascular access site and prosthesis size selection) were discussed among a multidisciplinary team consisting of cardiac surgeons, invasive and non-invasive cardiologists, and anesthesiologists. All patients provided informed consent prior to treatment. Patients without complete data were excluded from the study.
Clinical follow-up exams, during a period of 12 ± 2 months, were obtained by clinical visits and/or through telephone contacts. Death and cardiac rehospitalization were recorded from all patients.
Procedural technique. Procedural details have been published elsewhere.8 Briefly, under conscious sedation or general anesthesia, patients underwent implantation of the Medtronic CoreValve (Medtronic CoreValve) or Edwards SAPIEN (Edwards Lifesciences, Inc) device in a hybrid procedural suite via a transfemoral, transaxillary, transapical, or transaortic route. The transfemoral procedures were performed using a surgical cut-down or pre-closure techniques with one ProStar and one ProGlide device (Abbott).
Measurement of BNP. Blood samples for BNP levels were drawn into chilled EDTA acid test tubes the day before TAVI (baseline), immediately after (post-treatment) and on the day of hospital discharge (7 ± 4 days post implantation). After 20 minutes of centrifugation, separated plasma samples were processed by a fluorescence immunoassay for measurement of B-type natriuretic peptide levels (Elecsys proBNP; Roche Diagnostics GmbH).
Echocardiographic data. At study entry, all patients underwent echocardiographic evaluation at baseline, at discharge, and at 1 year after TAVI. The echocardiographic protocol contain measurement of the aortic annulus, the interventricular septum, the aortic valve peak and mean gradient, aortic valve area and the left ventricular ejection fraction using commercially available ultrasound systems (Siemens, ACUSON. Sequoia. 512). Left ventricular ejection fraction (LVEF) was estimated according to Simpson’s rule. The simplified Bernoulli equation was used to calculate the transaortic gradients and the aortic valve area was calculated by the continuity equation. All echocardiographic examinations were performed by experienced echocardiographers.
Study endpoints. Primary endpoints were all-cause mortality and rehospitalization for heart failure at 30 days and 1-year after TAVI. Outcome variables were collected from patient interviews (ambulatory clinic or telephone calls) using a standardized questionnaire or review of electronic hospital records.
Statistics. Continuous variables were presented as means ± standard deviation or medians ± interquartile ranges (IQRs). Comparisons of continuous variables between groups were performed with the Student’s t-test or the Mann-Whitney U-test in case of non-parametric distribution. Categorical variables were compared with the chi-square or Fisher’s exact test if the expected frequency was less than 5. A two-sided P-value <.05 was considered to be significant.
For the analysis, NT-proBNP levels were divided into tertiles (≤1570 ng/L, 1571 to 4690 ng/L, and ≥4691 ng/L). Consequently, three groups were identified: first tertile with 124 patients, second tertile with 126 and third tertile with 123 patients. Unpaired Student t-tests or repeated-measures ANOVA with Bonferroni correction for multiple comparisons were used to compare continuous variables between the tertile groups.
 Kaplan-Meier estimator curves were used to examine the distribution of adverse outcomes on the basis of NT-proBNP tertiles. Log-rank test was used to compare differences between stratified groups.
Kaplan-Meier estimator curves were used to examine the distribution of adverse outcomes on the basis of NT-proBNP tertiles. Log-rank test was used to compare differences between stratified groups.
Using the Cox’s proportional hazards model, we studied the univariable and multivariable association between mortality and NT-proBNP (at baseline, post-treatment and discharge) and baseline characteristics (see variables in Table 1). Models were generated with a forward stepwise analysis. Factors with a P-value <.20 in the univariable analysis were entered into the multivariable analysis.
All data were analyzed with SPSS software (version 15 for Windows; SPSS Inc).
Results
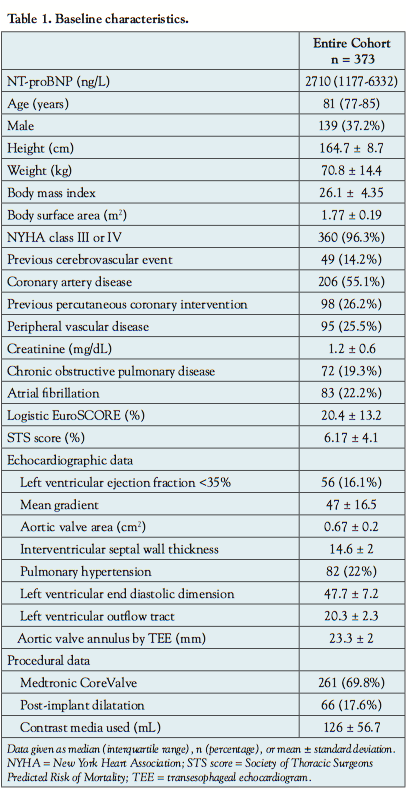
 Baseline characteristics. A total of 373 consecutive patients with severe aortic valve stenosis were enrolled in the study. Clinical characteristics and echocardiographic data of all patients are summarized in Table 1. Figures 1A and 1B illustrated the relationship between NT-proBNP levels and NYHA class, NT-proBNP and LVEF. Plasma levels of NT-proBNP correlates positively with the NYHA classification but negatively with the LV ejection fraction.
Baseline characteristics. A total of 373 consecutive patients with severe aortic valve stenosis were enrolled in the study. Clinical characteristics and echocardiographic data of all patients are summarized in Table 1. Figures 1A and 1B illustrated the relationship between NT-proBNP levels and NYHA class, NT-proBNP and LVEF. Plasma levels of NT-proBNP correlates positively with the NYHA classification but negatively with the LV ejection fraction.
NT-proBNP tertile analysis. NT-proBNP tertiles were ≤1570 ng/L, 1571 to 4690 ng/L, and ≥ 4691 ng/L. Table 2 summarizes the differences between the baseline NT-proBNP 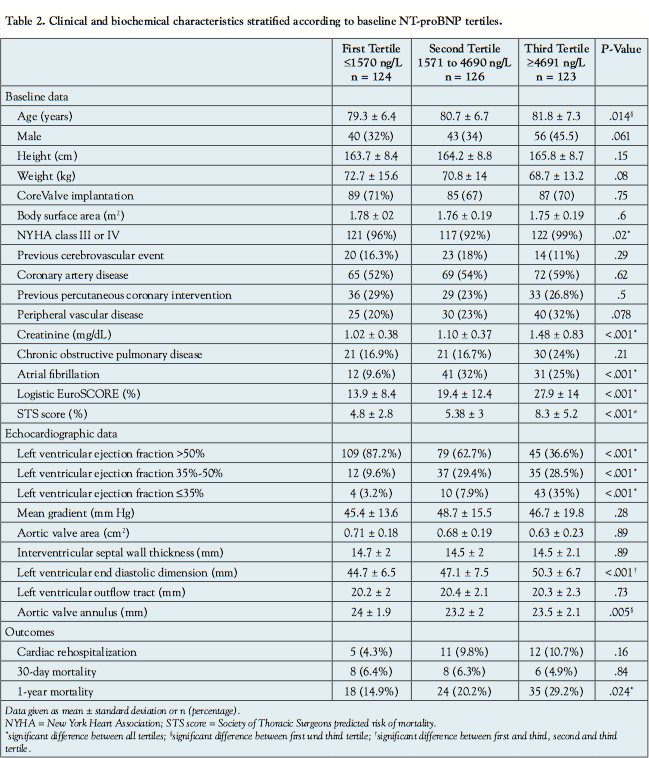 according to tertiles. Patients in the 3rd BNP tertile exhibited significantly higher preoperative creatinine levels than patients in the 1st tertile (1.48 ± 0.83 mg/dL (3rd tertile) vs 1.02 ± 0.38 mg/dL (1st tertile); P<.001), a 2-fold higher logistic EuroSCORE and STS score (Logistic EuroSCORE, 27.3 ± 14% vs 13.9 ± 8.4%, respectively; P<.001) (STS score, 8.3 ± 5.2% vs 4.8 ± 2.8%, respectively; P<.001). Furthermore, patients in the 3rd tertile had a 3 to 4-fold higher frequency of atrial fibrillation than patients in the 1st tertile (32% vs 9.6%, respectively, P<.001). There were no significant differences in 30-day mortality (P=.84) and cardiac rehospitalization rate (P=.16) among the NT-proBNP tertiles but a higher 1-year mortality in the 3rd tertile (P=.024).
according to tertiles. Patients in the 3rd BNP tertile exhibited significantly higher preoperative creatinine levels than patients in the 1st tertile (1.48 ± 0.83 mg/dL (3rd tertile) vs 1.02 ± 0.38 mg/dL (1st tertile); P<.001), a 2-fold higher logistic EuroSCORE and STS score (Logistic EuroSCORE, 27.3 ± 14% vs 13.9 ± 8.4%, respectively; P<.001) (STS score, 8.3 ± 5.2% vs 4.8 ± 2.8%, respectively; P<.001). Furthermore, patients in the 3rd tertile had a 3 to 4-fold higher frequency of atrial fibrillation than patients in the 1st tertile (32% vs 9.6%, respectively, P<.001). There were no significant differences in 30-day mortality (P=.84) and cardiac rehospitalization rate (P=.16) among the NT-proBNP tertiles but a higher 1-year mortality in the 3rd tertile (P=.024).
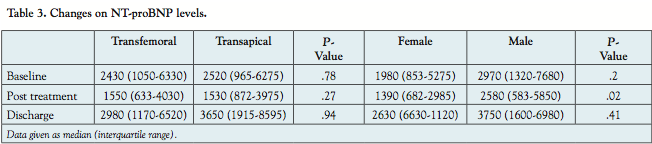 Evolution of NT-proBNP levels during hospitalization. The median baseline NT-proBNP level was 2710 ng/L (IQR, 1177-6332). NT-proBNP changes are shown in Table 3. Median NT-proBNP levels decreased by approximately 40% immediately after TAVI (baseline 2460 ng/L (IQR, 1080-6410) vs post-treatment 1550 ng/L (IQR, 681-4030; P<.001). From post-treatment to hospital discharge, median NT-proBNP levels increased from 1550 ng/L (IQR, 681-4030) to 3070 (IQR, 1270-6670 ng/L), (P<.001). There were no statistically significant differences in NT-proBNP levels between the transfemoral and transapical subgroups either at baseline or at hospital discharge. Comparing the NT-proBNP levels in men and women, men presented a higher baseline NT-proBNP than women. The post-treatment decrease in NT-proBNP is higher in females than males (P=.02).
Evolution of NT-proBNP levels during hospitalization. The median baseline NT-proBNP level was 2710 ng/L (IQR, 1177-6332). NT-proBNP changes are shown in Table 3. Median NT-proBNP levels decreased by approximately 40% immediately after TAVI (baseline 2460 ng/L (IQR, 1080-6410) vs post-treatment 1550 ng/L (IQR, 681-4030; P<.001). From post-treatment to hospital discharge, median NT-proBNP levels increased from 1550 ng/L (IQR, 681-4030) to 3070 (IQR, 1270-6670 ng/L), (P<.001). There were no statistically significant differences in NT-proBNP levels between the transfemoral and transapical subgroups either at baseline or at hospital discharge. Comparing the NT-proBNP levels in men and women, men presented a higher baseline NT-proBNP than women. The post-treatment decrease in NT-proBNP is higher in females than males (P=.02).
Thirty-day and 1-year mortality and cardiac rehospitalization Patients were followed up for a median of 1.1 (1.0-1.4) years. The 30-day and 1-year mortality rate were 7.3% and 18%, respectively. Cardiac rehospitalization for acute heart failure was observed in 28 patients (7.5%). There were no statistically significant differences in baseline NT-proBNP in those patients with and without rehospitalization (1590 [671-5410] ng/L vs 2455 [1197-6432] ng/L; P=.28).
 Kaplan Meier survival analyses stratified according to tertile NT-proBNP levels at baseline and post-treatment are shown in Figure 2. The survival rates after 12 months were 88.5%, 77.1%, and 77.7% among the 1st, 2nd, and 3rd tertile, respectively.
Kaplan Meier survival analyses stratified according to tertile NT-proBNP levels at baseline and post-treatment are shown in Figure 2. The survival rates after 12 months were 88.5%, 77.1%, and 77.7% among the 1st, 2nd, and 3rd tertile, respectively.
In the 30-day mortality, there was no significant difference between the baseline and post-treatment NT-proBNP tertiles (Figures 2A and 2C). In the 1-year mortality however, there was a significant difference in the 1-year mortality in baseline and post-treatment NT-proBNP tertiles (Figures 2D and 2B).
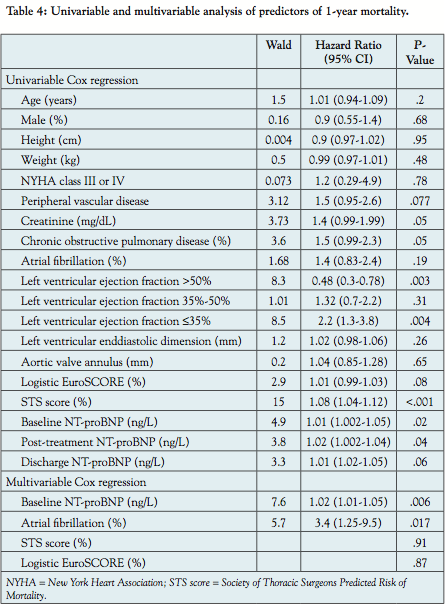 Predictors of 1-year mortality. Table 4 summarizes predictors for 1-year mortality. In the univariable analysis: age, gender, NYHA class, chronic obstructive pulmonary disease (COPD), left ventricular ejection fraction, left ventricular end-diastolic dimension, peripheral vascular disease, creatinine level, atrial fibrillation, logistic EuroSCORE, STS Score, NT-proBNP at baseline, post-treatment, and at hospital discharge were identified as univariable predictors for mortality in patients undergoing TAVI. On multivariable analysis, only baseline NT-proBNP and atrial fibrillation remained as independent predictors for 1-year mortality (HR, 1.02; 95% CI, 1.01-1.05; P=.006 and HR, 3.4; 95% CI, 1.25-9.5; P=.017, respectively).
Predictors of 1-year mortality. Table 4 summarizes predictors for 1-year mortality. In the univariable analysis: age, gender, NYHA class, chronic obstructive pulmonary disease (COPD), left ventricular ejection fraction, left ventricular end-diastolic dimension, peripheral vascular disease, creatinine level, atrial fibrillation, logistic EuroSCORE, STS Score, NT-proBNP at baseline, post-treatment, and at hospital discharge were identified as univariable predictors for mortality in patients undergoing TAVI. On multivariable analysis, only baseline NT-proBNP and atrial fibrillation remained as independent predictors for 1-year mortality (HR, 1.02; 95% CI, 1.01-1.05; P=.006 and HR, 3.4; 95% CI, 1.25-9.5; P=.017, respectively).
Discussion
In the present study, the median baseline NT-proBNP was 2710 ng/L (IQR, 1177-6332) and BNP tertiles were identified as ≤1570 ng/L, 1571 to 4690 ng/L and ≥4691 ng/L. The major findings of this study were:
(1) Baseline NT-proBNP tertiles correlated with patient risk profile such that patients in the last tertile were older, more symptomatic (NYHA), had higher incidence of peripheral vascular disease, left ventricular dysfunction, atrial fibrillation, higher STS and logistic EuroSCORE;
(2) Median baseline NT-proBNP levels decreased significantly after TAVI;
(3) Patients in the last NT-proBNP tertile had significantly higher 1-year mortality than patients in the first or second tertiles;
(4) Baseline NT-proBNP levels and atrial fibrillation were independent predictors of 1-year mortality.
Patients undergoing TAVI exhibited high levels of baseline NT-proBNP (median 2710 ng/L, IQR 1177-6332). Berry et al also observed high baseline levels of NT-proBNP (mean 10059 ± 12117 ng/L) in patients undergoing TAVI.9 On the other hand, patients undergoing surgical aortic valve replacement typically have lower baseline NT-proBNP levels (mean values ranging from 157 to 623 ng/L.10-12 These differences in NT-proBNP levels can be explained by the patient’s baseline risk profile.
Very few previous studies on TAVI have reported data on the BNP changes after TAVI. Sherif et el compared early hemodynamic and neurohormonal changes in surgical aortic valve replacement (SAVR) and TAVI-group,13 they found, 30 days after the implantation, a notable improvement in the LV function in patients with moderately to severely impaired LV function in TAVI patients, suggesting an earlier reverse cardiac remodeling process.
Our data confirm the association between NT-proBNP levels and aortic valve stenosis severity, and preoperative ejection fraction as reported in previous studies.2,11,14 Similarly, other studies have demonstrated the correlation between NT-proBNP levels and transvalvular aortic pressure gradients.15,16 This is not surprising given the fact that secretion of NT-proBNP is induced by left ventricular overload and extent left ventricular hypertrophy.
In severe aortic stenosis, the impact of surgical aortic valve replacement on BNP levels is controversial. Several studies have demonstrated up to a 25% decrease in BNP levels after SAVR or balloon valvuloplasty (BAV).7,17 In the present study, NT-proBNP levels were measured preoperatively, post-treatment and at discharge. Patients undergoing transapical implantation had a more distinct, through not significant decrease than those undergoing transfemoral implantation, and females had a significantly more distinct decrease than males. There was a significant decrease in NT-proBNP levels immediately after the TAVI procedure likely a reflection of lower transventricular pressures. Interestingly, we observed that NT-proBNP levels increased non-significantly prior to hospital discharge. We agree with other investigators who believe, this is a result of anesthetic effects surrounding the periprocedural period16 or as response of new-onset atrial fibrillation.18 Other possible explanation of the NT-proBNP increase were postprocedural right ventricular pacing during the implantation.
In SAVR, Qi et al19 found no significant decrease of NT-proBNP 4 and 12 months after the procedure. Similarly to this finding, Sherif et al13 observed no significant differences in NT-proBNP levels 30 days after SAVR, in the TAVI group, however, they demonstrated a significant decrease in NT-proBNP in patients with normal or impaired left ventricular function. Another possible explanation is the post-implant aortic regurgitation. Future studies are certainly needed to assess the impact of aortic regurgitation on NT-proBNP levels after TAVI.
Recently, Kefer et al20 found that both baseline and 24 hours post-treatment BNP were strong predictors of 30-day mortality in patients undergoing TAVI. In contrast, the present study did not find any association between NT-proBNP levels and 30-day mortality. Instead, we observed an association between NT-proBNP levels and 1-year mortality. These observations may indicate that the hemodynamic status of the ventricle influences long-term survival.
Several other studies have described the prognostic value of NT-proBNP in patients undergoing surgical aortic valve replacement and patients with aortic stenosis treated conservatively.3,12,21 In one study, Bergler-Klein et al demonstrated the prognostic value of BNP in 130 patients with aortic valve stenosis during an average follow-up of 377 days. Their results demonstrated that NT-proBNP provides important prognostic information and independently predicts symptom-free survival, outcome, and left ventricular function.2
Other factors influencing NT-proBNP levels are important to mention. It is well established that NT-proBNP correlated with elevated pulmonary artery pressure in patients with right heat failure.22 Patients with aortic stenosis and diastolic dysfunction presented a higher NT-proBNP levels and this correlated with poor prognosis.23 Furthermore, female patients may have a higher NT-proBNP levels.24 NT-proBNP is influenced by other comorbidities such as advanced age, obesity,25 and sleep apnea as well.
Recent studies investigate the impact of atrial fibrillation on outcomes of patients following TAVI. New-onset atrial fibrillation was seen in one-third of all patients undergoing TAVI but was not associated with higher 30-day or 1-year mortality.26 Having said that, B-type natriuretic peptide level is increased in patients with atrial fibrillation.27
Study limitations. Although we enrolled a total of 373 TAVI patients, subgroup analyses into NT-proBNP tertiles resulted in relatively small sample sized cohorts. Thus, our results may be viewed as hypothesis generating with larger studies needing to prove the prognostic value of BNP in patients undergoing TAVI. Other confounders of this study are noteworthy. NT-proBNP levels could be higher in patients developing acute kidney injury.
Conclusion
The results of this study suggest an association between baseline NT-proBNP levels and 1-year mortality in patients undergoing TAVI. This information may prove useful in the risk stratification of patients following TAVI and should be considered as a biomarker in future risk stratification models.
References
- Dickstein K. ESC guidelines for the diagnosis and treatment of acute and chronic heart failure 2008: application of natriuretic peptides. Reply. Eur Heart J. Epub 2008 Dec 24.
- Bergler-Klein J, Klaar U, Heger M, et al. Natriuretic peptides predict symptom-free survival and postoperative outcome in severe aortic stenosis. Circulation. 2004;109(19):2302-2308.
- Patel DN, Bailey SR. Role of BNP in patients with severe asymptomatic aortic stenosis. Eur Heart J. 2004;25(22):1972-1973.
- Weber M, Arnold R, Rau M, et al. Relation of N-terminal pro B-type natriuretic peptide to progression of aortic valve disease. Eur Heart J. 2005;26(10):1023-1030.
- Nozohoor S, Nilsson J, Luhrs C, Roijer A, Algotsson L, Sjogren J. B-type natriuretic peptide as a predictor of postoperative heart failure after aortic valve replacement. J Cardiothorac Vasc Anesth. 2009;23(2):161-165.
- Kolh P, Lahaye L, Gerard P, Limet R. Aortic valve replacement in the octogenarians: perioperative outcome and clinical follow-up. Eur J Cardiothorac Surg. 1999;16(1):68-73.
- Spargias K, Alexopoulos E, Thomopoulou S, et al. Effect of balloon valvuloplasty in patients with severe aortic stenosis on levels of N-terminal pro-B-type natriuretic peptide. Am J Cardiol. 2009;104(6):846-849.
- Bleiziffer S, Ruge H, Horer J, et al. Predictors for new-onset complete heart block after transcatheter aortic valve implantation. JACC Cardiovasc Interv. 2010;3(5):524-530.
- Berry C, Asgar A, Lamarche Y, et al. Novel therapeutic aspects of percutaneous aortic valve replacement with the 21F CoreValve Revalving System. Catheter Cardiovasc Interv. 2007;70(4):610-616.
- Berger R, Stanek B, Frey B, et al. B-type natriuretic peptides (BNP and PRO-BNP) predict longterm survival in patients with advanced heart failure treated with atenolol. J Heart Lung Transplant. 2001;20(2):251.
- Pedrazzini GB, Masson S, Latini R, et al. Comparison of brain natriuretic peptide plasma levels versus logistic EuroSCORE in predicting in-hospital and late postoperative mortality in patients undergoing aortic valve replacement for symptomatic aortic stenosis. Am J Cardiol. 2008;102(6):749-754.
- Weber M, Hausen M, Arnold R, et al. Prognostic value of N-terminal pro-B-type natriuretic peptide for conservatively and surgically treated patients with aortic valve stenosis. Heart. 2006;92(11):1639-1644.
- Sherif MA, Abdel-Wahab M, Awad O, et al. Early hemodynamic and neurohormonal response after transcatheter aortic valve implantation. Am Heart J. 2010;160(5):862-869.
- Bergler-Klein J, Mundigler G, Pibarot P, et al. B-type natriuretic peptide in low-flow, low-gradient aortic stenosis: relationship to hemodynamics and clinical outcome: results from the Multicenter Truly or Pseudo-Severe Aortic Stenosis (TOPAS) study. Circulation. 2007;115(22):2848-2855.
- Neverdal NO, Knudsen CW, Husebye T, et al. The effect of aortic valve replacement on plasma B-type natriuretic peptide in patients with severe aortic stenosis — one year follow-up. Eur J Heart Fail. 2006;8(3):257-262.
- Georges A, Forestier F, Valli N, Plogin A, Janvier G, Bordenave L. Changes in type B natriuretic peptide (BNP) concentrations during cardiac valve replacement. Eur J Cardiothorac Surg. 2004;25(6):941-945.
- Qi W, Mathisen P, Kjekshus J, et al. Natriuretic peptides in patients with aortic stenosis. Am Heart J. 2001;142(4):725-732.
- Yamada T, Murakami Y, Okada T, et al. Plasma atrial natriuretic peptide and brain natriuretic peptide levels after radiofrequency catheter ablation of atrial fibrillation. Am J Cardiol. 2006;97(12):1741-1744.
- Qi W, Mathisen P, Kjekshus J, et al. The effect of aortic valve replacement on N-terminal natriuretic propeptides in patients with aortic stenosis. Clin Cardiol. 2002;25(4):174-180.
- Kefer J, Beauloye C, Astarci P, et al. Usefulness of B-type natriuretic peptide to predict outcome of patients treated by transcatheter aortic valve implantation. Am J Cardiol. 2010;106(12):1782-1786. Epub 2010 Nov 3.
- Gerber IL, Stewart RA, Legget ME, et al. Increased plasma natriuretic peptide levels reflect symptom onset in aortic stenosis. Circulation. 2003;107(14):1884-1890.
- Daniels LB, Maisel AS. Natriuretic peptides. J Am Coll Cardiol. 2007;50(25):2357-2368.
- Iwanaga Y, Nishi I, Furuichi S, et al. B-type natriuretic peptide strongly reflects diastolic wall stress in patients with chronic heart failure: comparison between systolic and diastolic heart failure. J Am Coll Cardiol. 2006;47(4):742-748.
- Weber M, Arnold R, Rau M, et al. Relation of N-terminal pro-B-type natriuretic peptide to severity of valvular aortic stenosis. Am J Cardiol. 2004;94(6):740-745.
- Batal O, Faulx M, Krasuski RA, et al. Effect of obesity on B-type natriuretic peptide levels in patients with pulmonary arterial hypertension. Am J Cardiol. 2012;110(6):909-914. Epub 2012 Jun 7.
- Tay EL, Gurvitch R, Wijesinghe N, et al. A high-risk period for cerebrovascular events exists after transcatheter aortic valve implantation. JACC Cardiovasc Interv. 2011;4(12):1290-1297.
- Hussein AA, Saliba WI, Martin DO, et al. Plasma B-type natriuretic peptide levels and recurrent arrhythmia after successful ablation of lone atrial fibrillation. Circulation. 2011;123(19):2077-2082.
_____________________________________________
Disclosure: The authors have completed and returned the ICMJE Form for Disclosure of Potential Conflicts of Interest. The authors report no conflicts of interest regarding the content herein.
Manuscript submitted June 19, 2012, provisional acceptance given July 13, 2012, final version accepted July 26, 2012.
Address for correspondence: Elhmidi Yacine, MD, Lazarettestrasse 36, 80636, Munich, Germany. Email: elhmidi@dhm.mhn.de



