

Coronary Artery Bypass Surgery Compared With Percutaneous Coronary Intervention for Proximal Left Anterior Descending Artery Treatment in Patients With Acute Coronary Syndrome: Analysis From the ACUITY Trial
Abstract: Background. The optimal revascularization strategy in patients with acute coronary syndrome (ACS) and proximal left anterior descending (pLAD) coronary artery lesions is not well defined. The aim of this study was to compare the outcomes of ACS patients with pLAD culprit lesions receiving percutaneous coronary intervention (PCI) vs coronary artery bypass graft (CABG). Methods. The ACUITY trial was a multicenter, prospective trial of patients with ACS treated with an early invasive strategy. Major adverse cardiac event (MACE; defined as death, myocardial infarction [MI], and repeat revascularization) and stroke were compared at 30 days and 1 year between PCI and CABG in patients with significant stenosis of the pLAD undergoing revascularization. Postprocedural major bleeding was evaluated at 30 days. Results. Among patients with a significant pLAD stenosis (n = 842), a total of 562 (66.7%) underwent PCI and 280 (33.3%) underwent CABG. Baseline characteristics, including age, sex, diabetes, and TIMI risk score, were well matched between groups; however, patients undergoing PCI were more likely to have had previous CABG (21.9% vs 6.4%; P<.001). Death, MI, MACE, and stroke rates did not differ between groups at 1 year. PCI patients had lower bleeding rates (8.1% vs 52.4%; P<.001) and blood product transfusion at 30 days (4.5% vs 41.3%; P<.001), but higher rates of unplanned revascularization at 1 year (12.7% vs 5.2%; P<.01). These results were consistent in patients with single vs multivessel disease and in diabetics vs non-diabetics. Conclusions. Among ACS patients with pLAD culprit lesions, an initial revascularization strategy of PCI compared with CABG yields similar 1-year death, MI, and MACE rates, although unplanned revascularization is more common after PCI.
J INVASIVE CARDIOL 2015;27(10):468-473. Epub 2015 June 15
Key words: acute coronary syndromes, percutaneous coronary intervention
_____________________________________________
The proximal segment of the left anterior descending (pLAD) coronary artery is involved in as many as 15% of patients presenting with acute coronary syndrome (ACS)1 and is associated with worse prognosis.2,3 Moreover, the optimal revascularization strategy between percutaneous coronary intervention (PCI) and coronary artery bypass graft (CABG) surgery in the acute setting is not well defined. Previous studies have shown PCI to be a valid alternative to surgical revascularization in patients with a pLAD lesion;4-6 however, the majority of retrospective studies and all recent randomized studies comparing CABG and PCI have been performed in stable patients.7-9 Consequently, there is a lack of published literature specific to this subset of ACS patients, and the guidelines do not clearly state which strategy should be adopted, referring instead to the recommendation for patients with stable coronary artery disease (CAD).10,11 Historical studies have shown a 3-year survival benefit in pLAD disease treated with surgical revascularization vs angioplasty or bare-metal stenting.12,13 More recently, with the introduction of drug-eluting stent (DES) use, the studies report conflicting results in long-term survival.14,15 We have previously reported a relative advantage of PCI over CABG in the ACS setting with respect to stroke, myocardial infarction (MI), and bleeding;16 however, whether this treatment benefit also applies to pLAD lesions remains uncertain. Therefore, the aim of this study was to compare the outcomes of ACS patients with a pLAD lesion managed with either percutaneous or surgical revascularization.
Methods
The Acute Catheterization and Urgent Intervention Triage Strategy (ACUITY) trial design has been previously described.17 In brief, ACUITY was a prospective, open-label, randomized, multicenter trial of patients with non-ST segment elevation ACS treated with an early invasive strategy. Patients were randomized to receive heparin with a glycoprotein (GP) IIb/IIIa inhibitor, bivalirudin plus a GP IIb/IIIa inhibitor, or bivalirudin alone. Coronary angiography was performed in all patients within 72 hours of randomization with subsequent triage to percutaneous, surgical, or medical management according to investigator discretion. Stent type was determined by operator discretion and resulted in approximately 85% DES use in the PCI population, all of which were paclitaxel-eluting and sirolimus-eluting stents.
Before surgery, a 5-day clopidogrel wash-out was recommended. All patients received unfractionated heparin during CABG with dosing per standard institutional practice. After hospital discharge, aspirin was recommended indefinitely to all patients, while clopidogrel was recommended for at least 1 year in PCI patients and at physician discretion in CABG patients.
Endpoints and definitions. The study endpoints have been previously reported.17 In brief, major adverse cardiac event (MACE) was defined as death from any cause, MI, or unplanned revascularization. Post-PCI MI was assessed as any CPK-MB increasing to ≥3x normal within 24 hours after the PCI or ≥1x normal with the occurrence of new, significant (≥0.04 seconds) Q-waves in 2 or more anatomically contiguous electrocardiographic leads. Post-CABG MI was assessed as any CPK-MB increasing to ≥10x normal within 24 hours of the procedure or to ≥5x normal with the occurrence of new, significant Q-waves in 2 or more contiguous electrocardiographic leads. Major bleeding was defined as intracranial or intraocular bleeding, access-site hemorrhage requiring intervention, ≥5 cm diameter hematoma, reduction in hemoglobin ≥4 g/dL without or ≥3 g/dL with an overt bleeding source, reoperation for bleeding, or blood product transfusion. The events were assessed at 30 days and 1 year by an independent clinical events committee blinded to treatment.
In this subanalysis of the ACUITY trial, we compared the outcomes of patients undergoing PCI or CABG for the treatment of pLAD disease. An angiographic core laboratory performed the quantitative coronary analysis in 6921 consecutive patients as an angiographic subgroup of the study. Coronary artery disease (CAD) was defined as the presence of epicardial vessel stenosis ≥30% by quantitative coronary analysis, approximately equivalent to a stenosis of 50% by visual estimation. The pLAD was defined as the portion of the artery prior to the origin of the first septal branch. All angiographic procedural complications were determined according to previously defined criteria.1
Statistical analysis. Summary statistics are presented as mean ± standard deviation or median (interquartile range) for continuous variables and as percentages for categorical variables. Baseline and procedural characteristics of the CABG and PCI groups were compared using chi-square or Fischer exact test for categorical variables and Kruskal-Wallis test for continuous variables. The unadjusted rate of all-cause mortality, MI, unplanned revascularization, and MACE was estimated by Kaplan-Meier event curves and the log-rank test.
Due to baseline differences in the PCI and CABG groups, we performed a Cox proportional hazard analysis, considering death, MI, new unplanned revascularization, MACE, and major bleeding as endpoints. We fitted a model adjusting for the covariates of age, gender, previous CABG, diabetes, multivessel CAD, baseline elevated cardiac biomarkers, and low left ventricular ejection fraction (<35%). We also evaluated the outcomes by stratifying our population according to the presence of multivessel disease and diabetes mellitus.
Results
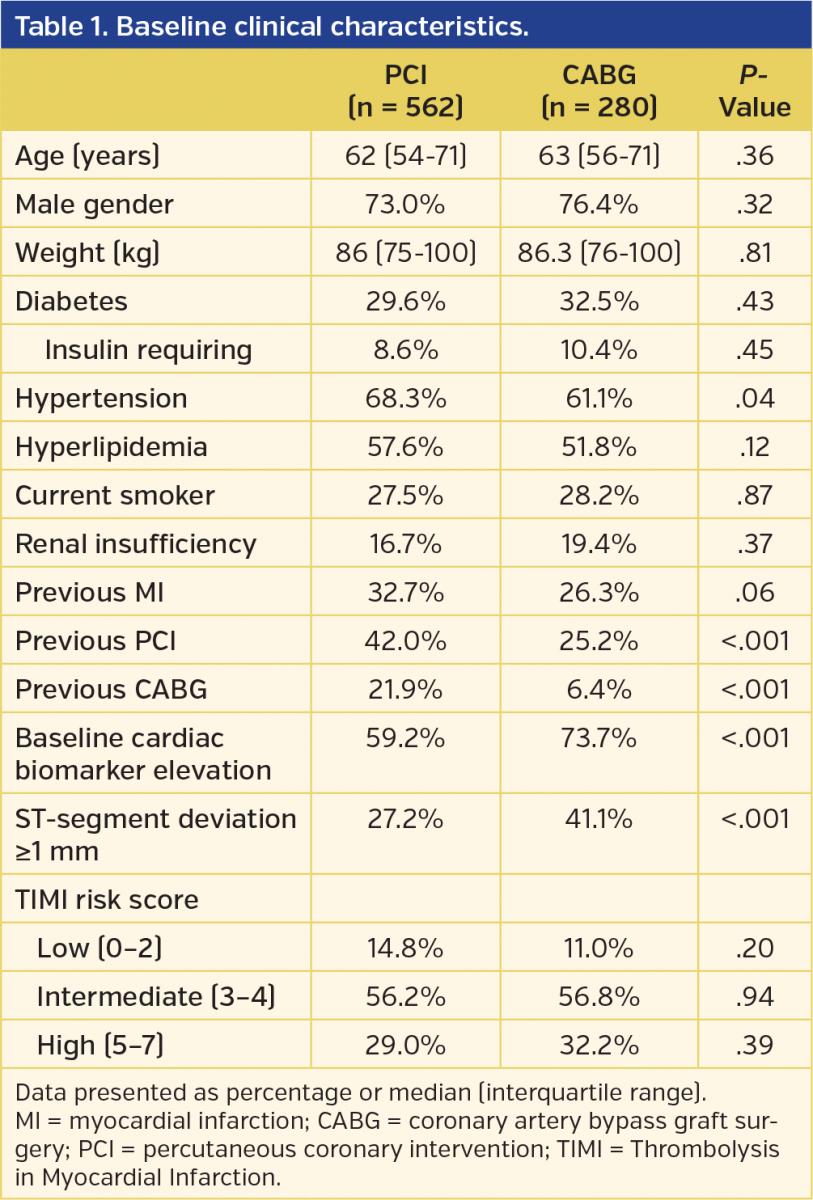
Among 13,819 moderate-risk and high-risk ACS patients enrolled in the ACUITY trial, a group of 6921 consecutive patients were included in the ACUITY angiographic substudy.Of these patients, a total of 4581 underwent revascularization: 3826 (83.5%) with PCI and 755 (16.5%) with CABG. Among these, we identified 842 patients presenting with a pLAD culprit lesion. Revascularization was performed with PCI in 562 patients (66.7%) and CABG in 280 patients (33.3%). Baseline characteristics of the two groups are shown in Table 1. PCI patients were less likely to present with ST-segment deviation (27.2% vs 41.1%; P<.001) and elevated serum cardiac necrosis markers (59.2% vs 73.7%; P<.001). PCI patients were also more likely to have a history of previous CABG (21.9% vs 6.4%; P<.001).
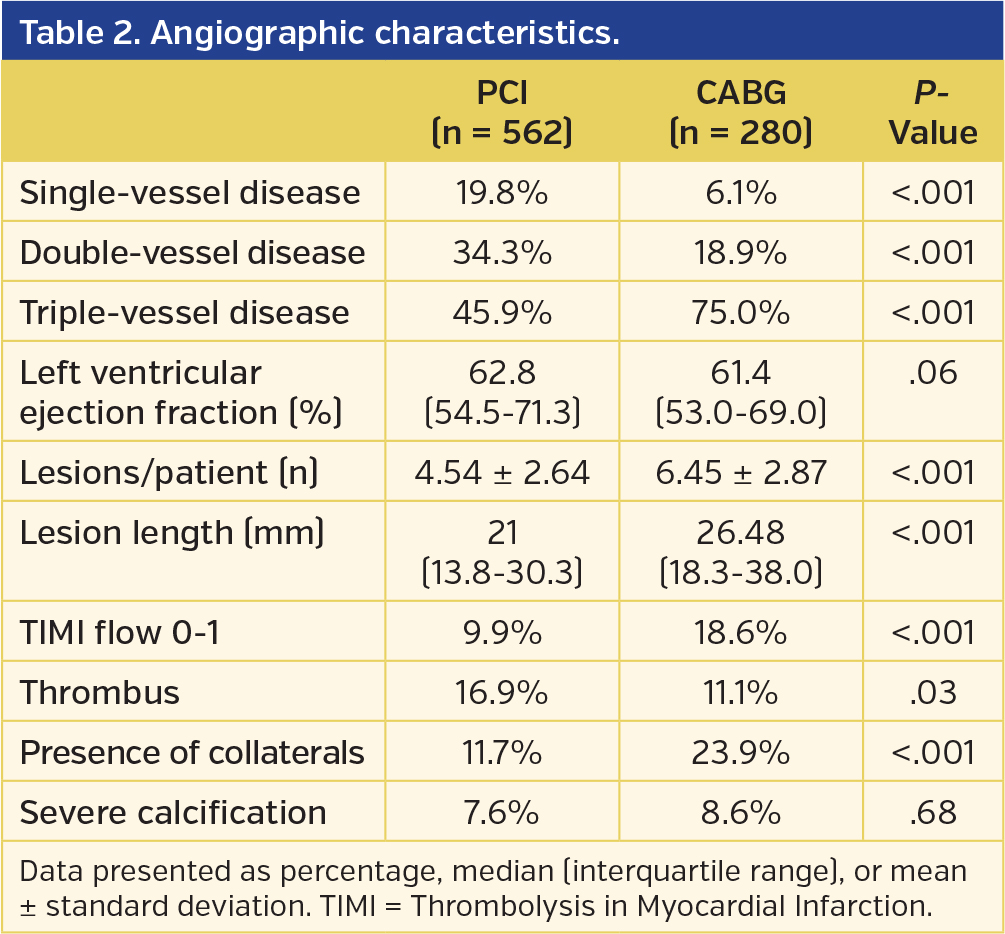
Table 2 presents the angiographic characteristics.The PCI patients were more likely to present with single-vessel disease (19.8% vs 6.1%; P<.001) and thrombotic lesions (16.9% vs 11.1%; P=.03), whereas CABG patients more often presented with TIMI flow 0-1 (18.6% vs 9.9%; P<.001) and collateralized vessel flow (23.9% vs 11.7%; P<.001). Revascularization occurred later in CABG patients vs PCI patients (median time from first anticoagulant to revascularization, 43 hours [range, 23-81 hours] vs 4 hours [range, 1-17 hours], respectively; P<.001).
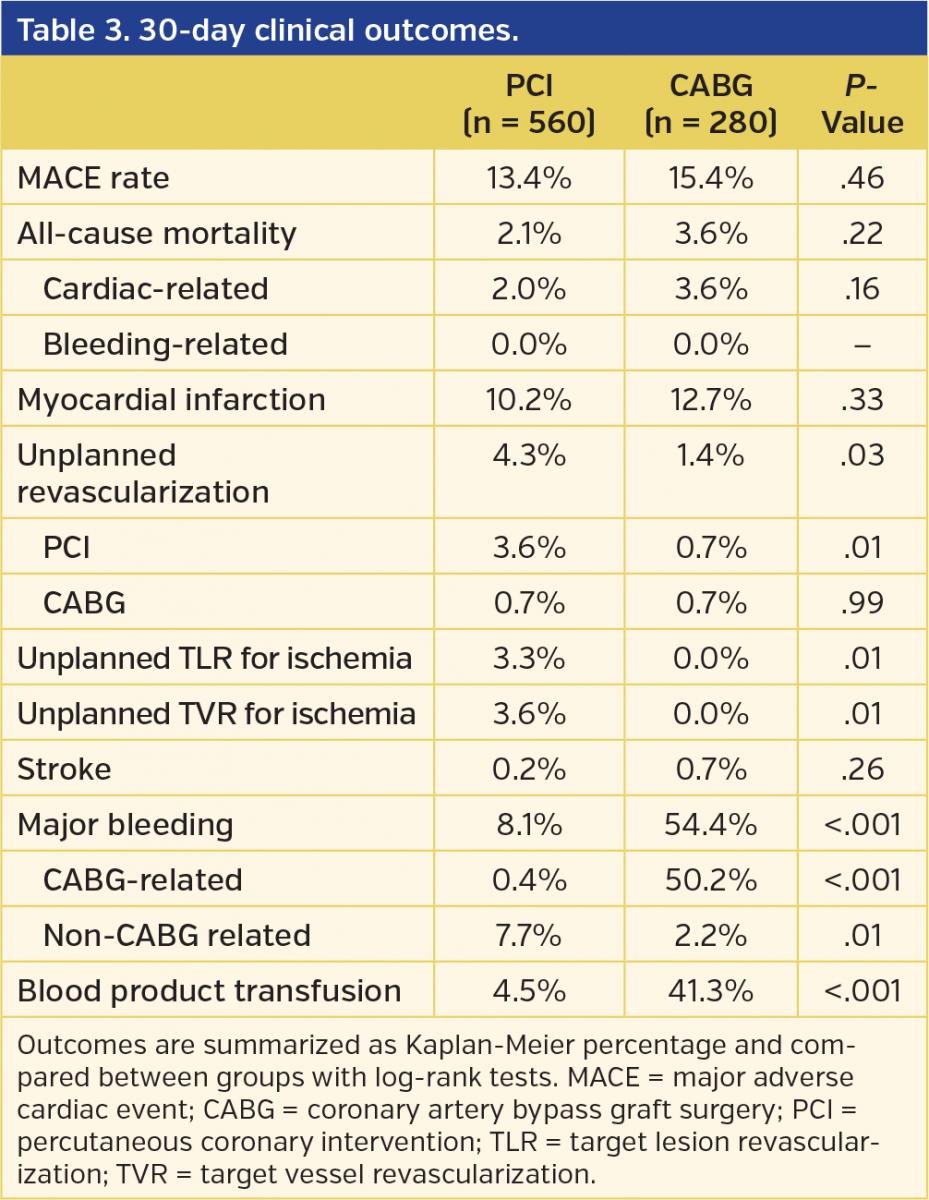
PCI and CABG patients had similar rates of death, MI, MACE, and stroke, but PCI patients had increased revascularization rates at 1 month and 1 year, which was mainly driven by target lesion failure (Tables 3 and 4; Figure 1).

Multivariate analysis demonstrated no significant difference between PCI and CABG at 1 year for death (adjusted hazard ratio [HR], 0.90; 95% confidence interval [CI], 0.35-2.32; P=.83), MI (adjusted HR, 0.87; 95% CI, 0.57-1.31; P=.50),MACE (adjusted HR, 0.96; 95% CI, 0.69-1.33; P=.79), or stroke (adjusted HR, 0.25; 95% CI, 0.02-2.71; P=.25); however, PCI remained significantly associated with major bleeding at 30 days (adjusted HR, 0.13; 95% CI, 0.09-0.18; P<.001) and unplanned revascularization at 1 year (adjusted HR, 2.18; 95% CI, 1.21-3.93; P<.001).
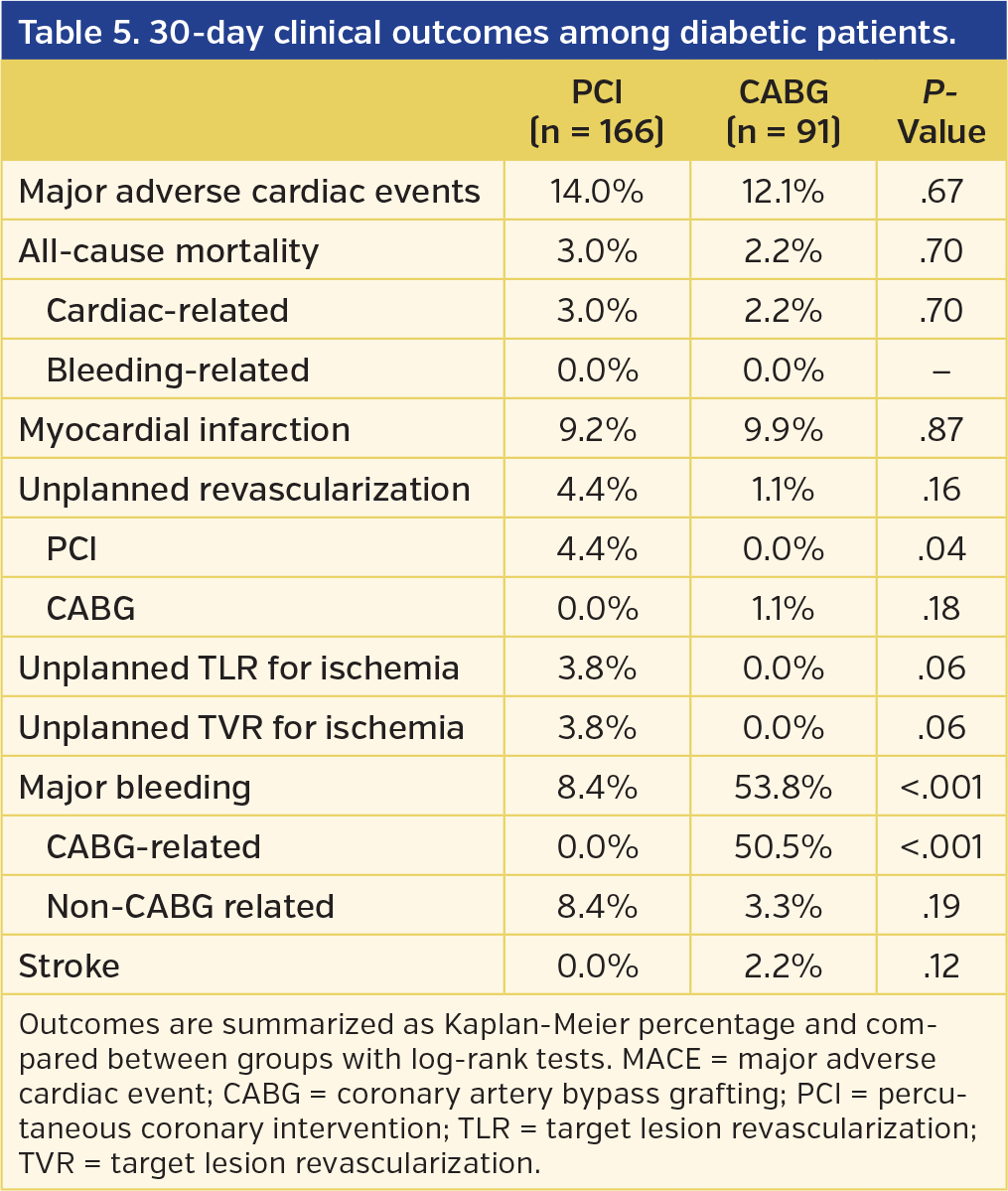
Among diabetics, we observed non-significant differences in adverse events at 30 days, while MACE rates were higher at 1 year in the PCI arm (28.5% vs 15.4%; P=.02), driven by a higher rate of unplanned revascularization (18.9% vs 6.8%; P=.01) (Tables 5 and 6).Similarly, we saw no significant difference in terms of adverse events in a dedicated analysis of patients with multivessel disease (Figure 2). Formal interaction testing between the main effects of diabetes or multivessel disease and revascularization approach was non-significant for all endpoints (Pint>.10).
Discussion
The present study of ACS patients with pLAD involvement demonstrates substantial differences in the clinical and angiographic profiles of patients treated with percutaneous vs surgical approach in this setting, consistent with contemporary trends toward surgical revascularization among patients with more diffuse or complex CAD, although left ventricular function and clinical characteristics were remarkably similar. While we detected no differences in 30-day or 1-year survival between groups, CABG was associated with a substantially lower repeat revascularization rate and a higher bleeding rate. Postprocedural stroke was numerically, albeit non-significantly, higher among those undergoing CABG. Results were unchanged after multivariable adjustment and remained consistent among those with diabetes or multivessel disease.

Existing studies that inform clinical decision-making and contemporary guidelines for the optimal revascularization approach (CABG vs PCI) in patients with CAD are largely based on comparative studies involving stable patient populations. Patients with more diffuse or complex coronary atherosclerosis derive a benefit from surgical revascularization based on results from the Future Revascularization Evaluation in Patients with Diabetes Mellitus: Optimal Management of Multivessel Disease (FREEDOM)9 and Synergy Between PCI with Taxus and Cardiac Surgery (SYNTAX)8 trials. Consistent with these randomized results, we found in this subgroup analysis that patients with more extensive or complex CAD were selected for CABG. In fact, major clinical risk factors, such as age, sex, and diabetes mellitus did not vary between groups while angiographic parameters including extent of disease and lesion length were significantly different. These findings suggest that angiographic, rather than clinical, markers may be more important determinants of revascularization choice among patients with ACS and concomitant pLAD involvement.

Given the lack of data regarding the comparative efficacy of CABG vs PCI among such patients, we also compared 30-day and 1-year outcomes between groups. Although many studies have reported a survival benefit in pLAD disease treated with surgical revascularization compared with PCI, these analyses were performed in a historical cohort of patients treated with angioplasty only or bare-metal stenting.12,13 In contrast, most recent trials using DES implantation report conflicting results in long-term survival when the pLAD is involved.14,15 Similarly, the 5-year outcome analysis of the SYNTAX trial8 recently reported no significant survival benefit for the surgical arms. However, this trial included only 30% patients with unstable angina, and thus our findings add evidence that might inform clinical decision-making vis a vis revascularization strategy in the setting of moderate to high-risk ACS. Specifically, we found a substantial advantage for CABG in reducing repeat revascularization, consistent with previous comparisons of CABG vs PCI. In terms of mortality and composite events rates, however, our findings show no significant differences in CABG vs PCI at 1 year. This result is consistent with the findings of a meta-analysis of 8000 patients.7 It is important to note, however, that the modest sample size and 1-year endpoint of our analysis may have introduced the possibility of a type-II error, rendering our findings with respect to clinical outcomes hypothesis-generating rather than a definitive result, particularly in the diabetic cohort.

Study limitations. Our PCI population was treated exclusively with either first-generation DES or bare-metal stents. These stent platforms have been superseded by second-generation DESs, which have shown lower revascularization rates in the setting of ACS.18,19 Currently, second-generation DESs are being tested in randomized trials comparing PCI vs CABG.20,21 Furthermore, this was not a prespecified subanalysis of the ACUITY trial. For this reason, the study might be underpowered to detect differences in the treatment groups, and multivariable analysis does not adjust for all residual confounding factors (eg, frailty). In addition, the follow-up period of 1 year might be insufficient to detect an outcome difference in the long term, as treatment arms in the FREEDOM trial only started to diverge after the first year.9 Nonetheless, these data come from a large randomized trial with an angiographic core lab and all events adjudicated by a clinical events committee, blinded to treatment assignment.
Conclusion
In patients with ACS attributable to the pLAD, the method of revascularization (PCI vs CABG) does not influence 1-year mortality. The only significant difference between strategies derived from the increased rate of repeat revascularization after PCI, driven primarily by target lesion failure. While larger studies are needed to confirm these findings, our results indicate that PCI is a safe initial revascularization strategy in ACS patients with appropriate anatomy undergoing pLAD revascularization.
References
1. Aoki J, Lansky AJ, Mehran R, et al. Early stent thrombosis in patients with acute coronary syndromes treated with drug-eluting and bare-metal stents: the Acute Catheterization and Urgent Intervention Triage Strategy trial. Circulation. 2009;119:687-698.
2. Mahmarian JJ, Pratt CM, Boyce TM, Verani MS. The variable extent of jeopardized myocardium in patients with single vessel coronary artery disease: quantification by thallium-201 single photon emission computed tomography. J Am Coll Cardiol. 1991;17:355-362.
3. Taylor GJ, Humphries JO, Mellits ED, et al. Predictors of clinical course, coronary anatomy and left ventricular function after recovery from acute myocardial infarction. Circulation. 1980;62:960-970.
4. Sawhney N, Moses JW, Leon MB, et al. Treatment of left anterior descending coronary artery disease with sirolimus-eluting stents. Circulation. 2004;110:374-379.
5. Dangas G, Ellis SG, Shlofmitz R, et al. Outcomes of paclitaxel-eluting stent implantation in patients with stenosis of the left anterior descending coronary artery. J Am Coll Cardiol. 2005;45:1186-1192.
6. Monteiro P; Portuguese Registry on Acute Coronary Syndromes. Impact of early coronary artery bypass graft in an unselected acute coronary syndrome patient population. Circulation. 2006;114:I467-I472.
7. Hlatky MA, Boothroyd DB, Bravata DM, et al. Coronary artery bypass surgery compared with percutaneous coronary interventions for multivessel disease: a collaborative analysis of individual patient data from ten randomised trials. Lancet. 2009;373:1190-1197.
8. Mohr FW, Morice MC, Kappetein AP, et al. Coronary artery bypass graft surgery versus percutaneous coronary intervention in patients with three-vessel disease and left main coronary disease: 5-year follow-up of the randomised, clinical SYNTAX trial. Lancet. 2013;381:629-638.
9. Farkouh ME, Domanski M, Sleeper LA, et al. Strategies for multivessel revascularization in patients with diabetes. N Engl J Med. 2012;367:2375-2384.
10. Hamm CW, Bassand JP, Agewall S, et al. ESC guidelines for the management of acute coronary syndromes in patients presenting without persistent ST-segment elevation: the task force for the management of acute coronary syndromes (ACS) in patients presenting without persistent ST-segment elevation of the European Society of Cardiology (ESC). Eur Heart J. 2011;32:2999-3054.
11. Anderson JL, Adams CD, Antman EM, et al. 2012 ACCF/AHA focused update incorporated into the ACCF/AHA 2007 guidelines for the management of patients with unstable angina/non-ST-elevation myocardial infarction: a report of the American College of Cardiology Foundation/American Heart Association Task Force on Practice Guidelines. J Am Coll Cardiol. 2013;61:e179-e347.
12. Hannan EL, Racz MJ, McCallister BD, et al. A comparison of three-year survival after coronary artery bypass graft surgery and percutaneous transluminal coronary angioplasty. J Am Coll Cardiol. 1999;33:63-72.
13. Hannan EL, Racz MJ, Walford G, et al. Long-term outcomes of coronary-artery bypass grafting versus stent implantation. N Engl J Med. 2005;352:2174-2183.
14. Kukreja N, Serruys PW, De Bruyne B, et al. Sirolimus-eluting stents, bare-metal stents or coronary artery bypass grafting for patients with multivessel disease including involvement of the proximal left anterior descending artery: analysis of the Arterial Revascularization Therapies study part 2 (ARTS-II). Heart. 2009;95:1061-1066.
15. Hannan EL, Wu C, Walford G, et al. Drug-eluting stents vs coronary-artery bypass grafting in multivessel coronary disease. N Engl J Med. 2008;358:331-341.
16. Ben-Gal Y, Moses JW, Mehran R, et al. Surgical versus percutaneous revascularization for multivessel disease in patients with acute coronary syndromes: analysis from the ACUITY (Acute Catheterization and Urgent Intervention Triage Strategy) trial. JACC Cardiovasc Interv. 2010;3:1059-1067.
17. Stone GW, Bertrand M, Colombo A, et al. Acute catheterization and urgent intervention triage strategy (ACUITY) trial: study design and rationale. Am Heart J. 2004;148:764-775.
18. Kedhi E, Joesoef KS, McFadden E, et al. Second-generation everolimus-eluting and paclitaxel-eluting stents in real-life practice (COMPARE): a randomised trial. Lancet. 2010;375:201-209.
19. Jeremias A, Kaul S, Rosengart TK, Gruberg L, Brown DL. The impact of revascularization on mortality in patients with non-acute coronary artery disease. Am J Med. 2009;122:152-161.
20. Evaluation of Xience Prime everolimus-eluting stent system (EECSS) or Xience V EECSS versus coronary artery bypass surgery for effectiveness of left main revascularization (EXCEL) clinical trial. ClinicalTrials.gov identifier NCT01205776. https://clinicaltrials.gov/ct2/show/study/NCT01205776.
21. Bypass surgery versus everolimus-eluting stent implantation for multivessel coronary artery disease (BEST) clinical trial. ClinicalTrials.gov identifier NCT00997828. https://clinicaltrials.gov/ct2/show/study/NCT00997828.
___________________________________________
From the 1Icahn School of Medicine at Mount Sinai, New York, New York; 2Cardiovascular Research Foundation, New York, New York; 3Tel Aviv Sourasky Medical Center, Tel Aviv University, Tel Aviv, Israel; 4Columbia University Medical Center, New York, New York; 5Hôpital du Sacré-Coeur de Montréal, Montréal, Québec, Canada; 6New York Methodist Hospital, Brooklyn, New York; 7NYU Langone Medical Center, New York, New York; 8Cleveland Clinic Lerner College of Medicine of Case Western Reserve University, Cleveland, Ohio; 9Duke Heart Center, Durham, North Carolina; and 10University Hospital of Caen, Normandy, France.
Funding: The ACUITY trial was supported by the Medicines Company and Nycomed.
Disclosure: The authors have completed and returned the ICMJE Form for Disclosure of Potential Conflicts of Interest. Dr Dangas and Dr Mehran report institutional research grant support from The Medicines Company, Bristol-Myers Squibb/Sanofi, Eli Lilly and Company/Daiichi-Sankyo, Regado Biosciences, and STENTYS; consulting fees from Abbott Vascular, AstraZeneca, Boston Scientific, Covidien, CSL Behring, Janssen Pharmaceuticals, Maya Medical, and Merck & Co; advisory board fees from Covidien, Janssen Pharmaceuticals, Merck, and Sanofi. Dr Généreux reports speaker fees from Abbott Vascular, CSI; consultant fees from CSI. Dr Feit reports consultant fees from The Medicines Company; shareholder in Johnson and Johnson, Eli Lilly, The Medicines Company. Dr Lincoff reports grant support/research contract with AstraZeneca, Daiichi-Sankyo/Eli Lilly and Company. Dr Ohman reports grant support from Gilead Sciences, Daiichi-Sankyo/Eli Lilly and Company; consultant fees from AstraZeneca, Boehringer Ingelheim, Bristol-Myers Squibb, Gilead Sciences, Janssen Pharmaceuticals, Liposcience, The Medicines Company, Merck/Schering Plough, Pozen, Roche, Sanofi-Aventis, WebMD. Dr Hamon reports consultant fees from The Medicines Company. The remaining authors report no conflict of interest regarding the content herein.
Manuscript submitted March 10, 2015 and accepted March 13, 2015.
Address for correspondence: Roxana Mehran, MD, Icahn School of Medicine at Mount Sinai, One Gustave L. Levy Place, Box 1030, New York, NY 10029. Email: roxana.mehran@mssm.edu



