

Collateralization of an Occluded Left Internal Mammary Artery Coronary Bypass Graft
ABSTRACT: The left internal mammary artery (LIMA) is frequently utilized in coronary artery bypass grafting (CABG); adequate visualization of the LIMA bypass graft during diagnostic angiography is critical for determination of myocardial blood supply. We present a novel case of angiography via a left transradial approach demonstrating an occluded LIMA coronary bypass graft with antegrade flow maintained via a collateral branch from the ipsilateral thyrocervical trunk. Given the prevalence of LIMA use in CABG, it is critical to be aware of unusual configurations, including collateralization of a proximally occluded LIMA graft as described in this report.
J INVASIVE CARDIOL 2011;23:E181–E182
______________________________________
The left internal mammary artery (LIMA) is frequently utilized as a coronary artery bypass graft (CABG) conduit, given its superior long-term patency and enhanced survival compared to saphenous venous grafts.1 Adequate visualization of the LIMA bypass graft during diagnostic angiography is critical to determining myocardial blood supply and for identification of culprit areas of hypoperfusion. We present the novel case of an occluded LIMA coronary bypass graft with antegrade flow maintained via a collateral branch from the ipsilateral thyrocervical trunk.
 Case Report. A 75-year-old male with a history of coronary artery disease status post 2-vessel CABG 8 years prior [LIMA to middle left anterior descending (LAD) coronary artery and saphenous vein graft to the first obtuse marginal coronary artery] was referred for cardiac catheterization with a history of atypical chest discomfort and an anterior perfusion defect on adenosine sestamibi stress testing. His past medical history was notable for symptomatic bradycardia necessitating permanent pacemaker implantation, hypertension, hyperlipidemia, former nicotine abuse with a 30-plus pack-year smoking history, bilateral renal artery stenosis status post renal artery stenting, and severe aortoiliac occlusive disease status post aortobifemoral bypass. The adenosine sestamibi revealed a new perfusion defect anteriorly in the distal one-third of the ventricle and apex when compared to a study 1 year prior. Left ventricular function by gated wall motion was 48%, with a subsequent transthoracic echocardiogram demonstrating a left ventricular ejection fraction of 65% with no regional wall motion abnormalities or significant valvular abnormalities.
Case Report. A 75-year-old male with a history of coronary artery disease status post 2-vessel CABG 8 years prior [LIMA to middle left anterior descending (LAD) coronary artery and saphenous vein graft to the first obtuse marginal coronary artery] was referred for cardiac catheterization with a history of atypical chest discomfort and an anterior perfusion defect on adenosine sestamibi stress testing. His past medical history was notable for symptomatic bradycardia necessitating permanent pacemaker implantation, hypertension, hyperlipidemia, former nicotine abuse with a 30-plus pack-year smoking history, bilateral renal artery stenosis status post renal artery stenting, and severe aortoiliac occlusive disease status post aortobifemoral bypass. The adenosine sestamibi revealed a new perfusion defect anteriorly in the distal one-third of the ventricle and apex when compared to a study 1 year prior. Left ventricular function by gated wall motion was 48%, with a subsequent transthoracic echocardiogram demonstrating a left ventricular ejection fraction of 65% with no regional wall motion abnormalities or significant valvular abnormalities.
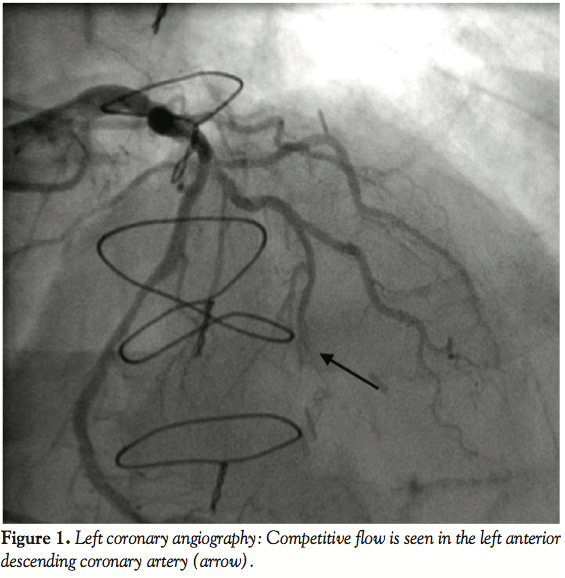
 Coronary and graft angiography was performed via left transradial approach. Native coronary angiography revealed left coronary dominance with significant obstruction of the left main coronary artery by a single discrete lesion. The LAD and circumflex arteries were patent but diseased, with the occluded first obtuse marginal branch being supplied by a patent saphenous vein graft. Notably, competitive flow was present in the mid-LAD due to filling from both the proximal native vessel and LIMA graft (Figure 1, Video 1).
Coronary and graft angiography was performed via left transradial approach. Native coronary angiography revealed left coronary dominance with significant obstruction of the left main coronary artery by a single discrete lesion. The LAD and circumflex arteries were patent but diseased, with the occluded first obtuse marginal branch being supplied by a patent saphenous vein graft. Notably, competitive flow was present in the mid-LAD due to filling from both the proximal native vessel and LIMA graft (Figure 1, Video 1).
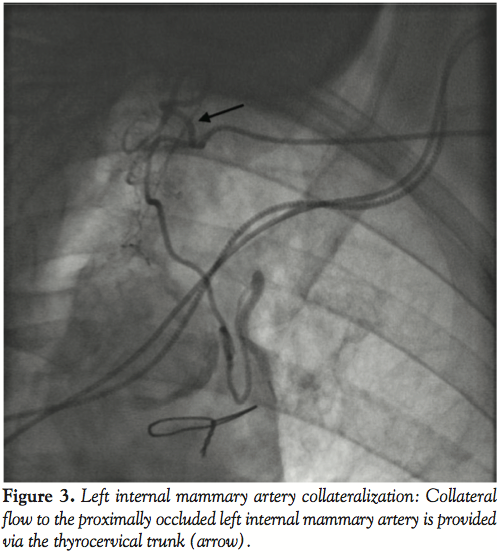 Based upon competitive flow noted during native vessel angiography, internal mammary graft patency was expected. Surprisingly, the LIMA was found to be proximally occluded (Figure 2). To reconcile the apparent discrepancy, exploration was performed for alternate sources of LAD filling. It was found that the LIMA downstream of the occluded origin filled via a single branch arising directly from the ipsilateral thyrocervical trunk (Figure 3, Video 2). The etiology of the proximal LIMA occlusion remains uncertain, but conceivably could have been related to vessel injury during coronary artery surgery. Regardless, an initial conservative strategy was felt appropriate, with the possibility of percutaneous intervention (native vessel or graft), or repeat CABG in the future, if required.
Based upon competitive flow noted during native vessel angiography, internal mammary graft patency was expected. Surprisingly, the LIMA was found to be proximally occluded (Figure 2). To reconcile the apparent discrepancy, exploration was performed for alternate sources of LAD filling. It was found that the LIMA downstream of the occluded origin filled via a single branch arising directly from the ipsilateral thyrocervical trunk (Figure 3, Video 2). The etiology of the proximal LIMA occlusion remains uncertain, but conceivably could have been related to vessel injury during coronary artery surgery. Regardless, an initial conservative strategy was felt appropriate, with the possibility of percutaneous intervention (native vessel or graft), or repeat CABG in the future, if required.
Discussion. The non-grafted LIMA can serve as a source of collateral supply to native coronary vasculature2 and peripheral arterial circulations.3 Anatomic variation in the LIMA is common, with an origin from a common stem with the thyrocervical trunk in greater than 8% of patients.4 However, external collateralization of an occluded LIMA has not been previously described. Given the prevalence of LIMA use in CABG, it is critical to be aware of unusual configurations, including collateralization of a proximally occluded LIMA graft as described in this report.
Geske Video_edited.mp4References
- Cameron A, Davis KB, Green G, Schaff HV. Coronary bypass surgery with internal-thoracic-artery grafts — Effects on survival over a 15-year period. N Engl J Med 1996;334:216–219.
- Aras D, Topaloglu S, Cagli K, et al. A rare form of communication between the left internal thoracic artery and the left anterior descending artery. J Invasive Cardiol 2006;18:E209–E210.
- Parashara DK, Kotler MN, Ledley GS, Yazdanfar S. Internal mammary artery collateral to the external iliac artery: An angiographic consideration prior to coronary bypass surgery. Cathet Cardiovasc Diagn 1994;32:343–345.
- Daseler EH, Anson BJ. Surgical anatomy of the subclavian artery and its branches. Surg Gynecol Obstet 1959;108:149–174.
______________________________________
From the Division of Cardiovascular Diseases, Mayo Clinic College of Medicine, Rochester, Minnesota.
The authors report no conflicts of interest regarding the content herein.
Manuscript submitted October 6, 2010, provisional acceptance given November 1, 2010, final version accepted January 1, 2011.
Address for correspondence: Rajiv Gulati, MD, PhD, Mayo Clinic, 200 First St. S.W., Rochester, MN 55905. Email: Gulati.Rajiv@mayo.edu



