


Tiny Tube Tricks and Trivia: Peds Cheat Sheets Are your Best Friend
By Scott DeBoer RN, MSN, CPEN, EMT-P, Lisa DeBoer NREMT-P/PI, CET, and Michael Seaver RN, BA
The human body has a variety of tubes or passages that connect the outside world to the inside world that can be subject to failure. In medical care, great attention is paid to maintaining the functioning of those tubes. We also know that the expressions “one size fits all” and “close enough” do not apply in pediatrics. To minimize both time and stress, here are some tips and tricks to help with tubes. Some are “tried and true,” while some are some new tiny tube tricks!
Starting at the Top: Tracheas
While all the tubes are important, one is of critical importance. Windpipe, airway, trachea, call it what you like, it’s just a tube. But this isn’t just any ordinary tube. It’s the tube of life itself! If this tube ceases to function properly, we have a situation that requires our immediate attention. It’s quite literally, a matter of life and death.
There are several types of artificial airways and numerous sizes of those devices, which means we must select the correct size and type. Many don’t like choices in stressful situations. But when it comes to pediatric tiny tubes, in kindergarten, children are first taught to count from one to ten. However, with critical pediatric patients, it’s even easier. You only count from one to four!
Did you know? Tracheostomies have been performed for over 4,000 years (since the 2nd century BC). Oral intubation is relatively newer, having been performed first in animals, then later in humans, since 1543.1
1x, 2x, 3x, and 4x rules
Picking the Correct Size Oral ETT: The 1x Rule

1x the endotracheal tube (ETT) is the size of the oral ETT. This is not a trick as there is only one trachea. The American Lung Association summarizes this nicely: When you can’t breathe, nothing else matters!2 Adult females tend to get a 7.5 mm oral endotracheal tube (ETT), while adult males tend to get an 8.0 mm oral ETT.3
But how do you figure out the oral ETT size for a child? If at first glance, it looks like way too big of a tube, chances are it’s way too big of a tube. This is crucial. Not only for proper patient care, but to avoid malpractice lawsuits as well. There have been several lawsuits where children had way too big of an ETT placed with subsequent long term airway issues.
Did you know? In the prehospital and emergency department settings in the United States, oral intubation is the norm. Outside of the U.S., for elective or even emergency intubations, and especially for those patients anticipated to require longer term intubation, the nasal route is commonly used. For this article and the associated tiny tube tricks, we will assume that oral endotracheal intubation is the reference point.
Newborn Oral ETT: Forget the Fancy Formulas
Imagine you’re on the scene of a newborn baby in respiratory arrest. Is this the time to figure out formulas, do division, or master the math? Probably not. Especially with a newborn!
Here’s a trick: If you know the gestational age in weeks (or even a good guess), you can pick a tube just by moving a decimal point and rounding down to the nearest size ETT available. A premature baby who is 25 weeks gestation should get a 2.5 mm oral ETT. A “32 weeker” would get a 3.0 mm ETT (because there isn’t a 3.2 mm size). A full-term baby (40 weeks) should get a 4.0 mm oral ETT. Just move the decimal one place and there’s the correct size oral ET tube. How cool is that!3,4
Pediatric Oral ETT: Cancel the Calculations, but Be Ready With References, Aids, and Apps
Formulas—Age/4+4, 16+age/4 /the mother’s date of birth; Mental math under stress is stupid. Mental math under stress with a crashing kid can result in determining a size 14 mm ETT should be used. However, there’s hopefully not a size 14 mm ETT in the jump bag or crash cart. That’s a clue that it’s probably not the right size.
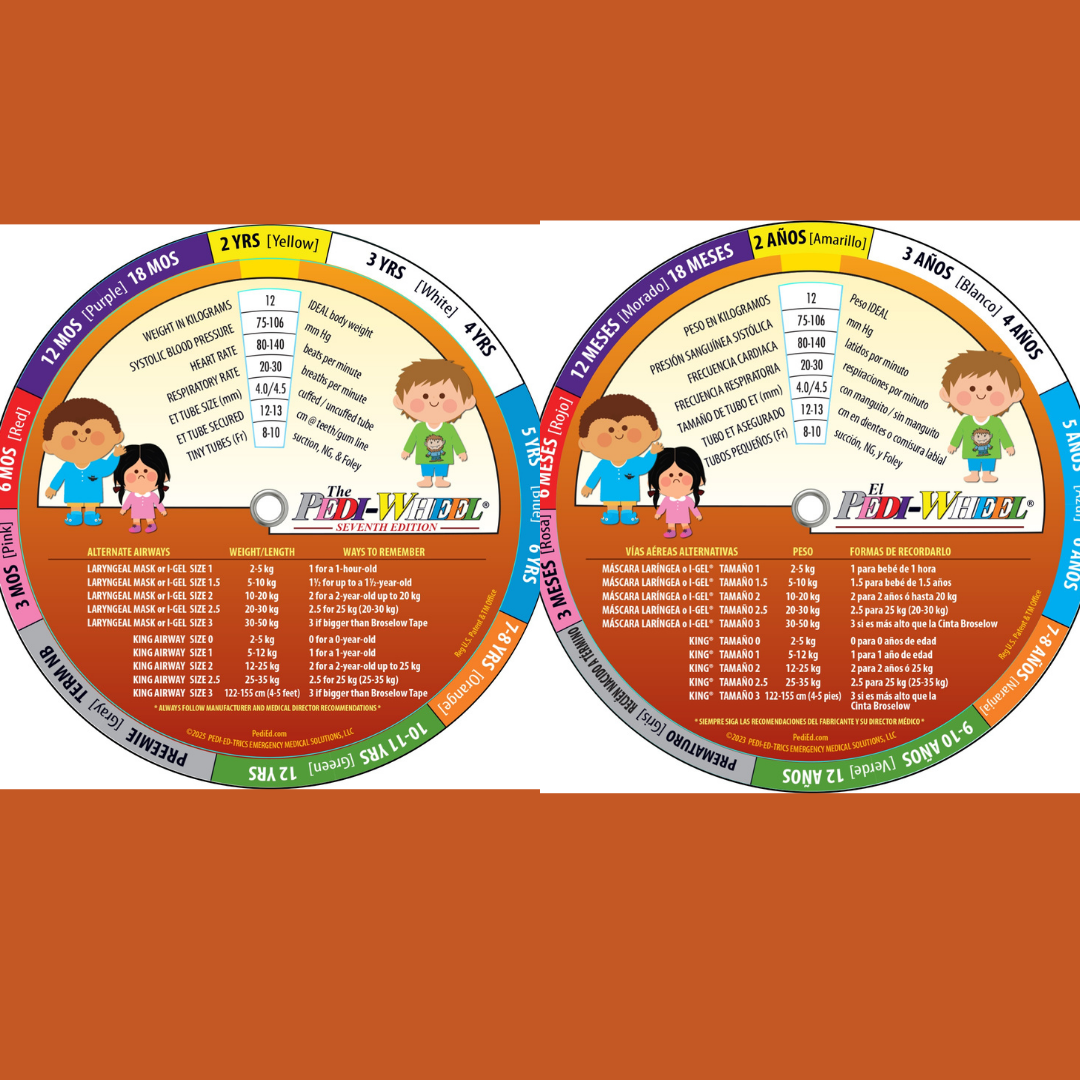
For many years providers have used various products and programs to avoid mental math. Whether hard copy or electronic, ready references and resources can replace reliance on remote recollection. In other words, memory minders are better than mental mess-ups. Yes, it’s better to read than to try to remember. Check your charts, browse your Broselow tape, preview the Pedi-Wheel, or hang onto the Handtevy app. Whatever tool or tools you choose to reduce the stress of trying to determine the right size ETT for a child, the important thing is to practice using it, so it becomes second nature when needed. As a bonus, these same references provide guidance for determining other tiny tube sizes (ETT suction catheter, NG/OG tube, Foley urinary catheter, and even chest tubes). Our suggestion is for every emergency healthcare provider, and possibly even emergency dispatchers/communication specialists as well, to have easy access to a pediatric “cheat sheet.”
Consider the Cuff When Selecting Size

When you look carefully, you will notice that each of the helpful resources shown not only indicate the appropriate oral ETT size, but also the importance of “downsizing” when utilizing cuffed endotracheal tubes. More and more providers are placing cuffed endotracheal tubes in children with excellent results. But it is essential to remember that, in a tiny airway, space is an issue. Although small tubes have small cuffs, the cuffs still take up space. So, check your preferred reference material, aka. cheat sheet. It should provide a visual reminder not only to consider the use of cuffed tubes, but also, if you are adding a cuff, “downsize” the tube size by 0.5 mm.3
Did you know? Cuffed endotracheal tubes for the smallest patients are rapidly becoming increasingly popular in the prehospital, emergency department, and pediatric ICU environments. However, uncuffed ETTs are still the norm in most neonatal ICUs.3,4
Other Tubes: The 2x Rule
If a pediatric patient has an endotracheal or tracheostomy tube, inserting secondary tubes should be second nature. We need to consider the correct size for the ETT suction catheter, NG/OG tube, and Foley urinary catheter. Fortunately, once you have the correct size for the ETT or trache you shouldn’t have to think twice about the size for the other tubes. Just pick the number (size) of the tube that is twice the number (size) for the ETT or trache. That’s what we call “the 2x rule.”
ETT Suction Catheter
2x the oral ETT size is the ETT suction catheter size. There are hopefully two lungs that you are trying to suction boogers out of, so 2x is the ETT suction catheter size. The 2x suction catheter size trick works not only for endotracheal tubes, but for traches as well.3
Except in the tiniest of sizes, such as 5 Fr, suction catheter sizes are only available in even number sizes—6 Fr, 10 Fr, etc. If the 2x rule calls for an “odd size suction catheter,” like a 9 Fr, picking the next smaller/available size, in this case an 8 Fr, should work great.
Nasogastric (NG) or Orogastric (OG) Tubes

2x the ETT size is the gastric tube size, whether placed through the nose or through the mouth. An NG tube goes down the nose to the stomach while an OG tube goes down the mouth to the stomach. They both have the same ending destination, just a different starting point. With that, more and more places are placing OG tubes in intubated patients, especially in the
context of trauma. There’s already one tube (ETT) sticking out the mouth, so most times, it’s easy to put another one there. The mouth hole is bigger than the nose hole and as such, it tends to be easier to place a gastric tube. And OG tubes help avoid issues such as sinusitis and nasal bleeding. Same size tubes, just with a different route.3,5
Above is what some of us were taught and have taught for years, but in a recent course, a very experienced medic shared a few things to remember:
- There are two holes in the nose (nostrils), therefore 2x the size of the oral ETT is the suggested NG size (again, it’s the same size if going down the mouth with an OG tube).
- Except in the tiniest of sizes, such as 5 Fr, NG/OG tube sizes are only available in even number sizes—6 Fr, 10 Fr, etc. If the 2x rule calls for an “odd size NG/OG tube,” like a 9 Fr, picking the next smaller/available size, in this case an 8 Fr, should work great.
- Astute readers will notice that there are two nostrils, however, only one mouth. So, yes, the same size tube can be placed down the mouth as down the nose. However, this is an example of where the 2x rule requires a bit of thought.
Foley Urinary Catheter
2x the oral ETT size is the Foley urinary catheter size. Urethral catheterization, aka “cathing,” a little guy is easy, there’s usually only one orifice, the urethra, up front to shoot for, but there are hopefully two testicles. So, 2x the size of the oral ETT is the Foley urinary catheter size. But “cathing” little girls is not easy by any means. There are usually two ovaries and there should be two orifices, the urethra and vagina. It takes at least two people to “cath” most little kids, so, 2x the size of the oral ETT is the Foley urinary catheter size.3
Just like with suction catheters and OG/NG tubes, Foley urinary catheter tube sizes are only available in even sizes, so if the 2x rule calls for an odd size Foley urinary catheter next smaller/available size should work great
Where to Secure the Oral ETT: The 3x Rule
3x the size of the oral ETT in centimeters is where the tube should be secured. Note this important word change—not taped but secured. Though “tube taping” is still commonly performed, more and more providers are using “tube holders” to secure the ETT. Secured works well as the goal is to secure the tube. Again, this is not a trick.3
Take that one step further with two insights about “the secured at” statement from a senior burn ICU nurse. 1) “Secured at the lips.” This is very commonly documented, but with trauma and/or burns, the lips can be very swollen. This can lead to an ETT being initially secured at “x” cm but when the swelling goes down, the tube still secured at “x” cm can be in a very different place. 2) “Secured at the teeth.” This is also very commonly documented, but most babies and small infants don’t have visible teeth. Patients with extensive facial trauma may not have a lot of teeth. “Secured at the gumline” more accurately describes this placement, as it follows the 3x rule.
Picking the Correct Size Chest Tube: The 4x Rule

4x the size of the oral ETT is the maximum chest tube size that should be placed for a pneumothorax (air) or hemothorax (blood). This rule has changed over the years. Whereas it used to be taught that 4x the oral ETT size was for evacuation of trapped air, 5x the oral ETT size was for evacuation of blood or other fluids. Now recent reference materials reflects a maximum of 4x the oral ETT size for drainage of either air or blood. Especially in the critical care transport, emergency, and critical care environments, smaller, more flexible, and far less painful pigtail chest catheters are increasingly being used across the lifespan.

“Four” your patient to be able to breathe with a collapsed lung, four times the oral ETT size is the maximum chest tube size or use an even smaller pigtail catheter.3,6
So, when it comes to caring for sick kids, the sicker the kid, the higher the stress. The higher the stress, the less your brain works. You are not in high school algebra anymore. Go back to kindergarten and count one to four. Or even easier: Why do math if you don’t need to? Peds cheat sheets are your best friends!
References
1. Ezri, T., et al, (2005). Tracheostomy and endotracheal intubation: A short history. Harefuah. 144(12). 891-893.
2. American Lung Association. (2025). Lung.org. Available: On-line: Accessed January 16, 2025.
3. Moses, S. (2025). Endotracheal tube. Family Practice Notebook. https://fpnotebook.com/Lung/Procedure/EndtrchlTb.htm. Available: On-line. Accessed January 16, 2025.
4. NeoResus.org.au. (2019). Clinical Practice Guidelines for Intubation. https://www.neoresus.org.au/learning-resources/key-concepts/advanced-interventions/endotracheal-intubation. Available: On-line. Accessed January 16, 2025.
5. Nickson, C. (2024). Nasogastric and orogastric tubes. Life in the Fast Lane. https://litfl.com/nasogastric-and-orogastric-tubes. Available: On-line. Accessed January 16, 2025.
6. Lyons NB, Abdelhamid MO, Collie BL, et al. Small versus large bore thoracostomy for traumatic hemothorax: A systematic review and meta-analysis. Journal of Trauma and Acute Care Surgery. 2024;97(4):631-638.
About the Authors
Scott DeBoer is an international pediatric emergency/transport nurse educator, paramedic at Universal Studios Orlando, and the CXO of Pedi-Ed-Trics Emergency Medical Solutions.
Lisa DeBoer is an international healthcare entrepreneurial educator, paramedic at Universal Studios Orlando, and the CEO of Pedi-Ed-Trics Emergency Medical Solutions.
Michael Seaver is an international healthcare informatics expert, author, and educator.
Scott DeBoer is a consultant for Air Life.





