


Use of Micropuncture Needle in the Treatment of Pericardial Effusion by Pericardiocentesis
Introduction
 Patients with pericardial effusions present to all medical specialties, although their care is often supervised by cardiologists. Percutaneous needle pericardiocentesis remains the most common therapeutic procedure for the management of symptomatic effusions and is also utilized as a diagnostic procedure in some patients with asymptomatic pericardial effusions.
Patients with pericardial effusions present to all medical specialties, although their care is often supervised by cardiologists. Percutaneous needle pericardiocentesis remains the most common therapeutic procedure for the management of symptomatic effusions and is also utilized as a diagnostic procedure in some patients with asymptomatic pericardial effusions.
The micropuncture 21-gauge needle has increasingly become the mainstay of vascular access in various cardiac procedures. Recent data for femoral arterial access has shown a significant reduction in bleeding complications with the use of a micropuncture 21-gauge needle as compared to the standard 18-gauge needle.1 Increasingly, the micropuncture needle for pericardiocentesis has been been used for access of the pericardium in patients with compromising pericardial effusion.2 The use of this technique, however, is sparsely described in the literature. We present a case series of the use of the 21-gauge micropuncture needle in successful pericardiocentesis.
Methods
Data Collection
 Our study was approved by the institutional review board at our institution. We conducted a retrospective chart review on 14 patients from 2012-2016 who underwent pericardiocentesis with the use of a micropuncture 21-gauge needle kit. The indications for pericardiocentesis were clinical cardiac tamponade, echocardiography signs suggestive of cardiac tamponade, and symptomatic pericardial effusion.
Our study was approved by the institutional review board at our institution. We conducted a retrospective chart review on 14 patients from 2012-2016 who underwent pericardiocentesis with the use of a micropuncture 21-gauge needle kit. The indications for pericardiocentesis were clinical cardiac tamponade, echocardiography signs suggestive of cardiac tamponade, and symptomatic pericardial effusion.
Baseline data characteristics for each patient were reviewed in this retrospective analysis. The patient’s age, gender, body mass index, left ventricular function, blood pressure, heart rate, effusion output, and effusion description were listed. Additionally, the presence of echocardiographic evidence of tamponade, complications, and the need for needle upgrade were also reported.
Procedure/Pericardiocentesis
 The patient was prepped and draped in sterile fashion. The patient was positioned in an upright 45-degree angle. Fluoroscopy was positioned in the anterior-posterior (AP) caudal view. Local lidocaine was administered at the entry site of the xiphoid process. The 21-gauge micropuncture needle was attached to a three-way stopcock. The perpendicular port was attached to a pressure line that was connected to a standard manifold. The coaxial port was attached to a standard 10 cc syringe filled with 2% lidocaine and saline.
The patient was prepped and draped in sterile fashion. The patient was positioned in an upright 45-degree angle. Fluoroscopy was positioned in the anterior-posterior (AP) caudal view. Local lidocaine was administered at the entry site of the xiphoid process. The 21-gauge micropuncture needle was attached to a three-way stopcock. The perpendicular port was attached to a pressure line that was connected to a standard manifold. The coaxial port was attached to a standard 10 cc syringe filled with 2% lidocaine and saline.
 The micropuncture needle was inserted into the left xiphocostal angle perpendicular to the skin approximately 3 mm below the left costal margin. The needle was then lowered parallel to the chest wall and directed towards the cardiac apex. Under fluoroscopic guidance, the needle was advanced in 5 to 10 mm until it reached the pericardial fluid. A “giving” sensation suggested penetration of the parietal pericardium; the “ticking” sensation suggested contact with the right ventricle as described by Spodick.3 Pericardial pressure was obtained and a 3 cc contrast injection into the pericardial space was performed to confirm position. The .018-inch guidewire was placed through the needle under fluoroscopy. Using a modified Seldinger technique, the needle was removed and a 5 French (Fr) sheath/introducer was introduced into the pericardial space. An .035-inch x 80 cm guidewire was placed into the pericardial and again, using the modified Seldinger technique, an 8.5 Fr, 40 cm high flow straight catheter was placed into the pericardial space. After removal of the effusion, the pericardial drain was left in place for observation of recurrence.
The micropuncture needle was inserted into the left xiphocostal angle perpendicular to the skin approximately 3 mm below the left costal margin. The needle was then lowered parallel to the chest wall and directed towards the cardiac apex. Under fluoroscopic guidance, the needle was advanced in 5 to 10 mm until it reached the pericardial fluid. A “giving” sensation suggested penetration of the parietal pericardium; the “ticking” sensation suggested contact with the right ventricle as described by Spodick.3 Pericardial pressure was obtained and a 3 cc contrast injection into the pericardial space was performed to confirm position. The .018-inch guidewire was placed through the needle under fluoroscopy. Using a modified Seldinger technique, the needle was removed and a 5 French (Fr) sheath/introducer was introduced into the pericardial space. An .035-inch x 80 cm guidewire was placed into the pericardial and again, using the modified Seldinger technique, an 8.5 Fr, 40 cm high flow straight catheter was placed into the pericardial space. After removal of the effusion, the pericardial drain was left in place for observation of recurrence.
Results
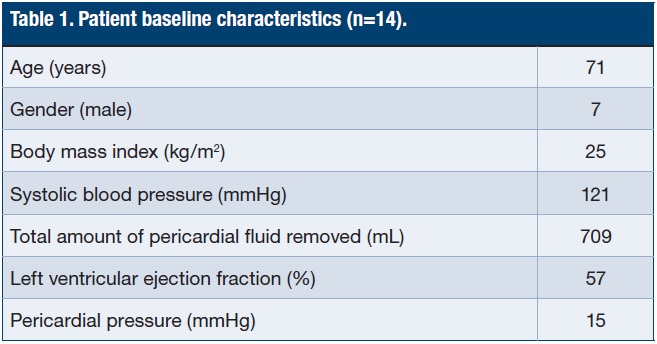 Baseline characteristics for the patients in our study can be seen in Table 1.
Baseline characteristics for the patients in our study can be seen in Table 1.
Age, gender, body mass index, systolic blood pressure, heart rate at time of procedure, amount of fluid drained, fluid analysis, echocardiographic evidence of tamponade, presence of complication, and need for upsize of the needle were all reviewed.
The mean patient age in our study was 71 years. Fifty percent of our patients were female. The mean body mass index was 25. The mean systolic blood pressure was 121 mmHg. Presence of pulsus paradoxus was not reported. The mean heart rate was 83 beats per minute.
On transthoracic echocardiogram, the mean left ventricular ejection fraction of patients in our study was 57. The echocardiographic signs of cardiac tamponade were present in 79% of our patients.
Right heart catheterization was performed in 11 of the 14 patients. The mean right atrial pressure prior to pericardial drain was 14 mmHg. Pericardial pressure prior to drainage was reported in all patients. The mean pericardial pressure prior to drainage was 15 mmHg.
The average amount of pericardial fluid drained in our study was 709 mL. The pericardial fluid was described as serosanguinous in 8 patients, serous in 2 patients and straw-colored fluid in 4 patients. Cytology was sent on all patients studied and none had evidence of malignancy in the pericardial fluid.
The need for upgrade to an 18-gauge long pericardiocentesis needle was observed in 3 of 14 cases. The mean body mass index in these 3 patients was 25. No procedural complications were noted in any patients.
Discussion
The literature reports a major complication rate of <2% using standard pericardiocentesis technique and equipment. The most serious and immediate mechanical complications of pericardiocentesis include myocardial puncture, vascular injury, pneumothorax, air embolism, and arrhythmia. Needle introduction may inadvertently traverse intra-abdominal organs if penetrating the peritoneal space. Vasovagal response to pericardial decompression occurs in up to 25% of patients and may be severe.4
We propose that the use of a smaller gauge and shorter length of the micropuncture needle may reduce the risk of peri-procedural complications. We also propose that the smaller caliber needle may offer an advantage in terms of patient comfort. Limitations of the micropuncture needle include large body habitus and excessive subcutaneous tissue. Both factors potentially limit the ability to penetrate the pericardium, although this was not observed in our patient cohort. To date, there are no randomized trials that address the use of the micropuncture needle in the drainage of pericardial fluid. Further investigation should be considered.
References
- Ambrose JA, Lardizabal J, Mouanoutoua M, Buhari CF, Berg R, Joshi B, et al. Femoral micropuncture or routine introducer study (FEMORIS). Cardiology. 2014; 129(1): 39-43.
- Kern M. Conversations in cardiology: should we use micropuncture technique for pericardiocentesis? Cath Lab Digest. 2015 Sept: 23(9). Available online at https://www.cathlabdigest.com/article/Conversations-Cardiology-Should-We-Use-Micropuncture-Technique-Pericardiocentesis. Accessed September 7, 2016.
- Spodick DH. Acute cardiac tamponade. N Engl J Med. 2003 Aug 14; 349(7): 684-690.
- Holt BD. Diagnosis and treatment of pericardial effusion. UpToDate, Inc., Wolters Kluwer. Available online at https://www.uptodate.com/contents/diagnosis-and-treatment-of-pericardial-effusion. Accessed September 7, 2016.
- Reddy PS, Curtiss EI, Uretsky BF. Spectrum of hemodynamic changes in cardiac tamponade. Am J Cardiol. 1990 Dec 15; 66(20): 1487-1491.
- Wong B, Murphy J, Chang CJ, Hassenein K, Dunn M. The risk of pericardiocentesis. Am J Cardiol. 1979 Nov; 44(6): 1110-1114.
- Spodick DH. Pathophysiology of cardiac tamponade. Chest. 1998 May; 113(5): 1372-1378.
Disclosure: The authors report no conflicts of interest regarding the content herein.
The authors can be contacted via Arvind Gireesh, MD, FACC, at agireesh@yahoo.com.
