


Use of Art Therapy in Geriatric Populations
In the United States, the population of older adults continues to grow as more baby boomers reach retirement age. Aging is associated with an increased number of cognitive and physical impairments, requiring various interventions. For decades, art has been used in long-term care facilities to provide residents with something constructive to do. Less commonly, it is used as a therapy to address older adults’ psychological needs. When art therapy is employed, various forms and mediums are used to foster the creative process as a vehicle for healing. Research indicates that art therapy can increase motivation, self-esteem, and self-confidence while facilitating communication and maintaining cognitive functioning in older adults. In this article, the authors review the effectiveness of using pottery, mandalas, therapeutic thematic arts programming, and home-based art therapy in elderly populations with various impairments. (Annals of Long-Term Care: Clinical Care and Aging. 2012;20[6]:28-32.)
_________________________________________________________________________________________________________________
In 2010, approximately 50 million Americans were 62 years of age or older according to the US Census Bureau.1 This represents a 21% increase since the 2000 Census in the number of Americans over the age of 62 years,1 henceforth referred to as older adults. It is logical to surmise that as the number of elderly Americans increases, the need for mental healthcare increases, because aging is associated with numerous physical and cognitive impairments. In particular, there has been a documented increase in the number of individuals with dementia. Alzheimer’s Disease International’s World Alzheimer Report 2009 stated that 36 million persons globally were living with Alzheimer’s disease and dementia in 2009, representing a 10% increase since 2005.2 In the United States alone, 5.4 million people are living with Alzheimer’s disease, the most common form of dementia.2 Art therapy has been found to enhance mood; increase motivation, self-esteem, and self-confidence; and reduce anxiety in older adults. This article reviews the literature on the therapeutic use of art with older adults and explores the current use of art therapy counseling for individuals with dementia or other impairments.
Art and Older Adults
Professional artists typically enjoy their most productive and lucrative period in young to middle adulthood.3 Less commonly, artists continue or begin their work in old age. Michelangelo, who lived to the age of 88, worked throughout his life.4 Willem de Kooning also continued creating, even during the onset and progression of his Alzheimer’s disease.5 Examples of individuals who turned to art in their late adulthood include Grandma Moses and Grandma Layton. Grandma Moses began her career as a folk artist and painter in her 70s and continued for much of the remaining 30 years of her life.6 Grandma Layton took a contour drawing class at the age of 68 and continued to create for the rest of her life, crediting drawing with curing a 35-year depression.7
Activity directors and occupational therapists have used art for decades in senior centers and other long-term care facilities. These art activities are often used to provide residents with something constructive to do or to address physical and motor issues. Less commonly, creative arts therapists use art in these settings to assist patients with psychological coping and other needs. These professionals may experience resistance to this form of mental health therapy, as many people view art as something for children or worry about their creative capabilities on the basis of previous criticisms of their artistic attempts.8 With time and patience, however, art can provide great opportunities for older adults. Some researchers and therapists state that dementia can unlock creativity and enhance communication.6,9,10 Changes in artistic production and style are evident in the work of professional artists with dementia diagnoses, such as de Kooning.6
Therapeutic Art
Art therapy, sometimes referred to as art therapy counseling, is a form of therapy that uses the creative process as an instrument for healing. According to the American Art Therapy Association, art therapy is defined as “a mental health profession that uses the creative process of art making to improve and enhance the physical, mental, and emotional well-being of individuals of all ages.”11 It is based on the belief “that the creative process involved in artistic self-expression helps people to . . . resolve conflicts and problems, develop interpersonal skills, manage behavior, reduce stress, handle life adjustments, and achieve insight.”11
Art therapy occurs in conjunction with traditional talk therapy or as standalone primary therapy. Some mental health counselors also make use of art within their therapy sessions. Often referred to as creativity counseling, this use overlaps with art therapy in technique, but differs in the educational background of its practitioners. Art therapy requires the study of art and psychotherapy, typically mental health counseling or clinical psychology.12 Creativity counseling requires the study of mental health counseling, but no specific training in art or art therapy.13
Art Therapy In Elders
In art therapy, the medium and methods used can take numerous forms. A comprehensive discussion of each of these is well beyond the scope of this article. We provide an overview of pottery, mandalas, therapeutic thematic arts programming (TTAP), and home-based art therapy, all of which have been assessed in various populations of older adults.
Pottery
Researchers have found some success with pottery as a therapeutic modality for older adults. Doric-Henry14,15 performed a study on the use of the Eastern Method of throwing pottery with 20 residents of a nursing home who had varying degrees of physical and cognitive impairments. The Eastern Method of throwing pottery begins with several pounds of clay that is precentered on a pottery wheel. This allows several pots to be completed using the same clay, eliminating the necessity of throwing and centering new clay for each project. The researcher precentered the clay to enable participants with multiple ability levels to participate and to make the use of the pottery wheel less intimidating.14,15
The researcher used a convenience sample because “the physical nature of the intervention made random sampling impractical as many residents were incapable of participating.”14 Doric-Henry explored levels of depression, anxiety, and self-esteem with the 20 participants and with 20 control group members. Measurements included the Beck Depression Inventory,16 the State-Trait Anxiety Inventory,17 and the Coopersmith Self-Esteem Inventory.18 In addition to administering these assessments before and after the pottery intervention, the researcher made qualitative observations and administered a subjective questionnaire at the end of the study.
Doric-Henry used two-sample t tests to assess group equivalency and matched sample t tests to analyze results.14 The two-sample t tests revealed no difference in the two groups in pretest depression and self-esteem scores; however, the pretest anxiety scores were significantly lower in the experimental group than in the control group.
Participants in the pottery intervention showed significant reduction in anxiety and depression, as well as significant increases in self-esteem compared with the control group, as shown by the matched sample t tests.14,15 Doric-Henry also compared subgroups with matched sample t tests and found that those who already had higher self-esteem, lower depression, and lower trait and state anxiety experienced no significant changes in these areas, whereas those with higher depression and trait and state anxiety scores and lower self-esteem experienced a significant improvement in these areas.14 Doric-Henry completed several case studies that support these results.14,15
This study indicates that pottery as therapy is particularly beneficial for older adults with high depression, high anxiety, and low self-esteem.14 The small sample size must be noted here. A similar study with a larger sample would provide stronger evidence for the efficacy of pottery as therapy with this population. Also problematic is the use of convenience sampling. Doric-Henry reported that participants volunteered for this study; therefore, a preexisting difference may be present between those who volunteered and those who did not.14
Mandalas
Mandala is a Sanskrit word that means “circle,” a geometric shape amply found in nature and throughout the universe, imbuing it with deeper meaning and cosmic significance among many cultures. As an art form, mandalas are circular art pieces that are often symmetrical. Production of a mandala is thought to help shed light on the inner being, especially as it relates to the world at large, and mandalas are used to promote meditative states and psychological centering (focusing attention on a particular stimulus or the current environment). Couch19 completed a study of mandala creation by older adults with dementia, guided by the MARI (Mandala Assessment Research Instrument) card test developed by art therapist Joan Kellogg. The MARI card test is a holistic, nonverbal evaluation tool that requires the participant to color a mandala and to intuitively select from a set of mandala design cards a series of mandala images and then an associated color for each design from a set of colored cards.20 This test is based on Kellogg’s observation of hundreds of mandala drawings completed by multiple client populations and on Jung’s archetypal theory, which postulates that people share a collective unconscious, including shared concepts and imagery (sort of a genetic memory).21 Using her observations and Jung’s theory, Kellogg identified 13 life stages in mandalas that help to describe clients’ emotional states, including conscious and unconscious feelings present during mandala creation (Table).19
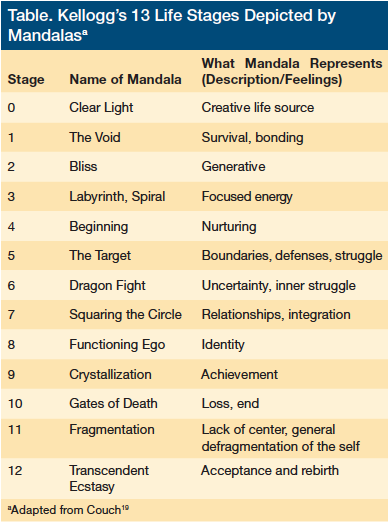
Couch selected the MARI card test because individuals with dementia respond well to drawing stimuli.19 She examined nearly 500 mandalas completed by more than 70 older adults. The three most commonly seen life stages in Couch’s study are the 5th stage (n=138), which represents defense, struggle, and setting of boundaries; the 11th stage (n=86), which represents a lack of center and a general defragmentation of the self; and the 6th stage (n=72), which represents uncertainty and an internal struggle. Using Kellogg’s theory, Couch speculates that the struggle with boundary setting represented by the 5th stage relates primarily to the struggle in early dementia of older adults with their caregivers, when they attempt to preserve some control over their lives, whereas the defragmentation of the self in the 11th stage indicates the disintegration that occurs as cognitive decline takes hold in dementia.19 She hypothesizes that the imagery in the 6th stage reflects “a patient’s struggle with tolerating ambivalent feelings toward significant others.”19
Couch observed that the mandalas provided a sufficient stimulus for art making despite the patients’ level of cognitive impairments. She also found that overall feelings of powerlessness were pervasive, as reflected in the MARI card test categories in which the produced mandalas fit.19 This study provides some insight into how art can help clients who are quickly losing the cognitive ability to communicate their internal states. This study did, however, use a projective assessment, which is notoriously inconsistent in research; thus, a replication study should be conducted to compare results.
Therapeutic Thematic Arts Programming
Developed by therapist and researcher Linda Levine-Madori, PhD, TTAP provides a structured arts program for adults. The TTAP method is based on Levine-Madori’s 25 years of research in gerontology and combines aspects of therapeutic recreation and the creative arts.The five main objectives of the TTAP method are to enrich older adults’ lives by the following means22:
1. To embrace the concept of “use it or lose it” by stimulating all areas of brain functioning to enhance cognitive, emotional, physical, and social capacity.
2. To provide opportunities for the individual to integrate life experiences into group experiences through object relations in the creative arts process.
3. To provide a system in which the individual can reintegrate into a supportive social group to foster feelings of safety and support and thereby increase social participation.
4. To engage the participant in a multitude of creative arts experiences: music, drawing, sculpture, movement, poetry, and special theme events.
5. To provide programming that enables the flow of activities and life to flourish.
The method aims to enhance self-esteem, self-worth, and motivation with older adult groups. It also encourages expression of older adults’ past, present, and future life experiences, and it shows their interests across their lifespan through creative activities. In addition, the TTAP method incorporates an individual’s unique skills, multiple intelligences, and capabilities for self-expression.22
Alders and Levine-Madori23 used the TTAP method with 24 older Hispanic and Latino adults, most of whom were Puerto Rican, at a community center. In this pilot study, the efficacy of the TTAP method in improving cognitive functioning was measured using the clock drawing test (CDT),24 an exercise that requires participants to draw a clock, and the Cognitive Failures Questionnaire (CFQ),25 a self-report measure. Both have been normed and validated. The study did not use a random sample or random assignment; rather, researchers used a sign-up sheet that advertised “relaxing art therapy sessions” to recruit participants. Community members who did not want to participate in the art therapy served as the control group. Researchers administered the CDT and CFQ as both pretests and post-tests to assess the efficacy of the TTAP intervention in improving or maintaining cognitive functioning. Results of both tests indicated that participation in art therapy was positively correlated with an improvement in cognitive functioning, although researchers discarded data from two outliers in the CFQ data to achieve this result. Alders and Levine-Madori point out that “the CFQ scores serve as a reflection of change in self-perception and self-confidence, whereas the CDT scores (as intrinsic to the nature of the test) demonstrate changes in auditory comprehension, visual-spatial ability, and constructional praxis/visual motor skills.”23 This study provides promising results for the use of arts-based treatment to improve or maintain cognitive functioning. However, because of the small sample size, lack of randomization, and specific population, the results cannot be generalized. Future research must explore the use of the TTAP method with more diverse populations.
Home-based Art Therapy
Sezaki26 and McElroy and colleagues27 qualitatively assessed the success of in-home art therapy for older adults with varying needs. Sezaki reported on two case studies: one with a 73-year-old woman with multiple physical problems, including osteoporosis and osteoarthritis, Mrs. J; and another with a 69-year-old man with Alzheimer’s disease and his wife (caretaker), Mr. and Mrs. M.26 The therapist focused on Mrs. J’s strengths and encouraged her to set her own therapeutic goals. Mrs. J was once an artist, and the therapist observed that she appeared to gain self-confidence and pleasure in regaining her art by using multiple media and that she appeared to enjoy teaching art techniques to the therapist.
The therapist worked with Mr. and Mrs. M regarding Mr. M’s Alzheimer’s disease to assess and improve Mr. M’s communication with others, including his wife and son; to assess Mr. M’s cognitive loss; and to assist Mrs. M in dealing with her husband’s cognitive decline.26 The therapist used multiple art directives and media with the couple. Mrs. M initially self-reported feeling depressed as a result of the art therapy, stating that she could see more clearly just how much her husband had declined through this process. However, both Mrs. M and the couple’s son later reported that the art therapy improved Mr. M’s ability to communicate and their ability to understand him.26
McElroy and colleagues27 based their UK study of home-based art therapy services on the work of Sezaki.26 However, their methods of collecting and assessing the results of art therapy use for older adults with depression expanded beyond therapist observations.27 They used a semistructured interview developed by Robson28 and applied interpretive phenomenological analysis, as outlined by Smith and colleagues,29 to the results. The researcher and assistant coded the interview results and triangulated this information with researcher notes and session transcripts. The project also included a focus group of older adults with mental health needs who were participating in a day program and had previously received art therapy. This focus group assisted in developing questions, reviewing interview scripts, and providing responses to the research results.27 This study included five older adults with depression; the sample was a convenience sample referred to the researchers from a community mental health team. The authors reported that they initially sought eight participants, but because of inappropriate referrals, obtained only five. The average age of these five participants was 77 years. As a result of illness among the participants and the pregnancy of the lead researcher, only one of the five completed all eight sessions offered.27
McElroy and colleagues27 reported some challenges posed in the study that would need to be addressed in future home-based art therapy assessments. Participants identified the art therapist’s friendly disposition as a strength; however, more authority might be necessary on the art therapist’s part to maintain appropriate boundaries related to the home-based environment. In addition, distracters such as pets are common in home settings; in the future, therapists, clients, and caregivers should attempt to minimize distracters.27
Despite the challenges, McElroy and colleagues27 reported that family members, other caregivers, and participants valued the opportunity to participate in art therapy and particularly appreciated the home-based sessions. Benefits reported by some clients included increased confidence and motivation, as well as an outlet for emotions, which facilitated communication. These reports echoed the observations in the art therapist’s notes and the results of the interpretive phenomenological analysis. Many participants met goals that they had set at the outset of the art therapy and invited continued art therapy sessions beyond the initial 8-week study.27
Conclusion
The research studies described in this article indicate that art therapy can increase motivation, self-esteem, and self-confidence among older adults by facilitating communication and improving or maintaining cognitive functioning in this population. The research also implicates art therapy as a mood enhancer and anxiety reducer in older adults.
It is clear that art therapy is a useful tool for those who work with older adults. However, all of the studies had small sample sizes. In addition, there has been a paucity of quantitative/true experimental research regarding the use of art therapy in older adults. Of the studies we highlighted in this article, only two used an experimental design and those two studies had small convenience samples. Art therapy appears to be a promising method for use with older adults; however, more evidence-based research is needed.
The authors report no relevant financial relationships.
References
1. Howden LM, Meyer JA; US Census Bureau. Age and sex composition: 2010. 2010 Census Briefs. May 2011. www.census.gov/prod/cen2010/briefs/c2010br-03.pdf. Accessed April 5, 2012.
2. Alzheimer’s Disease International. World Alzheimer Report 2009. www.alz.co.uk/research/files/WorldAlzheimerReport.pdf. Accessed April 5, 2012.
3. Lanyon G, Smith L. A portrait of the artist as a young, middle-aged and elderly man. https://lonessmith.comhttps://s3.amazonaws.com/HMP/hmp_ln/imported/portrait_0.pdf. Accessed April 5, 2012.
4. Hibbard H, Hibbard S. Michelangelo. 2nd ed. Boulder, CO: Westview Press; 1985.
5. University of Alabama Birmingham Magazine. Painting in Twilight: An Artist’s Escape From Alzheimer’s [video]. May 2009. bit.ly/Mpxscq. Accessed April 5, 2012.
6. Stein J. The white-haired girl: a feminist reading. In: Grandma Moses in the Twenty First Century. New Haven, CT: Yale University Press; 2001.
7. Elizabeth Layton. www.elizabethlayton.com. Accessed April 5, 2012.
8. Edwards B. Drawing on the Right Side of the Brain. London, UK: Harper Collins; 1993.
9. Killick J, Craig C. Creativity and Communication in Persons With Dementia:
A Practical Guide. London, UK: Jessica Kingsley Publishers; 2011.
10.Woolhiser Stallings J. Collage as a therapeutic modality for reminiscence in patients with dementia. Art Ther J Am Art Ther Assoc. 2010;27(3):136-140.
11. American Art Therapy Association. Art therapy. www.americanarttherapyassocia
tion.org/aata-aboutus.html. 2012. Accessed April 5, 2012.
12. American Art Therapy Association. Masters education standards. www.americanartther
apyassociation.org/upload/masterseducationstandards.pdf. Published June 30, 2007. Accessed April 5, 2012.
13. Shallcross L. Working outside the box. Counseling Today. February 2011. https://ct.counseling.org/2011/02/working-outside-the-box. Accessed April 5, 2012.
14. Doric-Henry L. Pottery as art therapy with elderly nursing home residents. Art Ther J Am Art Ther Assoc. 1997;14(3):163-171.
15. Doric-Henry L. Pottery making on a wheel with older adult nursing home residents. In Perry Magniant RC. Art Therapy With Older Adults: A Sourcebook. Springfield, IL: Charles C. Thomas Pub Ltd; 2004.
16. Beck A, Ward C, Mendelson M, Mock J, Erbaugh J. An inventory for measuring depression. Arch Gen Psychiatry. 1961;4:561-571.
17. Speilberger C, Gorsch R, Lushene R, et al. State-Trait Anxiety Inventory (form Y): Self-Evaluation Questionnaire. Palo Alto, CA: Consulting Psychologists Press; 1983.
18. Coopersmith S. Self-Esteem Inventories. Palo Alto, CA: Consulting Psychologists Press; 1981.
19. Couch J. Behind the veil: mandala drawings by dementia patients. Art Ther J Am Art Ther Assoc. 1997;14(3):187-193.
20. Malchiodi C. The Art Therapy Sourcebook. 2nd ed. New York, NY: McGraw-Hill; 2007.
21. Storr A, ed. The Essential Jung. Princeton, NJ: Princeton University Press; 1983.
22. Levine-Madori L. Therapeutic Thematic Arts Programming for Older Adults. Baltimore, MD: Health Professions Press; 2007.
23. Alders A, Levine-Madori L. The effect of art therapy on cognitive performance of Hispanic/Latino older adults. Art Ther J Am Art Ther Assoc. 2010;27(3):127-135.
24. Sunderland T, Hill JL, Mellow AM, et al. Clock drawing in Alzheimer’s disease: a novel measure of dementia severity. J Am Geriatr Soc. 1989;37(8):725-729.
25. Larson G, Alderton D, Neideffer M, Underhill E. Further evidence on dimensionality and correlates of the Cognitive Failures Questionnaire. Br J Psychol. 1997;88(1):29-38.
26. Sezaki S. Home-based art therapy for older adults. Art Ther J Am Art Ther Assoc. 2000;17(4):283-290.
27. McElroy S, Warren A, Jones F. Home-based art therapy for older adults with mental health needs: views of clients and caregivers. Art Ther J Am Art Ther Assoc. 2006;23(2):52-58.
28. Robson C. Real World Research. 2nd ed. Oxford, UK: Wiley-Blackwell; 2002.
29. Smith J, Osbourne M, Jarman M. Doing interpretive phenomenological analysis. In: Murray M, Chamberlain K. Qualitative Health Psychology: Theories and Methods. 2nd ed. London, UK: Sage; 1999.
