


Improving Care Delivery Using Health Information Technology in the Home Care Setting: Development of the Home Continuation Care Dashboard
Lack of communication between physicians and case managers has been shown to result in adverse medical events and to increase healthcare costs for elderly individuals receiving home- and community-based long-term care (LTC) services. To remedy this problem, a multidisciplinary team from Florida International University formed a partnership with a local home care agency to develop the Home Continuation Care Dashboard, an Internet-based portal designed to facilitate communication between case managers, physicians, patients, and their caregivers. In this article, the authors explain the need for improved communication strategies and describe the team’s ongoing efforts to develop, refine, and implement their prototype Web-portal in homes with older persons receiving home- and community-based LTC services.
___________________________________________________________________________________________
According to the Centers for Disease Control and Prevention, the number of older adults in the United States who will require long-term care (LTC) services is projected to reach 27 million by the year 2050.1 Most of these individuals will receive healthcare services within the home and in community-based settings, and many will be eligible for Medicaid assistance to pay for this care.1 Improving the efficiency of care delivery for a growing, culturally diverse Medicaid-eligible population is vital for state Medicaid programs, as these programs are facing an increased demand for home- and community-based services (HCBS) and an impeding budget shortfall due to states implementing a range of Medicaid cost-cutting measures.2 Older adults who are dually eligible for Medicare and Medicaid incur healthcare costs four to six times greater than those enrolled only in Medicare.3
Previous research has demonstrated that the lack of communication among patients and caregivers, case managers, and physicians can result in adverse events, medication errors, and re-hospitalizations that result in poor patient outcomes and add to the increasing demands on state and federal Medicaid budgets.4-9 In a 2007 report, the US Department of Health and Human Services identified the need for the development of health information technology (HIT) in the home care setting to improve the exchange of patient information.7 Individual states have identified the need for improved health information exchange with regard to older adults as a means to support improved care coordination and access to services.10 The problem is that there is no established method for the case manager to provide patient information to the physician, and there is no established method for the physician to update the case manager. Physicians often complain that they cannot find a case manager when needed,11 and case managers often complain that physicians are not interested in their patient reports.12,13 As a result, the communication between home care case managers and physicians is limited and inefficient,14-16 raising concerns about the quality of home care service delivery and patient care.17
The current healthcare system does not emphasize prevention, chronic care, or care coordination,18 contributing to increasing healthcare costs. For example, in 2001, readmissions for congestive heart failure were estimated to cost $44,479 per patient annually.19 As the elderly population continues to grow, these types of preventable healthcare costs will be a greater burden on state Medicaid programs responsible for providing LTC services. Medicaid is currently the largest item in state budgets, and states are reducing provider payments and increasing patient copayments to provide care to the growing Medicaid population.20 Innovative approaches to reducing the Medicaid cost burden are needed.
Scope of the Health Information Technology Problem
Innovative strategies are needed to improve communication and coordination of care for seniors receiving HCBS. To the best of our knowledge, there are no existing HIT applications with the needed functions to address medically complex older adults receiving HCBS, a population that is often hospitalized. Existing HITs also do not address monitoring of patients, coordination of HCBS services, or transition between hospital and home care. Current HIT platforms focus mostly on traditional electronic health records (EHRs) that are managed in hospital or physician offices.7 These HIT platforms do not handle the setting of at-home care, and, specifically, the migration of client data from home care to primary care. Federal policies, including the Affordable Care Act of 2010, have attempted to accelerate the integration of HIT into healthcare by instituting financial incentives for healthcare providers who implement HIT, such as subsidies for technology implementation and reimbursement models that encourage the use of HIT.21,22 These incentives emphasize the use of EHRs by hospitals and physicians and have excluded participation by home healthcare agencies.23 We postulate that including home health agencies in federal policy initiatives may increase the adoption of HIT within primary care settings for comprehensive, clinical purposes, and expanding the use of HIT in healthcare is a primary goal of HIT policy.24 Evaluating the extent to which HITs can improve patient outcomes and reduce healthcare costs through the prevention of unnecessary health services will become increasingly important as a growing number of older Americans rely on LTC services delivered in home or community settings, rather than in permanent institutional settings. The US Department of Health and Human Services and other organizations have indicated that HIT programs for the home care setting could improve the exchange of patient information.7 In addition, patients and caregivers have expressed an interest in having online
access to health indicators and related information,25 a finding that our previous research confirmed.
When we spoke with the home care case managers at the local home care agency that we partnered with, they stated that they believed that use of a Web-based portal for communicating with their clients’ physicians would facilitate sharing patient information and coordinating care. Ideally, they wanted a way for case managers, physicians, and others involved with home care clients to relay patients’ physical and mental health changes in a more frequent, concise, and streamlined manner. It is clear that the current means of relaying patient information is severely lacking. The Institute of Medicine has described this dilemma, noting patient records to be “a collection of paper records, which often are poorly organized, illegible, and not easy to retrace, making it nearly impossible to manage various illnesses, especially chronic conditions, that require frequent monitoring and patient support.”26
The Home Continuation Care Dashboard
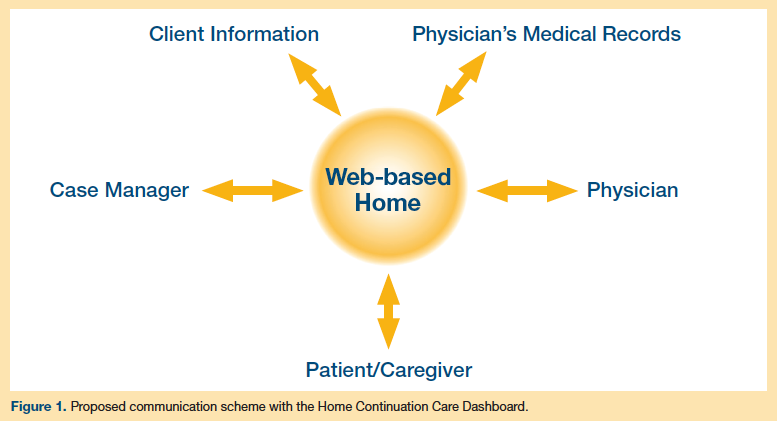
To improve care transitions and coordination, our team has developed the Home Continuation Care Dashboard (HCCD, “Home Care Dashboard”) through a partnership with a local in-home care service provider. The HCCD stores and displays patient data that are necessary to facilitate effective exchange of information concerning patients receiving HCBS, enabling patients, caregivers, case managers, and physicians to access and add information to the same records (Figure 1). The goal is to promote a safe, seamless transition between the hospital and home care setting.17 The HCCD, which is accessible online, is designed to improve the exchange of patient information and has the potential to reduce healthcare costs, improve care transitions across settings, increase patient safety, and promote improved health outcomes for nursing home–eligible older adults enrolled in HCBS programs.27
The HCCD has four objectives, which are as follows:
1. Increase and enhance how patients and their caregivers access information and communicate (ie, when they have questions, need to clarify conflicting information, want more information, need to modify or discuss the care plan, or report a change in patient status).
2. Increase and enhance how physicians monitor the status of their patients receiving HCBS and how they communicate and exchange patient information with case managers.
3. Improve the safety of care transitions from the home to the hospital and back to the home.
4. Provide caregivers and patients with links to educational materials and local service information, which are resources that have been historically underused.28
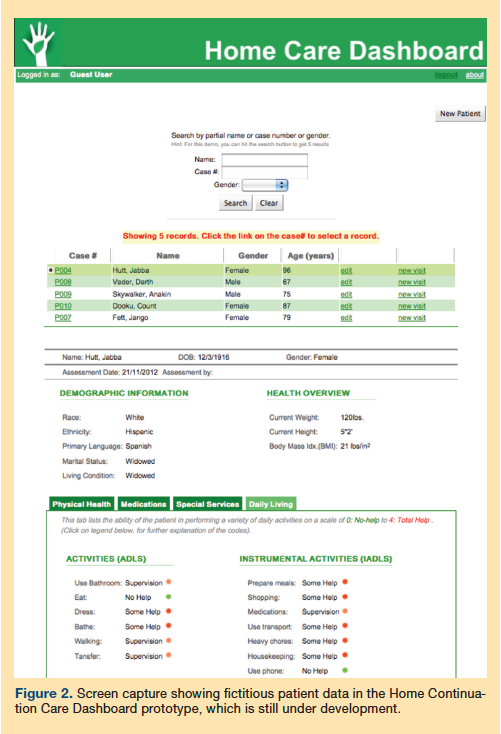
Currently, the HCCD is a working prototype, and future studies of feasibility and usability are planned. At present, the dashboard has not yet been fully developed. At a minimum, the dashboard will contain demographic and clinical information that states require home healthcare agencies to collect and record. These studies will be conducted with an interdisciplinary team of researchers from the fields of nursing, physical therapy, social work, public health, and HIT. Development and refinement of the HCCD will occur based on input from key stakeholders, such as physicians, case managers, patients, caregivers, and senior level management from the participating home health agency. This process will help us to identify additional functions that will be added to the dashboard. Our prototype is accessible at https://homecaredashboard.com. Figure 2 shows the HCCD interface.
Benefits and Barriers of Implementing the Home Care Dashboard
The role of HIT is to help the caregiver easily, accurately, and quickly capture in electronic format all information that is important for the well-being of the patient. Currently, case managers document most of this information with paperwork (eg, in Florida, an Elders Affairs Assessment Instrument form is completed). Family members do not generally have a way to record and access this information. We think that a case manager or caregiver should be able to use Internet-based technology to record such data. The interface for this software should be intuitive and require minimal training. A platform such as HCCD would enable multidirectional communication among case managers, physicians, and patients.17
In addition to the benefits for patients, technologies such as the HCCD would provide benefits to the healthcare system as a whole. Administrative efficiencies can be achieved through coordinated communication between physicians and home caregivers. In the absence of coordinated communication, phone calls or fax exchanges would need to occur between the physician’s office and the home care institution. HCCD has the potential to reduce these time-consuming and sometimes inefficient methods of communication.
While most physician practices and hospitals currently use some form of HIT, a major barrier to the widespread adoption of HIT in home healthcare is the issue of system interoperability. By integrating home healthcare agencies into the existing systems, in-home providers can provide physicians and hospitals with accurate biopsychosocial patient information, which is not typically collected through current HIT systems,29 such as medication adherence, environmental conditions, and depression symptoms. Such data could improve clinical decision-making without increasing the burden of data collection for hospitals and physicians.
(Continued on next page)
Cost Considerations. Future research will measure the costs of implementing HCCD. Implementation would involve the costs of providing the necessary hardware (ie, computers and Internet access) to those homes with homebound elders who do not already have it. Server space will be needed to host the HCCD platform, and technical support will be necessary to address bugs in the Website or answer questions from case managers, physicians, patients, and family caregivers
using HCCD. Training will be necessary to ensure that case managers, physicians, patients, and family caregivers know how to use HCCD to the fullest extent possible. The HCCD will also need to be monitored and periodically evaluated to identify needed updates and modifications based on feedback from its users.
These costs need to be compared with the potential cost savings resulting from improved care coordination and care transitions to determine whether these cost savings outweigh the costs of implementation. Such a situation would give insurers a financial incentive to sponsor the widespread implementation of HCCD. If the cost savings resulting from lower healthcare expenditures are not greater than the costs of implementation, analysis of improvements in clinical outcomes will be needed to determine whether such improvements provide significant justification for incurring the implementation costs of HCCD.
Determining the Optimal Approach for Implementation. In terms of large-scale implementation of a system such as HCCD, there are various options. First, states could create a central warehouse of home care data for all older home care patients. Further, states could create Website interfaces for case managers and physicians to read and input data. States could also provide standardized application interfaces to enable institutions to integrate home care data access into their own systems. This standardized model would ensure that data collected would be consistent across agencies within each state, but this approach might restrict agencies’ abilities to modify the platform for their individual needs, thereby limiting innovation.
Another alternative is to support home agencies to build their own HCCD platforms and provide a Web interface that enables physician access. The problem with this approach is that if a physician has patients from multiple home care agencies, he or she would have to use separate HCCD interfaces for each. Also, if a patient moves from one home care agency to another, his or her data would have to be transferred to the new agency’s system. Future research is needed to determine the optimal model for implementation and dissemination of home care HIT such as HCCD. An additional step for the adoption of HIT into home healthcare is to determine which data and information are of most value in improving communication and care coordination to promote better patient outcomes. Formative research is needed to determine which system features and clinical metrics facilitate improved patient care.
Benefits of Using Technology to Improve Healthcare Communication. The goal of case management teams is to collectively gather and process information about patient care.30 With technology that improves communication and coordination between the members of case management teams (eg, case managers, care recipient, family caregiver, physicians, and other clinicians), it is possible to improve clinical decision-making.31,32 The overall result may be improved outcomes for patients as well. In other healthcare settings, similar technology has demonstrated numerous benefits, including improved use of preventive health services, decreased use of emergency department and physician services,33 improved patient safety,34 improved clinical decision-making, and decreased patient mortality.35 Therefore, it may be possible that long-term implications of our proposed technology may include postponing institutionalization and prolonging life, improving preventive care, improving health outcomes, and promoting independent living for home care clients. Subsequently, these benefits may also lead to cost savings for hospitals, Medicare, Medicaid, and private LTC insurance companies.
Conclusion
Lack of communication between physicians, case managers, patients, and caregivers is a well-documented problem that can result in adverse medical events and increased healthcare costs for seniors receiving home-based healthcare services. HIT has been shown to be effective in improving communication between patients, caregivers, and healthcare providers in other healthcare settings, but is not used in the home care setting. To address this, we developed HCCD as a means of making HIT available in this setting. Improved communication and coordination of care has the potential to improve patient outcomes and also reduce unnecessary healthcare costs for seniors receiving home healthcare services. Although introducing HIT into home healthcare has several advantages, there are barriers to its widespread implementation in this setting. Two major barriers are a lack of government financial incentives for home healthcare agencies to invest in these technologies and the difficulties of developing a system that interfaces with existing physician and hospital HIT systems. Further research is needed to develop a functional HIT system for use in home healthcare and to evaluate its costs and benefits.
References
- Caffrey C, Sengupta M, Moss A, Harris-Krojetin L, Valverde R. Home health care and discharged hospice care patients: United States, 2000 and 2007. National Health Statistics Reports; number 38. Hyattsville, MD: National Center for Health Statistics, 2011. www.cdc.gov/nchs/data/nhsr/nhsr038.pdf.
- Kaiser Commission on Medicaid and the Uninsured. Medicaid’s continuing crunch in the recession: a mid-year update for state FY2010 and preview for FY 2011. www.kff.org/medicaid/upload/8049.pdf. Accessed July 18, 2011.
- Fortinsky RH, Fenster JR, Judge JO. Medicare and Medicaid home health and Medicaid waiver services for dually eligible older adults: risk factors for use and correlates of expenditures. Gerontologist. 2004;44(6):739-749.
- Forster AJ, Clark HD, Menard A, et al. Adverse events among medical patients after discharge from hospital [published correction appears in CMAJ. 2004;170(5):771]. CMAJ. 2004;170(3):345-349.
- Naylor MD, Brooten DA, Campbell RL, Maislin G, McCauley KM, Schwartz JS. Transitional care of older adults hospitalized with heart failure: a randomized, controlled trial [published correction appears in J Am Geriatr Soc. 2004;52(7):1228]. J Am Geriatr Soc. 2004;52(5):675-684.
- Brown EL, Raue P, Schulberg H, Bruce M. Clinical competencies—caring for late-life depression in home care patients. J Gerontol Nurs. 2006;32(9):10-14.
- Coleman EA, May K, Bennett RE, Dorr D, Harvell J. Report on Health Information Exchange in Post-Acute and Long-Term Care. Washington, DC: US Department of Health and Human Services, 2007. https://aspe.hhs.gov/daltcp/reports/2007/HIErpt.pdf. Accessed November 16, 2012.
- Drury LJ. Transition from hospital to home care: what gets lost between the discharge plan and the real world? J Contin Educ Nurs. 2008;39(5):198-199.
- Snow V, Beck D, Budnitz T, et al. Transitions of Care Consensus Policy Statement American College of Physicians, Society of General Internal Medicine, Society of Hospital Medicine, American Geriatrics Society, American College of Emergency Physicians, Society of Academic Emergency Medicine. J Gen Intern Med. 2009;24(8):971-976.
- Illinois Department of Aging. Older Adult Services Act: 2011 Report to the General Assembly. Springfield, IL: State of Illinois Department of Aging, 2011. www.state.il.us/aging/1news_pubs/publications/oasa_anreprt2011.pdf. Accessed November 16, 2012.
- Milette L, Hébert R, Veil A. Integrated service delivery networks for seniors: early perceptions of family physicians. Can Fam Physician. 2005;51:1104-1105.
- Feltes M, Wetle T, Clemens E, Crabtree B, Dubitzky D, Kerr M. Case managers and physicians: communication and perceived problems. J Am Geriatr Soc. 1994;42(1):5-10.
- Munson M, Proctor E, Morrow-Howell N, Fedoravicius N, Ware N. Case managers speak out: responding to depression in community long-term care. Psychiatr Serv. 2007;58(8):1124-1127.
- Brown EL, Raue PJ, Mlodzianowski AE, Meyers BS, Greenberg RL, Bruce ML. Transition to home care: quality of mental health, pharmacy, and medical history information. Int J Psychiatry Med. 2006;36(3):339-349.
- Eloranta S, Welch A, Arve S, Routasalo P. A collaborative approach to home care delivery for older clients: perspectives of home care providers. J Interprof Care. 2010;24(2);198-200.
- Fairchild DG, Hogan J, Smith R, Portnow M, Bates DW. Survey of primary care physicians and home care clinicians. J Gen Inter Med. 2002;17(4):253-261.
- Ruggiano N, Shtompel N, Hristidis V, Roberts L, Grochowski J, Brown EL. Need and potential use of information technology for case manager-physician communication in home care. Home Health Care Manage Pract. 2012;24(6):292-297.
- Davis K. Paying for care episodes and care coordination. N Engl J Med. 2007;356(11):1156-1168.
- Jerant AF, Azari R, Nesbitt TS. Reducing the cost of frequent hospital admissions for congestive heart failure: a randomized trial of a home telecare intervention. Med Care. 2001;39(11):1234-1245.
- Institute of Medicine. Crossing the quality chasm: a new health system for the 21st century. https://iom.edu/Reports/2001/Crossing-the-Quality-Chasm-A-New-Health-System-for-the-21st-Century.aspx. Accessed November 26, 2012.
- Smith VK, Rudowitz R, Snyder L; Kaiser Commission on Medicaid and the Uninsured. Moving Ahead Amid Fiscal Challenges: A Look at Medicaid Spending, Coverage and Policy Trends. Results From a 50-State Medicaid Budget Survey for State Fiscal Years 2011 and 2012. Washington, DC: The Henry J. Kaiser Family Foundation, 2011. www.kff.org/medicaid/8248.cfm. Accessed November 16, 2012.
- Blumenthal D. Launching HITECH. N Engl J Med. 2010;362(5):382-385.
- Kocher R, Emanuel EJ, DeParle NA. The Affordable Care Act and the future of clinical medicine: the opportunities and challenges. Ann Intern Med. 2010;153(8):536-539.
- Wolf L, Harvell J, Jha AK. Hospitals ineligible for federal meaningful-use incentives have dismally low rates of adoption of electronic health records. Health Aff (Millwood). 2012;31(3):505-513.
- Jha AK. Meaningful use of electronic health records: the road ahead. JAMA. 2010;304(15):1709-1710.
- Center for Technology and Aging. mHealth Technologies: Applications to Benefit Older Adults. www.techandaging.org/mHealth_Position_Paper_Discussion_Draft.pdf. Published March 2011. Accessed November 16, 2012.
- Hillstead R, Bigelow J, Bower A, et al. Can electronic medical record systems transform health care? Health Aff (Millwood). 2005;24(5):1103-1117.
- Brown EL, Friedemann ML, Mauro A. Use of adult day service centers in an ethnically diverse sample of seniors [published online ahead of print September 24, 2012]. J Applied Gerontol. doi:10.1177/0733464812460431.
- Glasgow RE, Kaplan RM, Ockene JK, Fisher EB, Emmons KM. Patient-reported measures of psychosocial issues and health behavior should be added to electronic health records. Health Aff (Millwood). 2012;31(3):497-504.
- Leavitt HJ. Some effects of certain communication patterns on group performance. J Abnorm Soc Psychol. 1951;46(1):38-50.
- Propp KM. Collective information processing in groups. In: Frey LR, Gouron DS, Poole MS, eds. The Handbook of Group Communication Theory and Research. Thousand Oaks, CA: Sage Publications:225-250.
- Taylor D, Faust WL. Twenty questions: efficiency in problem solving as a function of size of group. J Exp Psychol. 1952;44(5):360-368.
- Chaudhry B, Wang J, Wu S, et al. Systematic review: impact of health information technology on quality, efficiency, and costs of medical care. Ann Intern Med. 2006;144(10):742-752.
- Parente ST, McCullough JS. Health information technology and patient safety: evidence from panel data. Health Aff. 2009;28(2):357-360.
- Amarasingham R, Plantinga L, Diener-West M, Gaskin DJ, Powe NR. Clinical information technologies and inpatient outcomes: a multiple hospital study. Arch Intern Med. 2009;169(2):108-114.
Disclosures:
The authors report no relevant financial relationships.
Address correspondence to:
Timothy F. Page, PhD
Assistant Professor
Department of Health Policy and Management
Florida International University
11200 SW 8th Street
Miami, FL 33199
tpage@fiu.edu
