


How President Trump’s Remaining Days Will Affect LTC
If the first 100 days of the Trump Administration has your head spinning, imagine what the remaining days will bring. To date there are two pieces of legislation that paint the future for long-term care (LTC) as well as the Trump appointees’ priorities: the American Health Care Act (AHCA)1 and the Improving Access to Affordable Prescription Drugs Act.2
Increasingly our LTC environment is being impacted by federal and state legislators and regulators, especially given the seismic shift of control in Washington, DC. The repeal and replacement of the Affordable Care Act (ACA)3 via the AHCA is expected to increase the number of uninsured and underinsured, resulting in older adults entering Medicare sicker. As estimated by the Congressional Budget Office,4 some 51 million Americans may be uninsured by 2026 with the new law—14 million less under Medicaid and 3 million less under employers (Table 1).

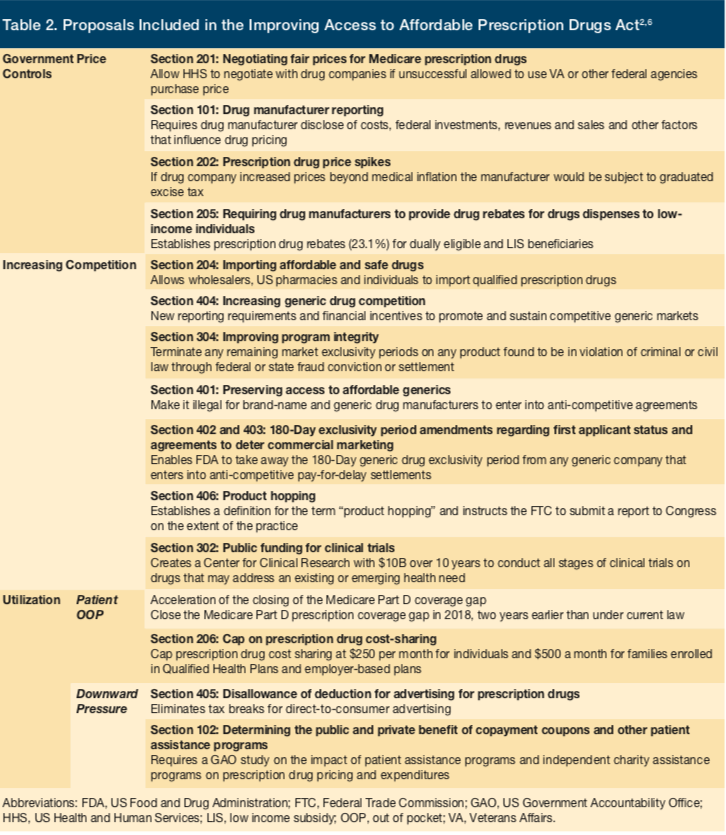
On the other side of this is legislation positioned to make pharmaceutical drugs more affordable. The Improving Access to Affordable Prescription Drugs Act aims to reduce prescription drug costs through reductions in both prices and utilization via government price controls, increasing competition and pressure on copayment coupons, and patient assistance programs. While the most significant measure would be the federal government negotiating prices for Medicare prescription drugs, there are other measures such as increasing competition through the allowance of drug importation and generic drug availability (Table 2). Although it is unlikely that all these provisions will be passed and implemented, the direction is clear—lower pharmaceutical costs.
The impact on Medicare/Medicaid beneficiaries will be most felt on older adults who can enter Medicare healthier as a result of improved access to medications, especially in treating chronic conditions such as diabetes, cardiovascular disease, and chronic obstructive pulmonary disease. This will be increasingly important when new potentially expensive treatments for early stage Alzheimers disease become available as these policies would increase access such that patients entering Medicare LTC could be delayed.
In addition to these two pieces of legislation, PresidentTrump’s recently released his $4.1 trillion budget for (FY) 2018,7 called “A New Foundation for American Greatness,” which outlines the administration’s federal funding requests and includes significant cuts to Medicare, Medicaid, and several health care institutions such as the Centers for Disease Control and Prevention (CDC), Food and Drug Administration (FDA), and Agency for Healthcare Research and Quality (AHRQ). Of course, this is only a proposal, as Congress must approve federal spending measures. Specifically, under this proposed budget, federal Medicaid spending would be reduced by $610 billion over 10 years on top of the $839 billion in Medicaid spending reductions called for under the House-approved AHCA. Further, the proposal calls for changing Medicaid into a block grant program or implementing per capita caps on federal Medicaid spending; it calls for moving all Medicaid beneficiaries to the new system—a shift from the AHCA’s approach, which would prevent states from moving older adults or individuals with disabilities into the new system. The budget proposal also calls for more than $72 billion in cuts to benefits for US residents with disabilities and $272 billion in reductions over 10 years across all welfare programs. These cuts would have a significant impact on the use of skilled nursing facilities for LTC under Medicaid, such that these services would shift to less expensive options such as assisted living, adult day care, and home-based services.
The CDC’s budget would be cut by 17% to $6.3 billion and the National Institutes of Health (NIH) by 18% to $26 billion and would include cutting: the National Cancer Institute by $1 billion; the National Institute of Allergy and Infectious Diseases by $840 million; and the National Institute of Diabetes & Digestive & Kidney Diseases by $355 million. In addition, the proposal would eliminate funding for the AHRQ and, instead, provide NIH with $272 million to implement similar initiatives, Modern Healthcare reports.8 The proposal also calls for the following cuts:
- 28% funding cut for CDC environmental health efforts, which would get $157 million;
- 18% funding cut for CDC global health program, which would get $350 million;
- 17% funding cut for CDC HIV/AIDS, sexually transmitted infection, and tuberculosis prevention programs, which would get $934 million
- 19% funding cut for CDC efforts to prevent chronic diseases and promote health; and
- 10% funding cut for CDC’s immunization and influenza preparation efforts.
FDA funding would be reduced by $854 million, although this funding cut would be offset by a projected $1.3 billion increase in FDA user fees. In addition, the budget calls for $29 billion in funding to extend the Veterans’ Choice Program.
Malpractice reform is also included in the budget such that awards would be limited to noneconomic damages at $250,000 indexed to inflation and implement a 3-year statute of limitations on medical malpractice claims. It is estimated that these reforms would save the federal government $55 billion over a decade, including $31.8 billion in savings for Department of Health and Human Services. Bottom line from the proposed budget is that LTC providers will be forced to develop less costly LTC options for patients.
LTC providers preparing for these changes will need to continue to provide value to their patients, organizations, and payers. The ability to improve the health for older adults will be a challenge for some, depending upon whether they are on the winning (insured and enjoying legislated, lower pharmaceutical costs) or losing (uninsured and entering Medicare sicker) end of what is still to come out of Washington, DC. In addition, these changes coming from the Trump Administration will be the driving force on the Medicaid side driving greater State control. All are certain to mean delivering more with less for LTC providers.
1. American Health Care Reform Act of 2017. HR277, 115th Congress (2017). https://www.congress.gov/bill/115th-congress/house-bill/277/text. Accessed May 17, 2017.
2. Improving Access To Affordable Prescription Drugs Act. HR1776, 115th Congress (2017-2018). https://www.congress.gov/bill/115th-congress/house-bill/1776. Accessed May 22, 2017.
3. Compilation of Patient Protection and Affordable Care Act. Healthcare.gov website. http://housedocs.house.gov/energycommerce/ppacacon.pdf. Published May 1, 2010. Accessed May 2, 2017.
4. Congressional Budget Office. American Health Care Act. https://www.cbo.gov/system/files/115th-congress-2017-2018/costestimate/hr1628aspassed.pdf. Published May 24, 2017. Accessed May 26, 2017.
5. 2016 Biennial Health Insurance Survey. The Commonwealth Fund website. http://www.commonwealthfund.org/interactives-and-data/surveys/biennial-health-insurance-surveys/2017/2016-biennial-health-insurance-survey. Published February 1, 2017. Accessed May 2, 2017.
6. Summary of the Improving Access to Affordable Prescription Drugs Act. Senator Elizabeth Warren website. https://www.warren.senate.gov/files/documents/2017 _3_29_Improving_Access_to_Affordable_Prescription_Drugs_Act_Summary.pdf. Accessed May 2, 2017.
7. Office of Management and Budget. Budget of the US Government: A New Foundation for American Greatness. White House website. https://www.whitehouse.gov/sites/whitehouse.gov/files/omb/budget/fy2018/budget.pdf. Published May 23, 2017. Accessed May 25, 2017.
8. Lee M. Hospitals worry about the 23 million that would lose coverage under AHCA. ModernHealthcare. May 24, 2017. http://www.modernhealthcare.com/article/20170524/NEWS/170529948/23-million-to-lose-insurance-under-house-gops-obamacare-reform-bill. Accessed May 25, 2017.
