

Cultural Influences in the Clinician–Elderly Nursing Home Resident Relationship
INTRODUCTION
Racial and ethnic differences in accessing and utilizing nursing home care have been clear from existing studies. While minorities of color have often been thought to shun nursing home care,1 the 1999 National Nursing Home Survey revealed otherwise (Table I). The rate of institutionalization per 10,000 elderly was comparable to, if not higher than, the rate for Caucasians with advancing age.2 This presents a demographic imperative for staff in nursing homes to understand diversity and deal with it more effectively.
Racial segregation still exists in nursing homes. The reason for segregation may be unintentional, but there is little external pressure to desegregate.3 Nursing homes are either predominantly minority or predominantly majority, like the “dominant” community.4,5 A segregated system is not “separate but equal.” It remains a two-class system of care. There is also evidence that facilities that are predominantly ethnic minority with residents of low socioeconomic class have poorer outcomes.4

Resistance to nursing homes may be especially strong among minority groups, partly because minority families may feel that available nursing homes are substandard. For example, Mexican caregivers in the Dallas-Fort Worth area expressed mistrust of nursing homes and questioned the quality of care their (older) family members would receive in these settings.6 Nursing home care also may not be affordable, which would delay placement as well.1
Surveys suggest there may be a stronger preference for care at home and a larger extended support network for many minority families. Involvement of families in care once a person is admitted to the nursing home may be more important among minority residents. A common fear is that staff will treat minority residents differently.6
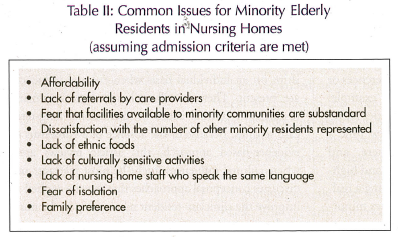
Staff must learn to deal with increasing diversity in nursing homes. Although there are more than 100 recognized ethnic groups or minority groupings, only five major racial distinctions (Asian, Hispanic, Black, White, Native American, and Pacific Islander) are recognized in the U.S. Census.7 From the last census, it is clear that most racial groups, other than African Americans, are first-generation (immigrant). Immigrant elderly may have language barriers and different lifestyle preferences or religious differences.8 New York is a good example. With more than 30 different ethnic minorities represented among the elderly population in New York, a growing number of elderly residing there, and desired assimilation, the trend for diversity and higher facility utilization by minorities is becoming a reality.9 Table II lists some of the common issues minority elderly face in the nursing home setting.
Taking a more microscopic view, the clinician must know how to improve the quality of care and relationships on an individual basis when cultural influences are present. There is still strikingly little systematic research on cultural issues in institutional long-term care settings. Because of the absence of a consensus or evidence-based approach, this article reviews areas where cultural influences might be most relevant, and discusses conceptual approaches that may be applied to improve the clinician–resident relationship in the nursing home setting.
WHEN MIGHT CULTURAL ISSUES BE IMPORTANT?
The National Institute of Mental Health (NIMH) Culture and Diagnosis Group described culture and ethnicity as related concepts. This was defined in the Diagnostic and Statistical Manual of Mental Disorders, fourth edition (DSM-IV), as follows:
Culture refers to meanings, values, and behavioral norms that are learned and transmitted in the dominant society and within its social groups. Culture powerfully influences cognitions, feeling, and “self” concept, as well as the diagnostic process and treatment decisions. Ethnicity, a related concept, refers to social groupings, which distinguish themselves from other groups based on ideas of shared descent and aspirations, as well as to behavioral norms and forms of personal identity associated with such groups.10
Generally, cultural issues may be expected to be more profound in immigrant populations or non-assimilated American-born populations that have experienced prejudicial treatment or exclusion.11 These issues may also be more pronounced if one is separated from one’s cultural reference group and “feels” different,12 such as being the only minority group member in a facility, or conversely, being the only majority group member in a minority facility. The same feeling of difference can apply to a minority clinician who deals with a resident from a different ethnic group, especially if the resident has prejudicial feelings about the clinician’s race. Thus, a white resident in a predominantly black nursing home, or a Jewish resident in a predominantly Catholic nursing home, or any number of similar possibilities, might engender a need for cultural sensitivity.
With immigrant populations, the most common cultural problems lie in: (1) communication barriers due to language; (2) noncompliance due to differing health care values and beliefs (ie, the resident will not listen to the clinician’s advice or make recommended lifestyle changes); and (3) bidirectional bias (by the clinician, the resident or the family, or both) caused by racial stereotyping or even outright prejudice.12 In addition, socioeconomic factors, such as the so-called “culture of poverty,” may have profound effects on knowledge, past risk factors for disease, and anxiety about medical care that need remedial work in health education by nurses.
HEALTH LOCUS OF CONTROL: A MODEL FOR HEALTH EDUCATION
Nursing home staff needs to be aware of cultural differences in attitudes about illness and accepting help. A convenient way to understand the behaviors of some minority elderly is captured by the notion of internal/external locus of control.
Individuals develop a belief that outcomes are either due to their own action (internal locus of control) or a result of outside factors, such as luck (external locus of control). This belief also applies to health. Many cultures seem to take a fatalistic view that good health or illness is due to luck: Why change one’s habits or diet or even lose weight? If doctors don’t or can’t reverse things by themselves, they are quacks. Wallston et al13-15 developed a health locus of control scale to measure the degree to which individuals believe that their health is controlled by internal or external factors. External locus of control is more prevalent in low socioeconomic and minority groups.16 An external health locus of control reduces the resident’s willingness to participate in health care decisions or monitor their health. Studies have shown that psychological distress is greater when there is a low level of personal control (ie, a high level of external health locus of control).17
A common tenet of psychiatry is that information and active coping skills help reduce anxiety. The therapeutic approach that staff should use has two steps. First, staff should let residents know that they recognize the residents’ point of view that they have no control over their own health at this point. Second, staff should help residents identify where they do have control through health education. This should empower residents to participate more actively in their care.
Similarly, culture and ethnicity play a role in the therapeutic relationship between the minority resident and the clinician in the nursing home. Staff can encourage participation of family or friends, other staff members of the same race/ethnicity/religion, or a “local healer” (including clergy), or they can allow alternative therapies (such as a home remedy).18
CULTURALLY APPROPRIATE SERVICES
It is difficult to use a single approach because of diversity, which exists even within a racial group. A useful clinical model is to anticipate common issues related to a resident’s distance from immigration or degree of assimilation, and perceived cultural identity (Table III).8
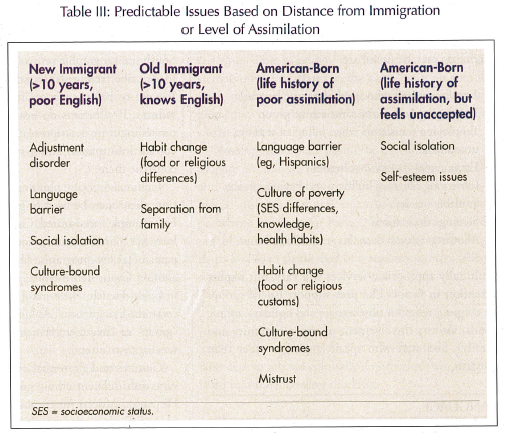
Because of the pattern of family unification, younger family members immigrate first to pave the way for their children and parents later. Elderly persons often enter the United States late in life, have limited English competency, and are reluctant to establish relationships outside their own culture. Since they are more likely to have “culture shock” (an adjustment disorder to America), they feel even more alienated in the nursing home setting.19
The culturally aware clinician must make a special effort to establish rapport and provide support. Involvement of family or key supports from the resident’s social network within the long-term care setting is needed. Community-based key informants who are knowledgeable about the ethnic minorities being served may serve as “culture-brokers.”20 Their services can help the clinician gain insight for understanding and accepting practices of their ethnic minority residents. Some culturally appropriate services that may be useful are:
• Employing staff who speak the same language
• Employing staff of the same ethnic group
• Employing translators when bilingual staff are unavailable
• Encouraging family involvement
• Observing religious holidays and having services available on site
• Serving ethnic foods
• Allowing cultural decor to personalize rooms
Culturally appropriate services will vary, but require attention to factors like peer support (social groups or cliques), religious observances and holidays, ethnic foods, visitors (involvement of the community and family), and staff who speak languages other than English.
LANGUAGE
For immigrant elderly persons, English is often the second language. In dementia, the second language is often forgotten, leading to communication difficulties. Poor English competency may even lead to avoidance of health care services.21
Employing bilingual staff, rather than using a family member or paid translator, is usually more comfortable for the resident. Residents often react to the interpreter initially as a cultural peer. A staff person will have more extended contact with the resident and allow a sense of greater involvement from the institution. For this reason, utilizing the services of a bilingual nurse or psychiatric worker as part of the treatment team is beneficial.22 A resident’s silence may be misconstrued as a sign of being uncooperative, depressed, paranoid, or cognitively impaired.23 Furthermore, stereotyping and misdiagnosis may lead to misinterpretation of behaviors as hostility or agitation.24 Even when communication is possible in English, idioms used by minority elderly individuals to describe feelings are often different and more difficult for younger clinicians to understand. For example, many African-American elderly persons use nonstandard English.23 Some who grew up in the South use geographic terms like “down in the valley” to describe feeling depressed. This is in contrast to the use of color, such as “feeling blue” to connote sadness. If clinicians do not understand the appropriate linguistic descriptors, they may fail to elicit the correct information about symptoms, or may misconstrue them.
Culturally-specific phrasing and patterns of expression must often be used to gain resident compliance. For example, an isolated Cajun resident would not leave her room with any amount of coaxing to participate in facility programs. She came out only when another Cajun staff member approached her and said in Cajun-French, “Mee-maw, come joint (sic) the others in the living room.” As long as it wasn’t labeled as a “group” or “treatment-centered” activity, the resident was happy to attend.
Gestures and nonverbal communication may also vary with different ethnic groups. Native Americans, Hispanics, African Americans, and Asians often seem more difficult to read because of the use of nonverbal communication that differs from Caucasians.23,25
MENTAL ILLNESS: DIAGNOSTIC CHALLENGES
It is often difficult to screen for or diagnose psychiatric problems in minority patients. While language difference is an obvious barrier, more subtle issues are different ways of communicating distress, conceptual differences about illness, or unwillingness to share information.26
The DSM-IV Outline for Cultural Formulation systematically details five distinct aspects of the cultural context of illness and their relevance to diagnosis and care.27 These aspects include the cultural identity (eg, reference group, language abilities, language use, and language preference); the cultural explanation of the illness; the psychosocial environment and levels of functioning; the cultural elements in the clinician–resident relationship, such as cultural or value differences; and an overall cultural assessment for diagnosis and care.
Culture and ethnicity influence whether symptoms are expressed behaviorally, somatically, or affectively.28 Resistance to disclosure of affect or feelings even applies to same-race providers, as in the case of a light-skinned African-American medical student’s interviews with a dark-skinned African-American nursing home resident. It took several sessions before depressive symptoms were acknowledged or before the underlying feelings of hesitancy emerged.29
There are also some rare differences in presentation of psychological distress called culture-bound syndromes that may be more prevalent in immigrant and poorly assimilated residents (ie, elderly). The DSM-IV Appendix on culture-bound syndromes includes a glossary listing of idioms of distress encountered in North American clinical practice. Gastrointestinal complaints, excessive gas, palpitations, and chest pain are common forms of somatization in Puerto Ricans, Mexican Americans, and whites.30 Some Asian groups express more cardiopulmonary and vestibular symptoms, such as dizziness, vertigo, and blurred vision.31 In Africa and South Asia, somatization sometimes takes the form of burning hands and feet, or the experience of worms in the head or ants crawling under the skin.32 Idioms of distress should not be considered as limited to one ethnic group. An erroneous diagnosis of panic or somatization disorder can occur when these idioms are misconstrued.33
Clinicians in nursing home settings should be aware of cultural variants in the expression of psychological distress. Competency in this area can avoid errors in diagnosis and the tendency to label residents as “attention-seeking” or somatically focused.
INTERRACIAL CARE
When medical and allied health professionals are predominantly white and/or culturally different from the minority or black elderly residents, the therapist–resident interaction can be fraught with misunderstanding. According to Watson,26 “Therapeutic relationships as interactive processes are as subject to ethnic and racial prejudice and discriminatory behavior as are other kinds of role relationships in society.”
Minority and nonminority staff may display differing support for their minority or nonminority counterparts among the mentally ill nursing home residents. This is evident in the residue of negative stereotyping. For example, the same behavior that is interpreted as aggression in an African-American resident may not be perceived the same way in a Caucasian resident.
Nursing home staff should be encouraged to participate in training programs that address cultural and ethnic differences in the expression of psychological distress. Cultural sensitivity training should be offered on a regular basis. Nursing homes should use bilingual staff to establish a rapport with residents and avail themselves of translator services when needed.
GUIDELINES FOR CLINICIANS TO PROVIDE CULTURALLY SENSITIVE CARE
The steps to achieve culturally sensitive care can be distilled into the following checklist:
1. Ethnic group is known, not just race; idioms for distress are known.
2. Immigration level of the patient is known (first-generation immigrant or later).
3. Cultural identity has been assessed; the cultural reference group is known (friends); English language abilities and English language use have been assessed; language preference is known.
4. Years since immigration is known (recent or not).
5. English competency is assessed; bilingual staff are available; translators are available.
6. Translated questionnaires are used if translators are not available (resident must be able to read).
7. History of prejudice or social exclusion due to race is known.
8. History of trauma is known.
9. Other residents from the same ethnic group live in the facility.
10. Other staff from the same ethnic group work in the facility.
11.The resident has been asked what he/she thinks is causing the illness (cultural explanation).
12. The family is appropriately involved (psychosocial network).
13. Rapport is sufficient for the resident to disclose information.
14. Culturally desirable decor is used in the nursing home.
15. Relevant religious services are held in the nursing home.
SUMMARY
Cultural factors strongly permeate the physician–resident interaction. This is particularly the case in long-term care settings, where residents’ interactions are often limited to their direct care staff. Further research on the impact of cultural issues in the long-term care setting is needed to provide an evidence-based approach to the care of ethnic minority elderly residents. Clinicians in long-term care settings should regularly participate in programs in which they can learn to identify the unique characteristics of older minority populations, and sensitively address issues of literacy, family support, the need for demonstrated respect, and alternative cultural remedies.34 Clinicians should be aware of cultural nuances in their dealings with minority elderly to establish rapport, and foster and strengthen the therapeutic alliance.
