

MEDICARE PART D UPDATE: Freedom of Speech
Imagine a physician diagnosing a frail senior patient with hypercholesterolemia, but instead of writing a prescription for the most appropriate statin for that specific patient, the physician is forced to give a list of all available treatment options—and let the patient make a decision on his or her own. Of course, no one knowledgeable about the healthcare system would ever allow this situation to develop. This decision would be too difficult for any patient to make, let alone a nursing home resident suffering some level of dementia, yet this is the situation that the Centers for Medicare & Medicaid Services (CMS) has set up when it comes to physicians and other providers directing their patients to the Medicare Part D plan that provides them the best access to those medications needed for that specific patient.
As a result of CMS marketing guidelines and direction to state surveyors, nursing home providers are unable to give their residents specific information as to the prescription plan that provides the greatest access to medications.
A QUESTIONABLE STANCE
In an effort to create an environment that promoted prescription drug plans to come into this new market, CMS wrote the rules so that there was an even distribution of members. While this may present the best opportunity for prescription drug plan (PDP) success, it does not bode as well for Medicare beneficiaries, especially the frail, dually eligible nursing home residents.
So, CMS wrote very restrictive guidance to nursing home providers regarding what they could not say about specific plans. But CMS did not stop with this guidance; they went further by providing state surveyors with a directive to monitor against facilities that directed residents to specific plans, despite whether this was actually in the residents’ best interest.
But who should direct residents to specific prescription plans? The answer for CMS is that residents should stay with the prescription plan that they were automatically enrolled in, although this strategy is questionable given that a report from the Office of Inspector General (OIG) found that only 18% of dually eligible elderly persons were automatically enrolled in plans that paid for all of the most common medications used by this group. In addition, the OIG found that 30% of the dually eligible elderly were assigned to plans that excluded 15% or more of the most common medications utilized by this group.1
Another option would be that prescription plans educate Medicare beneficiaries as to which plan is best suited for them, although this approach was also found to have major difficulties. The Government Accountability Office (GAO) determined that Medicare plans gave erroneous or incomplete answers twice as often as correct ones to seniors seeking drug benefit information.2
HIPPOCRATIC OATH
Unlike any other profession, physicians have an obligation to work for the health of their patients, and this can only be accomplished through physicians speaking freely to their patients. The Hippocratic Oath lays the foundation for physicians always acting in the best interest of their patients.
Physicians have an obligation to do their best for their patients; it’s unfortunate when obstacles are placed in the way of this goal. But that is exactly what is created by the CMS marketing guidelines. Given the potential benefit provided by healthcare providers and the difficulties already demonstrated when this important decision is left to chance, or when the prescription plans themselves do the directing, CMS should not only waive these restrictions but should give healthcare providers resources so they can promote the most appropriate plans to their Medicare patients.
NEXT
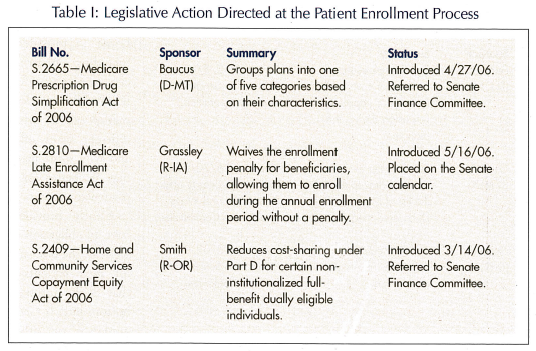
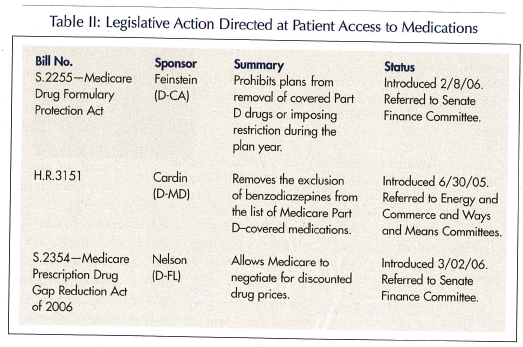
Despite the fact that there are still more than 50 pieces of legislation out to make changes to the Medicare Modernization Act (MMA), there are no pieces to correct these marketing restrictions. The current legislative landscape is littered with bills that would correct many of the issues that exist with regard to enrollment (Table I) and accessing medications (Table II), yet none get as basic as protecting providers’ freedom of speech in identifying the most appropriate plans for one’s patient.
At times, CMS seems to understand the importance of assuring that nursing homes work to maintain a one facility–one pharmacy relationship by providing LTC residents with the ability to change prescription plans through the special enrollment period to ensure that each resident is enrolled in the prescription plan that provides the greatest level of access to needed medications. These writings by CMS include guidance that “…an enrollee may choose an agent of the LTC facility, such as a registered nurse or case manager, to act as his or her appointed representative.”3 In addition, CMS has stated that nursing homes will be able to select from these (organizations that meet the CMS LTC pharmacy standard) pharmacy vendors to ensure that all of the residents have appropriate drug coverage.4 While these should provide some legal cover for nursing facilities providing guidance to their residents in their choosing the prescription drug plan that is best suited for them, CMS marketing guidelines to nursing facility providers makes these directives confusing.
CMS has provided some additional writings in the past that would allow providers to act in the best interest of their patients. CMS wrote that to the extent that a provider can assist a beneficiary in an objective assessment of the beneficiary’s needs and potential plan options that may meet those needs, providers are encouraged to do so. In addition, CMS also went on to state that “Obviously, we do not want pharmacies or any other providers steering beneficiaries into plans based upon the financial self-interest of the provider…this would not be in best interest of the beneficiary or the Medicare program.”5 Clearly, CMS does not want nursing home providers acting in a selfish manner, but the marketing guidelines go well beyond expected safeguards when they limit our basic constitutional right of freedom of speech.
Since changes regarding these restrictions are unlikely to come from the legislative side or within CMS independently, the legal system is likely to be the foundation of change. The Washington Legal Foundation released a brief on the issue by constitutional scholar Ronald Rotunda, calling into question CMS’s marketing guidelines as being unconstitutional because of its restrictions on the freedom of speech.6 CMS has decreed that it will not allow the nursing home providers, including pharmacies, to give truthful, nonmisleading information about what different plans offer and why some plans may be better for a particular resident.
Clearly, providers have an obligation to seek out the best care for their patients—that is the ultimate bottom line. If CMS guidance or other restrictions are put in the way, providers may need to work around those barriers to assure that their patients achieve their optimum health outcomes. Hopefully, this will be made easier when policy leaders turn to those with expertise in caring for the frail elderly for answers as to how best to design healthcare systems. Sadly, that does not appear to be the case at the present time.
Please send any questions or experiences about Medicare Part D you would like to share with readers to: BSpivack@Waveny.org
