


Psychopharmacology in the Elderly Person with Cardiovascular Disease
INTRODUCTION
Estimates from the American Heart Association indicate that cardiovascular disease is the leading cause of death in the United States, with 450,000 men and 550,000 women dying each year from heart disease.1 Eighty-five percent of these deaths occur in patients over the age of 65,2 a group that corresponds to the fastest-growing segment of the population in most western countries.3
Psychiatric disorders in the elderly are of significant prevalence. The estimated 4 million cases of mental illness in the elderly in 1970 is expected to increase to 15 million by 2030.4 Although mental illness includes such common conditions as anxiety disorders, sleep disorders and panic disorders, many of the therapeutic interventions in the elderly are directed toward depression, symptoms resulting from dementia and cognitive decline, and schizophrenia and related psychotic disorders. It is estimated that major depression affects 5-10% of older patients under the care of primary care physicians.5 Higher estimates of all depressive disorders in the elderly range from 12%-15%.6 Depression in the elderly is associated with significant morbidity, including impairment of the activities of daily living7 and decreased quality of life.8 Importantly, there is a significant correlation between cardiac disease and depression.2 Having either one of these diseases appears to increase the risk of acquiring the other.9 The prevalence of psychosis in the elderly population is estimated to be between 6% and 10%,10,11 and psychotic symptoms are present in 20-45% of hospitalized, elderly patients with depression and in 3.6% of depressed elderly individuals living in the community.7,11
With the substantial prevalence of concomitant psychiatric and cardiovascular disease in the elderly, pharmacologic management frequently involves treating the former while trying not to exacerbate the latter. Although newer antidepressants and antipsychotics in general offer improved side-effect profiles over their older counterparts, they are not devoid of potential adverse effects. In addition, polypharmacy (especially involving psychopharmacologic and cardiovascular agents) adds the concern of clinically significant drug-drug pharmacokinetic (PK) and pharmacodynamic (PD) interactions.10 A national survey of ambulatory U.S. adults found that more than 40% of those aged 65 years or older use 5 or more medications a week, and 12% use more than 10 different medications a week.12
This review addresses the major psychopharmacologic options available for the treatment of depression and psychosis, focusing on the challenges (including PK and PD issues) of treating elderly persons with comorbid cardiovascular disease.
PHARMACOKINETIC CONSIDERATIONS IN THE ELDERLY
An understanding of absorption, distribution, metabolism and excretion as they relate to the elderly is important for the appropriate choice of medication and dosage. These processes ultimately determine how much drug is in a patient’s body.
Absorption is unlikely to be significantly affected by the intrinsic physiology of aging. Some researchers believe that the rate of absorption of orally-administered medications is delayed in the elderly, due perhaps to decreased gastric pH, a decrease in the number of mucosal cells, a delay in gastric emptying time, a decrease in absorptive surface area, or a decrease in splanchnic blood flow.13 However, it appears that no significant age-related change truly occurs in individuals without gastrointestinal pathology.14
The extent of drug distribution or “volume of distribution,” however, does change with age.14 Specifically, elderly persons have a greater percentage of adipose tissue which increases the volume of distribution of lipophilic drugs, such as most psychotropic agents.15 Conversely, with a decrease in lean body mass in the elderly and a corresponding decrease in total body water, there is a decrease in the volume of distribution for hydrophilic drugs.16 Accordingly, the peak plasma concentrations for lipophilic drugs in the elderly can be decreased while peak levels for hydrophilic drugs can be increased, as compared to younger individuals.
The important PK principle of clearance is defined as the amount of blood, serum, or plasma from which a drug is completely removed per unit of time and is principally influenced by hepatic metabolism and renal excretion.15 A reduction in hepatic mass likely contributes to the observed age-related decline in the hepatic clearance of certain drugs.17 Plasma levels of drugs that are extensively “cleared” from the blood by the liver (such as some beta blockers and calcium channel blockers) may, accordingly, be higher in elderly patients.16,18 This overall decrease in hepatic blood flow can be exacerbated by heart failure or by drugs that reduce cardiac output, such as beta blockers.19 The extent to which the metabolic activity of specific hepatic enzymes involved in clearance declines with age remains the subject of active investigation. Metabolism occurs principally by the various members of the cytochrome (CYP) P450 superfamily of oxidative metabolizing enzymes (found predominantly in the liver and intestine). The most important P450 enzymes involved in the metabolism of currently available psychotropic drugs are CYP1A2, CYP2C9, CYP2C19, CYP2D6, and CYP3A4, with CYP2D6 and CYP3A4 being most important.20-22
In addition to the above PK considerations, the use of medications that may inhibit or accelerate (induce) the metabolic clearance of other coadministered drugs may lead to clinically significant PK interactions. Drug interactions can occur when CYP isoforms responsible for the metabolism of one drug are inhibited or induced by another drug. For example, the selective serotonin reuptake inhibitors (SSRIs) paroxetine and fluoxetine are known to be potent inhibitors of CYP2D6.23 Combining these drugs with a secondary tricyclic amine antidepressant (TCA) that depends upon CYP2D6 for its metabolism could lead to toxic accumulation of the TCA. CYP3A4 is the CYP isoform present in greatest amounts in humans, and is responsible for the metabolism of approximately 60% of drugs that undergo oxidation.24 Accordingly, pharmacologic modulation of CYP3A4 function can lead to untoward effects, such as drug interactions. Inhibitors of CYP3A4 function, such as erythromycin, clarithromycin, and ketoconazole should be given carefully to patients taking medications dependent upon CYP3A4 for their metabolism, such as the cardiovascular medications atorvastatin, nifedipine, verapamil, and amiodarone.24 CYP3A4 inhibitors will also decrease the clearance of important psychotropic medications such as the benzodiazepine alprazolam22 and the antidepressant trazodone.25
With aging, there is a decline in renal blood flow, renal mass, glomerular filtration, tubular secretion, and reabsorption, all of which cause a clinically relevant decline in renal elimination of drugs (and their metabolites) that are dependent upon renal excretion as the principal route of clearance.13,26 The time-course of drug disappearance after distribution is complete, referred to as the elimination half-life, depends upon both volume of distribution (proportionally) and clearance (inversely).15 For lipophilic psychotropic drugs taken by the elderly, an increase in the volume of distribution and a decrease in the clearance can increase the elimination half-life,10 ultimately leading to higher than intended drug exposure if dosing is not adjusted.
PHARMACODYNAMIC CONSIDERATIONS IN THE ELDERLY
Aging may impart changes that increase or decrease sensitivity to a pharmacologic agent. Specifically, PD changes in the elderly may manifest from changes at the receptor or signal-transduction level, as well as at the level of homeostatic equilibrium.18
Age-related changes at the receptor level can affect how drugs function in the elderly patient. For example, a decrease in response to beta blockers in the elderly has been reported, and is likely to be due to the downregulation of beta-adrenoceptors and the resulting decreased sensitivity to their effects.18
Aging can also lead to a decrease in homeostatic reserve that in turn intensifies the adverse effects of certain medications. Specifically, elderly patients demonstrate increased susceptibility to postural hypotension after taking drugs that lower arterial blood pressure.27 Syncope and falls are important sequelae of drug-induced orthostatic hypotension, a condition that occurs at a frequency of 5-33% in geriatric patients.18 The central nervous system is also increasingly vulnerable during aging to the effects of medications. The decrease in dopamine production and dopamine receptors seen in the elderly leads to an increased incidence of extrapyramidal symptoms with neuroleptic drug use (via dopaminergic blockade).18 There is also a high incidence of tardive dyskinesia, akathisia, and Parkinson’s syndrome in elderly patients taking chronic antipsychotic medications.18 Additionally, the changes in number and composition of the GABAA-benzodiazepine receptor complex with aging may be responsible for the heightened sensitivity to benzodiazepines (ie, sedation, confusion, and ataxia) in the elderly.28 A further example of increased drug effect sensitivity occurs with the TCAs that can cause more severe antimuscarinic effects in older patients (ie, agitation, confusion, memory impairment, and, ultimately, delirium).
A particularly important PD effect of aging concerns the cardiac QT interval (or “QTc” interval when corrected for heart rate), which can be prolonged by certain medications. The danger of such QT-prolongation is the development of life-threatening ventricular tachyarrhythmias, such as torsades de pointes and ventricular fibrillation. Cardiovascular conditions such as bradycardia and heart failure in the elderly can predispose elderly patients to the QT-prolonging effects of drugs, such as the antidpressants amitriptyline and imipramine, as well as the neuroleptics thioridazine and droperidol.29 PD drug interactions can occur when two or more QT-prolonging drugs are coadministered.30 The PK correlate to this effect would be the coadministration of a QT-prolonging drug and a drug that reduces the clearance of QT-prolonging drugs (through CYP enzyme inhibition, for instance).30 Examples of this PK effect include the pairing of haloperidol (a QT-prolonging drug) with paroxetine, fluvoxamine, or paroxetine, all of which can impair haloperidol clearance.30
ANTIDEPRESSANTS
Depression is the most common psychiatric disease in the elderly.31 Depression is not only common in patients with cardiovascular disease2 but is considered a risk factor for heart disease.32 In a study conducted by Frasure-Smith et al,33 16% of 222 patients evaluated one week after suffering an MI were diagnosed with major depression, a diagnosis that was associated with a 3.5-fold greater risk of cardiac mortality during the subsequent 6 months. Lespérance et al34 demonstrated similar 1-year mortality results in patients admitted for unstable angina. Additionally, it has been estimated that 33% of persons with myocardial infarction (MI) suffer from major depression during the first 12 months post-MI.35 Ranges of depression in persons with congestive heart failure span from 17-37%.36-38 Depression, it seems, confers a significant risk of mortality and morbidity when present in cardiovascular patients.39 Accordingly, the effective treatment of depression in elderly patients with cardiovascular disease is an important component of their medical management.
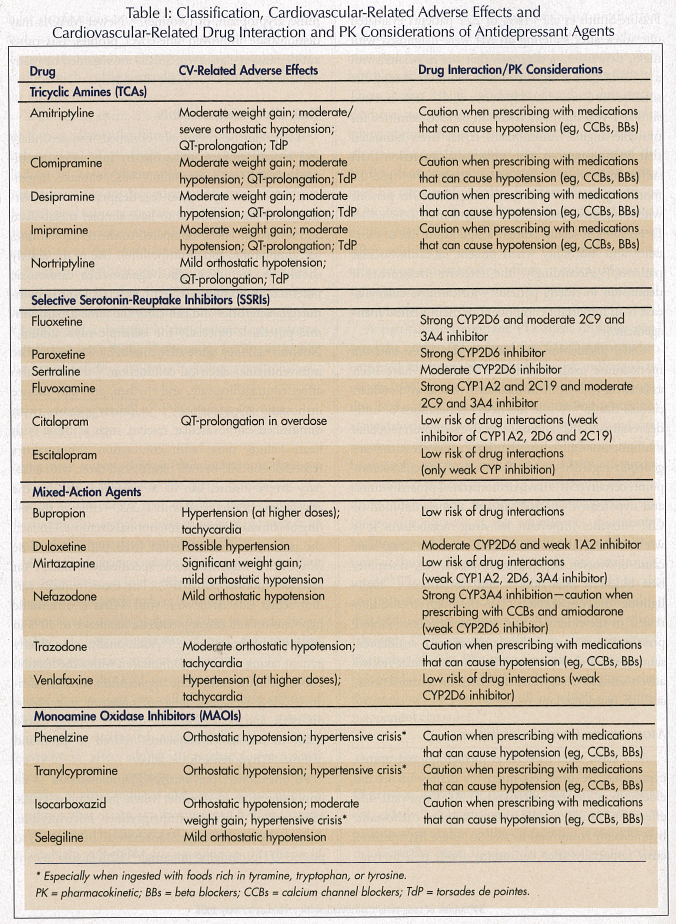
Older antidepressants (such as the TCAs and the monoamine oxidase inhibitors [MAOIs]) have been associated with both cardiac arrhythmias and sudden cardiac death.40 While the newer generations of antidepressants (SSRIs and nonselective serotonin reuptake inhibitors, or “mixed mechanism” antidepressants) are generally regarded as safer from a cardiovascular standpoint, certain SSRIs have demonstrated proarrhythmic and hypotensive effects,40 as well as the inhibition of CYP enzymes important for drug metabolism. It is worth noting that certain cardiovascular drugs can cause or worsen depressive symptoms (eg, reserpine, beta blockers, methyldopa, and clonidine),5,31 highlighting the importance of a thorough medication review of the elderly person with depression. (Table I presents a summary of the classification of antidepressant agents and their associated cardiovascular-related adverse effects, cardiovascular-related drug interactions, and PK considerations.)
Monoamine Oxidase Inhibitors
As a class, such MAOIs as phenelzine and tranylcypromine are used less often for depression in the elderly than are the SSRIs and TCAs. Untoward side effects of such medications include orthostatic hypotension (common) as well as severe hypertensive crisis (especially after consuming foods rich in tyramine, tryptophan, or tyrosine).41 Newer MAOIs may demonstrate improved side-effect profiles, but other antidepressant classes (eg, SSRIs) are regarded by many clinicians as safer choices for the elderly.
Tricyclic Antidepressants
TCAs can be chemically classified into secondary and tertiary amines, and work by inhibiting norepinephrine (NE) and serotonin (5-HT) reuptake. In general, the secondary amines (eg, desipramine and nortriptyline) are considered to have simpler metabolism and fewer side effects compared to the tertiary amines (eg, imipramine and amitriptyline). Use in the elderly should be carefully weighed against their cardiotoxic potential. Importantly, TCAs have class I antiarrhythmic characteristics and can carry the same proarrhythmic potential, especially for ischemic myocardium.9 Not only can they cause arrhythmias by slowing cardiac intraventricular electrical conduction,40 they may also affect contractility, rate, and rhythm, and may induce orthostatic hypotension.2,31,42 Elderly persons with diminished cardiovascular reserve, such as those with heart failure, those with conduction abnormalities (especially bundle branch block), and those with coronary artery disease, can be at particular risk for the adverse events associated with TCAs,43 either in the setting of clinical toxicity or intentional overdose.9 In fact, the postmyocardial infarction (MI) period is a time when TCAs may need to be specifically avoided44 (at least 2-3 months post-MI39). The most frequent cardiovascular side effect seen with TCAs is orthostatic hypotension and can approach an incidence of 50% in patients with heart failure.45 Additionally, in an elderly patient taking a TCA in conjunction with a medication known to cause orthostatic hypotension (such as calcium channel blockers, alpha-adrenoceptor antagonists, diuretics, and beta blockers), the PD synergy could result in serious consequences related to profound orthostatic hypotension (ie, falls).
As mentioned previously, QT-prolongation is an important issue to consider when prescribing TCAs. Medications such as amitriptyline, nortriptyline, desipramine, and clomipramine have all been shown to possess QT-prolonging potential.46 Risk factors to consider when prescribing these TCAs include the coadministration of drugs that inhibit TCA metabolism (such as the CYP2D6 inhibitor quinidine) or drugs with QT-prolonging potential.
Selective Serotonin Reuptake Inhibitors and Mixed-Mechanism Antidepressants
In general, the SSRIs and mixed-mechanism antidepressants (or “non-SSRI antidepressants”) have more favorable cardiovascular side-effect profiles compared to the TCAs and to the MAOIs. The SSRIs include citalopram, escitalopram, fluoxetine, fluvoxamine, paroxetine, and sertraline. The mixed-mechanism antidepressants include bupropion (a dopamine-norepinephrine reuptake inhibitor), venlafaxine and duloxetine (serotonin-norepinephrine inhibitors), nefazodone and trazodone (serotonin modulators), and mirtazapine (a noradrenergic and specific serotonergic antidepressant).
The PRevention Of Suicide in Primary care Elderly-Collaborative Trial (PROSPECT) algorithm recommends using an SSRI as first-line therapy in elderly persons with depression, with citalopram chosen as the drug of choice based on its safety profile.47 SSRIs produce fewer cardiotoxic, anticholinergic, and antihistaminergic side effects than do the TCAs,40 and are deemed safer choices for treating patients with ischemic heart disease.48 The SSRIs, however, are not free of cardiac side effects. Mild bradycardia has been documented with fluoxetine, fluvoxamine, and paroxetine.40 Additionally, fluoxetine use in a prospective cohort of elderly patients was found to be associated with a statistically increased risk of syncope (odds ratio [OR], 2.6; 95% confidence interval [CI], 1.8-3.5; P = 0.02).49 While case reports have also implicated SSRIs with arrhythmias, including atrial fibrillation, atrial flutter, bradycardia, supraventricular tachycardia, and heart block, when taken in total, the incidence of adverse cardiovascular events appears to be very low.39 In three studies by Glassman et al44 looking at SSRI use (fluoxetine, sertraline, and paroxetine) in patients with heart disease, no significant cardiovascular adverse events were seen, including blood pressure changes or orthostatic hypotension. Apparently, SSRIs do not negatively influence cardiac contractility44 or prolong the QT interval.48 Although more research is needed to clarify the issue, SSRIs appear to offer a generally safer alternative to the TCAs, especially for the elderly patient with cardiovascular disease.
The non-SSRI antidepressants also are not free of certain side effects. Along with the sedating effects of trazodone, significant orthostatic hypotension makes this non-SSRI antidepressant a potentially less attractive drug for the elderly (unless given at night, for example). Nefazodone may cause drug interactions through potent CYP3A4 inhibition (see below).20 Although venlafaxine and bupropion are generally well tolerated, venlafaxine can cause blood pressure increase at higher doses (200 mg per day or more).50
The administration of newer antidepressants (SSRIs and mixed-mechanism/non-SSRIs) that inhibit CYP enzymes necessary for the metabolism of coadministered drugs can lead to drug interactions. For example, paroxetine and fluoxetine are potent inhibitors of CYP2D6, which is responsible for the metabolism of many cardiovascular drugs, including calcium channel blockers (diltiazem, nifedipine, and verapamil), beta blockers and type IC antiarrhythmics (encainide, flecainide, mexiletine, and propafenone).39,51,52 The coadministration of a psychotropic drug that can inhibit CYP3A4, such as certain SSRIs (eg, fluvoxamine or fluoxetine) or the newer, non-SSRI antidepressant nefazodone, with a cardiovascular drug dependent upon CYP3A4 for metabolism (such as several calcium channel blockers, statins, and some antiarrhythmics) can potentially lead to significant drug interactions.52,53
Interestingly, there may actually be a cardiovascular benefit to SSRI therapy in patients with cardiovascular disease and depression via an inhibitory effect on platelet activation, with subsequent antithrombotic protection against MI.54 This benefit, however, is still theoretical and as yet unproven.
ANTIPSYCHOTICS
Antipsychotics (neuroleptics) are used for treating psychotic disorders (eg, schizophrenia and delusional disorders), as well as for, increasingly, the “off-label” treatment of such behavioral disturbances as agitation and aggression associated with dementia.55 Importantly, however, the FDA recently determined that atypical antipsychotic use for the off-label treatment of behavioral disturbances in elderly persons with dementia is associated with a significant increase (1.6- to 1.7-fold) in mortality as compared to placebo. Although the causes of mortality were varied, cardiovascular events (heart failure and sudden death) were the most frequent, along with infection.56 This decision was based upon clinical trials using aripiprazole, olanzapine, quetiapine, and risperidone. Accordingly, a Public Health Advisory was issued in April 2005 and “black box” warnings were added to all atypical antipsychotic medications to explain this risk, as well as the fact that they are not approved for use in elderly persons with dementia. A meta-analysis assessing increased mortality with atypical antipsychotic use (aripiprazole, olanzapine, quetiapine, and risperidone) in the elderly for delusions, aggression, and agitation with dementia similarly showed a small but increased risk of death compared with placebo (OR = 1.54; 95% CI, 1.06-2.23; P = .02).57 In a retrospective cohort study of Tennessee Medicaid patients from 1988 to 1993 taking moderate doses of essentially only older, conventional antipsychotics (less than 1% took the atypical agent clozapine), there was a 2.4-fold increase (95% CI, 1.77-3.22; P< .001) in the rate of cardiac sudden death as compared to similar patients not taking these medications.58 This rate climbed to 3.53 (95% CI, 1.66-7.51; P< .001) in moderate-dose cohort members with severe cardiovascular disease as compared to comparable nonusers.
This increased risk of death may extend to the conventional typical antipsychotics as well. A recent retrospective cohort study involving 22,890 patients 65 years of age or older who began taking conventional or atypical antipsychotic medications between 1994 and 2003 demonstrated significant increased risk of death with short-term (up to 180 days) conventional antipsychotic use.59 Conventional antipsychotic medications were associated with a 37% higher, dose-dependent risk of death when compared to atypical agents. Accordingly, the authors state that the results suggest conventional antipsychotics carry at least as much risk of mortality as atypical agents, and should not be used in their place (such as in reaction to the prior FDA warning).
Elderly persons with cardiovascular disease represent a high-risk population for the adverse effects of antipsychotic medications. Minor side effects include postural hypotension from alpha1-adrenoceptor blockade and tachycardia from anticholinergic blockade, while more serious consequences such as arrhythmias and sudden death are thought to be caused by the blockade of cardiac potassium channels (namely, hERG channels).60 Most antipsychotic agents (both conventional and atypical) have been found to cause QT-prolongation, and elderly patients with pre-existing heart disease are particularly vulnerable to this effect.21 Important drug interactions with antipsychotic use include the concomitant use of calcium channel blockers and diuretics that may predispose patients to QT interval prolongation and arrhythmias.55 In terms of metabolism, while CYP2D6 is significantly involved in the metabolism of TCAs and SSRIs, many antipsychotics are, in turn, inhibitors of CYP2D6 as well.61 CYP3A4 is important for the metabolism of high-potency antipsychotics.21
An important pharmacodynamic consideration of atypical antipsychotics is their potential to alter lipid and glucose homeostasis, as well as to cause significant weight gain. The result of these metabolic changes can worsen pre-existing cardiovascular disease, as well as create new cardiovascular risk factors. (Table II presents a summary of the classification of antipsychotic agents and their associated cardiovascular-related adverse effects, cardiovascular-related drug interactions, and PK considerations.)

Older, “Conventional” Antipsychotics
The conventional antipsychotics are commonly classified as low- or high- (and sometimes mid-) potency, according to their affinity for dopamine receptors. The low- potency typical antipsychotics (eg, chlorpromazine and thioridazine) are more likely than the high-potency antipsychotics (eg, haloperidol and fluphenazine) to cause cardiovascular side effects, such as significant orthostatic hypotension through alpha1-adrenergic blockade.55,62 The high-potency antipsychotics, however, tend to cause more extrapyramidal symptoms. There have been concerns linking thioridazine to QT interval abnormalities, ventricular tachycardia, and sudden death.63 Thioridazine and droperidol are known to be particularly problematic in terms of cardiac conduction (and each have black box warnings to that effect), as is the coadministration of QT-prolonging or potentially proarrhythmic drugs such as TCAs with most antiarrhythmic and antihypertensive drugs.21,60,64 There appears to be a greater association with thioridazine and sudden death compared to the other antipsychotics, as well as a common occurrence of QT interval prolongation.65 Chlorpromazine demonstrates some important drug interactions, namely increased hypotension when taken with ACE inhibitors, and an increased risk of ventricular arrhythmias when taken with amiodarone.66 In persons with cardiovascular disease, it appears that the high-potency antipsychotics (eg, haloperidol, flupenthixol, and fluphenazine) are safer choices with less anticholinergic and alpha1-blocking effects.
Newer, “Atypical” Antipsychotics
Members of the newer class of atypical antipsychotics include aripiprazole, olanzapine, quetiapine, risperidone, clozapine, and ziprasidone. These are less likely to cause unwanted extrapyramidal side effects, to cause tardive dyskinesia, or to raise prolactin levels as compared to the older, conventional antipsychotics.66 The atypicals have a strong affinity for dopamine (D2) receptors and are potent antagonists of the serotonin receptor.
Focusing on particular agents, elderly persons with cardiac disease may be more susceptible to clozapine’s side effects of orthostatic hypotension, tachycardia, and anticholinergic effects.67 Clozapine has demonstrated a causal relationship to cardiomyopathy and myocarditis, with an incidence in one series of at least 0.29%.68 Olanzapine appears to cause the least tachycardia, while clozapine causes the most.69 Postural hypotension is associated with both newer and older antipsychotics to roughly the same extent.69 Risperidone prolongs the QT interval and is contraindicated in patients with pre-existing cardiac disease, pre-existing QT interval prolongation, or those taking drugs known to prolong the QT interval. Risperidone has also been noted to cause postural hypotension, especially in cardiac patients.70 Quetiapine has been noted to cause hypotension as well as carry a risk for increased QT interval prolongation,71 but does not appear to affect hepatic enzymes function, resulting in fewer potential drug interactions.72 Ziprasidone has demonstrated a dose-related prolongation of the QT interval and is contraindicated in persons with known QT interval prolongation, with recent MI, or with uncompensated heart failure, and should not be given with QT interval-prolonging medications.67 Studies have shown that aripiprazole does not appear to prolong the QT interval and is associated with a reasonable safety profile.67
The relationship between atypical antipsychotic therapy and metabolic dysregulation is important for patients with cardiovascular disease. Studies show that atypical antipsychotics can elevate blood glucose and lipid levels (especially triglycerides), as well as cause significant weight gain, all of which can exacerbate cardiovascular disease. Olanzapine, clozapine, and quetiapine are particularly prone to cause such metabolic changes, as compared to risperidone and ziprasidone.73,74 Olanzapine and clozapine appear to cause the greatest weight gain.74 The exact mechanism of this weight gain is presently unknown, but it may be related to antagonism of the histamine H1 and serotonin receptors, or even increased leptin secretion.75,76
Clinical reports have implicated clozapine, olanzapine, and quetiapine with new-onset, insulin-resistant diabetes, and olanzapine and clozapine with ketoacidosis.74,77 FDA-conducted retrospective, epidemiologic surveys of spontaneously reported adverse events (MedWatch database), pooled with published cases of hyperglycemia or diabetes causally related to antipsychotic use, demonstrated the following findings: 384 cases were reported for clozapine (1990 to March 2001), 289 cases were reported for olanzapine (1994 to February 2002), 138 cases were reported for risperidone (1993 to February 2002), and 20 cases were reported for haloperidol (late 1970s to February 2002).78-80 A prospective study looking at 38,632 Veterans Affairs (VA) outpatients with schizophrenia over a period of 4 months found that for all ages, the odds of having diabetes were significantly higher for patients taking atypical agents as compared with conventional antipsychotics, specifically for clozapine, olanzapine, and quetiapine, but not for risperidone.81 A similar population case-control study of schizophrenics in the United Kingdom found that olanzapine use was correlated with a significantly increased risk of developing diabetes as compared with conventional antipsychotic use, while risperidone showed a nonsignificant increase.75 The mechanism of glucose dysregulation in patients taking antipsychotics is presently unknown, but may be due to more than the secondary effects of increased adiposity (especially given the incidence of hyperglycemia and diabetes in nonobese patients taking antipsychotics).75,78 The FDA issued a warning in October 2003 that the risk for hyperglycemia and diabetes was a potential concern for all atypical agents and recommended strict glucose monitoring for patients both before and after initiating treatment. The abundant data on weight gain, hyperlipidemia, hyperglycemia, and diabetes associated with atypical antipsychotic use (especially with clozapine and olanzapine) should alert the prescribing physician to closely and continuously monitor these metabolic parameters.
Atypical antipsychotics also appear to confer a risk for cerebrovascular events (strokes and transient ischemic attacks). The psychopharmacologic management of elderly persons with cardiovascular disease, having conditions such as atrial fibrillation, needs to take such increased cerebrovascular risk into particular account. Of the atypical agents, olanzapine and risperidone are most likely to add significant risk for cerebrovascular events.82 The FDA added warnings of increased cerebrovascular risk to the U.S. prescribing information for risperidone (April 2003), olanzapine (January 2004), and aripiprazole (February 2005).57 However, in a large, retrospective cohort study of stroke in atypical and conventional antipsychotic users (age 66 and older) from 1997 to 2002, olanzapine and risperidone showed no statistically significant increase in stroke risk compared to conventional antipsychotic users, raising the question of whether a difference in stroke risk truly exists between the two classes.83 Similar results were seen in another large, retrospective cohort study from 1997 to 2002, in which older adults (≥ 65 years) treated with high- and low-potency conventional and atypical (risperidone, olanzapine and quetiapine) antipsychotics for behavioral and psychological symptoms of dementia experienced no statistically significant different rates of ischemic stroke.84
AUGMENTATION REGIMENS AND EXPERT CONSENSUS
The combined use of antidepressants and antipsychotic therapies is sometimes encountered in “augmentation” strategies. Combining these two drug classes requires consideration of PK, PD, and interaction issues, especially in older patients with comorbid disease(s). Studies have shown that fluoxetine can increase risperidone levels by 75% (via CYP2D6 inhibition),85 fluvoxamine can increase thioridazine levels by 225% (most likely via dual inhibition of each other’s CYP metabolism),86 and fluvoxamine can increase clozapine levels approximately threefold (via CYP1A2 inhibition).87 The coadministration of the CYP2D6 inhibitors fluoxetine and paroxetine with the CYP2D6 substrate thioridazine could increase the blood levels of thioridazine and its potential for QT prolongation.43 Augmentation strategies for refractory depression may also include lithium, which is not metabolized by the liver but undergoes renal clearance. Caution should be exercised before initiating lithium augmentation in elderly persons with impaired renal function, or who take medications that may affect electrolyte balance or renal function.
An expert consensus panel of 38 geriatric psychiatrists and 14 geriatric internists/family physicians was surveyed in 2003 on its recommendations for antipsychotic use in older patients (65 years or older).88 For agitated dementia with delusions, its first-line treatment recommendation was risperidone, followed by quetiapine and olanzapine as high second-line options. (Antipsychotics were high second-line choices for agitated depression without delusions, as there were no first-line recommendations for that indication.) For “late-life” schizophrenia, risperidone was the first-line recommendation, while quetiapine, olanzapine and aripiprazole were high second-line options. In persons with diabetes, dyslipidemia, or obesity, the antipsychotics identified to be avoided were clozapine, olanzapine, and conventional antipsychotics (especially low- and mid-potency). The expert panel recommended that for persons with QT prolongation or congestive heart failure, clozapine, ziprasidone, and conventional antipsychotics (especially low- and mid-potency) should all be avoided. In persons with diabetes and dyslipidemia, the experts preferred risperidone, with quetiapine identified as their high second-line option.
CONCLUSION
Both cardiovascular disease and psychiatric disorders occur with significant frequency in the elderly. Adequate treatment of conditions such as depression and psychosis in the elderly is an important component of appropriate medical care. Both antidepressants and antipsychotics include newer and older generation agents. In general, the side-effect profiles of the newer agents are often viewed as more favorable, although some recent studies indicate that this distinction is somewhat unclear (especially for atypical antipsychotics). Both PK issues (such as CYP enzyme inhibition) and PD issues (such as cardiac toxicity and metabolic dysfunction) exist for many of these medications and should be considered whenever such drugs are administered. Careful prescribing of any of these agents is summarized and governed by the principle to “start low and go slow.”
Supported in part by grants AI-055412, DA-13209, DA-13834, DK/AI-58496, MH-58496, DA-05258, AG-17880, AT-01381, AI-58784, and RR-00054 from the Department of Health and Human Services, and by a grant from the National Institutes of Health. The authors report no relevant financial relationships.
