


Hematoma of the Lower Extremity: Operative Interventions in the Wound Clinic Setting
Dear Readers:
Hematoma in the soft tissue, a swelling in the tissue caused by bleeding, is not an uncommon occurrence following trauma or operative procedures. Hematomas of the extremities can be seen in as many as 33 per 10 000 individuals annually. Most hematomas are considered minor problems following the initial injury; however, accumulation of blood in the tissues can result in necrosis of the overlying skin due to increased tissue pressure. Even in the absence of increased tissue pressure, multiple cellular and biochemical changes that can result in tissue ischemia and necrosis have been identified. To avoid these significant complications, prompt recognition and operative evacuation of these hematomas should be performed. The author presents 2 cases of hematomas that were evacuated using local anesthesia in the wound clinic setting.
How Do I Cite This?
Treadwell T. Hematoma of the lower extremity: operative interventions in the wound clinic setting. Wounds. 2022;34(3):90-93. doi:10.25270/wnds/2022.9093
Introduction
Hematoma in the soft tissue, a swelling in the tissue caused by bleeding, is not an uncommon occurrence following trauma or operative procedures. Hematomas of the extremities can be seen in as many as 33 per 10 000 individuals annually.1 Most hematomas are considered to be minor problems following the initial injury; however, accumulation of blood in the tissues can result in necrosis of the overlying skin due to increased tissue pressure which occludes the subdermal and dermal capillaries.1,2 Even in the absence of increased tissue pressure, multiple cellular and biochemical changes that can result in tissue ischemia and necrosis have been identified.2-4 Platelets and white blood cells in the wound can release inflammatory cytokines, proteolytic enzymes, and toxic reactive oxygen species causing significant tissue damage.2 Iron ions present in the tissues from the lysis of the red blood cells and removal of hemoglobin molecules can cause a significant inflammatory reaction and thrombosis of the microvasculature.3,4 Some of these untreated hematomas do not resolve and can result in painful, fibrotic masses at the site of the previous injury (Figure 1).
Interestingly, studies have shown that wounds with hematomas of the lower leg are associated with increased mortality within 2 years of the injury.5,6 Prompt recognition and operative evacuation of these hematomas should be performed to avoid significant complications, and in the author’s experience, most evacuations can be done in the clinic setting. To provide an alternative option to surgical procedures in the operating room, this report presents 2 cases and additional examples of hematomas that were evacuated using local anesthesia in the wound clinic setting.
Case 1
A 74-year-old male with diabetes mellitus, who was taking antiplatelet agents, sustained an injury to the right leg in a motor vehicle accident 1 week before presenting to the wound center (Figure 2A). At the time of initial evaluation in the emergency department (ED), an abrasion and swelling of the leg were noted. The patient self-reported that he was prescribed antibiotic cream to apply to the abrasion and was told the problem would resolve. One week after receiving the cream, the patient presented to the wound clinic with worsening leg swelling and pain. The wound was found to have 2 areas of skin necrosis at the site of the original injury and a 9-cm underlying hematoma that was visibly enlarging. In the same visit, the hematoma was evacuated under local anesthesia (Figure 2B), and 2 bleeding points found in wound bed were controlled with sutures and oxidized regenerated cellulose (ORC)/collagen/silver dressings. One week after the hematoma was evacuated, the condition of the wound and patient’s quality of life had significantly improved. At 12 weeks following the procedure, the wound was healed (Figure 2C).
Case 2
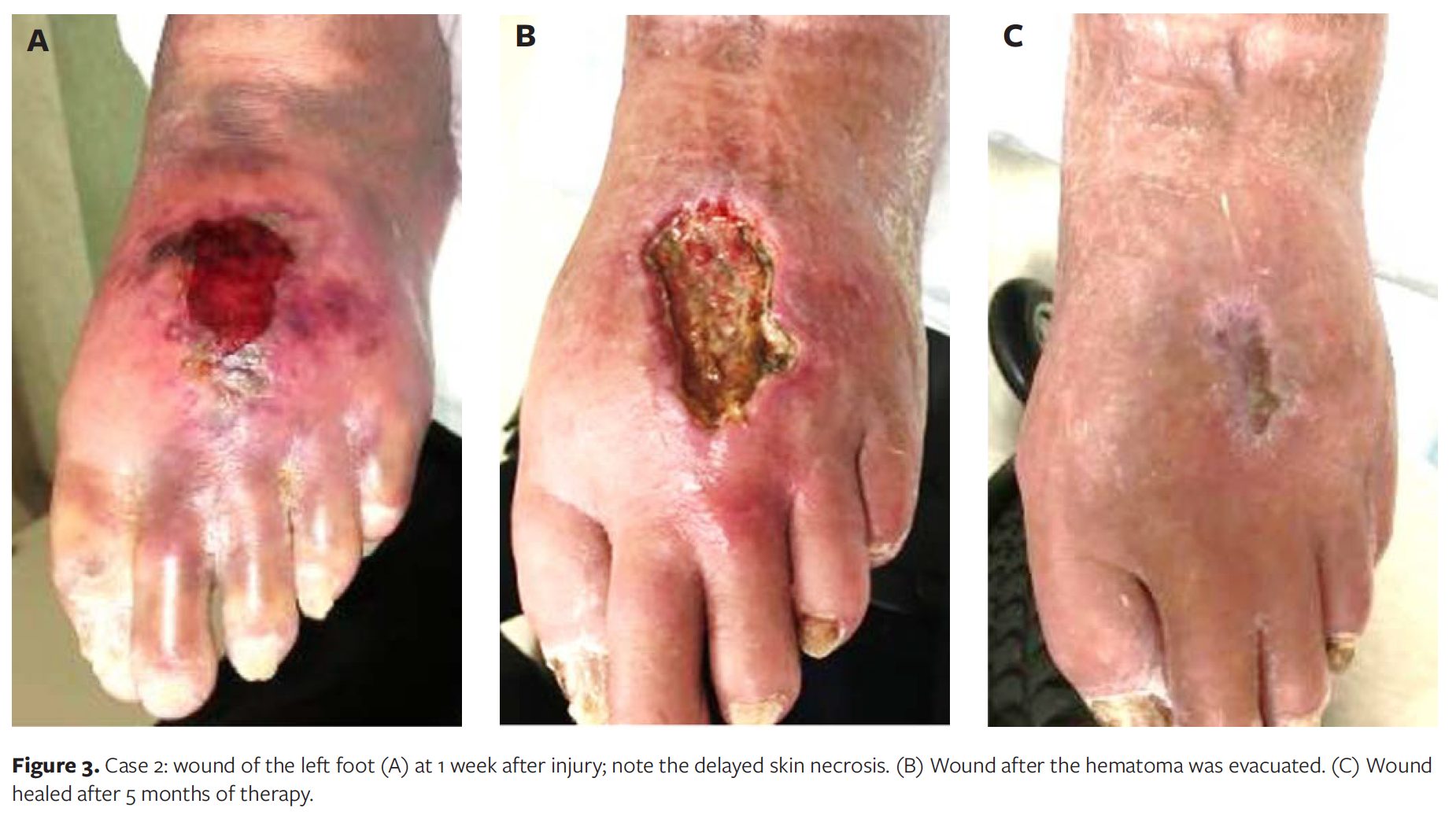
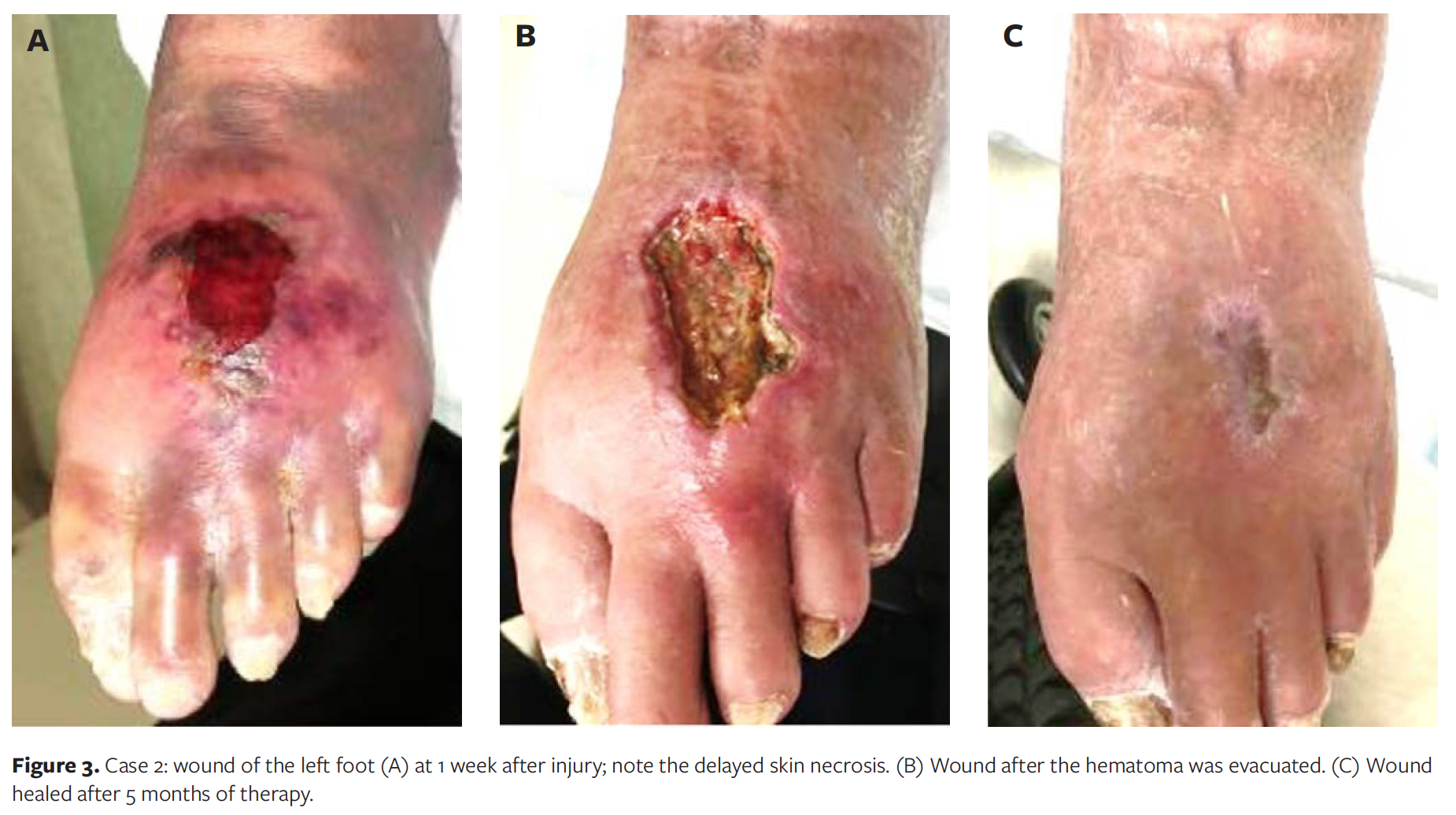
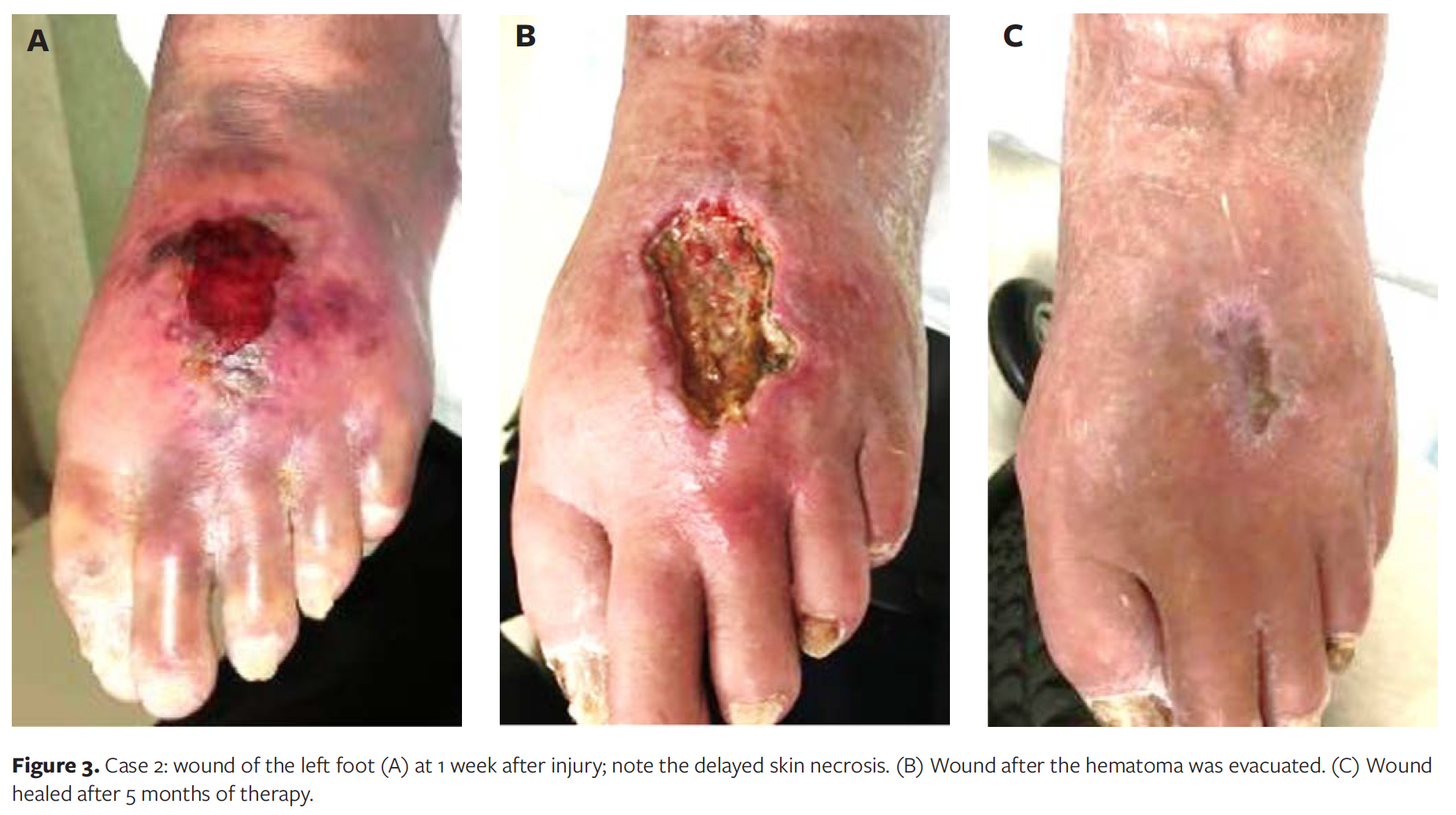
A 91-year-old male sustained an injury to the left foot after dropping a quart-sized jar of soup on his foot. The patient presented to the ED where the foot was noted to be bruised. X-ray examinations were reported to be negative, and there was normal circulation in the foot. The patient was seen by a physician in the ED, an orthopedic surgeon, and his primary care physician; the patient said he was informed that the swelling of the foot as well as blistering and necrosis of the skin would heal without treatment. After 1 week, the patient presented to the wound clinic with increasing skin necrosis and swelling of the left foot (Figure 3A). A hematoma of the foot measuring 6 cm in diameter was found. The necrotic tissue was debrided, and the hematoma was evacuated under local anesthesia (Figure 3B). One month after starting treatment with ORC/collagen/silver, after presentation and evacuation of the hematoma, the patient developed cardiac problems requiring hospitalization. After hospital discharge 1 week later, the foot was healing well, but a stage 3 presacral pressure injury had developed. After 5 months of therapy with debridement and applications of ORC/collagen/silver dressings on both wounds, wound healing was achieved (Figure 3C).
Clinical Significance
While generally considered innocuous, hematomas of the extremity following operative interventions or trauma can pose as a detriment to the patient. Without prompt treatment of the hematoma, progression and worsening of the wound can occur, resulting in significant delay of wound healing and potential long-term consequences. Operative evacuation of these hematomas can be performed using local anesthesia in most wound clinics.
Discussion
Hematomas of the extremity following operative intervention or trauma may occur in patients with thinner skin (patients >65 years, patients on corticosteroids) and those taking any variety of anticoagulant medications.1 Hematomas should not be taken lightly because their presence in a wound or site of injury increases the chance of infection and worsening of the tissue damage.1,2
Pressure on the surrounding tissues from the hematoma (Figure 4) can be significant. The patient in Figure 4 had a tight hematoma of the right leg after falling. At presentation, the leg was determined to be bruised, but, according to the patient, the treating clinician said there was no need to be concerned. The wound image captured 2 weeks after injury demonstrates the effect of the pressure of the hematoma on the overlying skin, resulting in necrosis of significant areas of the skin (Figure 4). There is concern that patients may experience continued bleeding into a hematoma, especially those taking anticoagulants like the patient in case 1.
Figure 5 illustrates a hematoma that developed in a repaired laceration. To avoid potential infection and delayed wound healing, hematomas developing in operative wounds (Figure 6) should not be ignored.
It has been shown that blood breakdown products and iron in the tissues can result in significant tissue damage if not treated, further supporting the need to evacuate these blood collections.1-4 Long-term complications as seen in Figure 1 and other more serious ones (eg, cases presented herein and those in the references) need to be avoided if possible.1,5,6
Summary
Evacuation of these hematomas should be performed as promptly as possible to facilitate healing of the wound and to avoid other potential complications.1,5,6 In the author’s experience, most hematomas can be safely, operatively evacuated in the wound clinic setting using local anesthesia as seen in the cases presented. If a particular case is not amenable to outpatient treatment, prompt treatment in the operating room is indicated. The treatment location should be chosen based on the patient’s needs and condition and the skill of the providers in the wound clinic.
Acknowledgments
Authors: Terry Treadwell, MD, FACS, FAAWC
Affiliation: Institute for Advanced Wound Care, Montgomery, AL
Disclosure: The author discloses no financial or other conflicts of interest.
Correspondence: Terry Treadwell, MD, FACS, FAAWC, Medical Director, Institute for Advanced Wound Care, Montgomery, AL; tatread@aol.com
Recommended Citation: Treadwell T. Hematoma of the lower extremity: operative interventions in the wound clinic setting. Wounds. 2022;34(3):90-93. doi:10.25270/wnds/2022.9093
References
1. Thompson-McHale S. Haematomas: management and treatment. Wound Essentials. 2015;10(1):24–28.
2. Glass GE, Nanchahal J. Why hematomas cause flap failure: an evidence based paradigm. J Plast Reconstr Aesthet Surg. 2012;65(7):903–910. doi:10.1016/j.bjps.2011.12.014
3. Caggiati A, Rosi C, Casini A, et al. Skin iron deposition characterizes lipodermatosclerosis and leg ulcer. Eur J Vasc Endovasc Surg. 2010;40(6):777–782. doi:10.1016/j.ejvs.2010.08.015
4. Wright JA, Richards T, Srai SK. The role of iron in the skin and cutaneous wound healing. Front Pharmacol. 2014;5:1–8. doi: 10.3389/fphar.2014.00156
5. Rees LS, Chapman T, Yarrow J, Wharton S. Long term outcomes following pretibial injury: mortality and effects on social care. Injury. 39(7):781–785. doi:10.1016/j.injury.2007.08.025
6. Thompson WL, Pujol-Nicolas A, et al. A kick in the shins: the financial impact of uncontrolled warfarin use in pre-tibial haematomas. Injury. 2014;45(1):250–252. doi:10.1016/j.injury.2012.07.007
Sign Up Today





{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
