


Use of a Novel Silicone-Acrylic Drape With Negative Pressure Wound Therapy in Four Patients With Periwound Skin Breakdown
Abstract
Introduction. Negative pressure wound therapy (NPWT) is applied using a foam dressing and an adhesive acrylic drape to create a seal. Removal of this drape can be painful and may play a role in periwound skin breakdown during dressing changes. A novel silicone-acrylic hybrid drape (HA-drape) has been developed for use with NPWT to allow for repositioning after initial placement and easier removal. Objective. This retrospective case series reports on the use of HA-drape in 4 patients who experienced periwound skin breakdown. The goal was to minimize skin breakdown while maintaining a seal on the dressing. Materials and Methods. Four patients with mild to moderate periwound skin breakdown were selected to receive NPWT with HA-drape. Negative pressure wound therapy was applied using a reticulated open cell foam dressing followed by placement of HA-drape to create a seal. Negative pressure wound therapy was initiated at -125 mm Hg with dressing changes occurring every 2 days. Wound healing, periwound healing, and patient-reported pain were assessed at dressing changes. Results. All 4 patients showed significant periwound skin improvement after the first dressing change. All patients reported a decrease in pain with dressing removal. Conclusions. In these 4 patients' wounds, use of NPWT with HA-drape resulted in intact periwound with improved periwound skin healing and reduction in patient-reported pain associated with dressing changes.
How Do I Cite This?
Greenstein E, Moore N. Use of a novel silicone-acrylic drape with negative pressure wound therapy in four patients with periwound skin breakdown. Wounds. Published online September 14, 2021. doi:10.25270/wnds/091421.01
Introduction
The use of medical adhesives in patient care has increased; however, their effect on the periwound skin is often overlooked.1 The application and removal of medical adhesives can result in medical adhesive-related skin injury (MARSI) that is frequently worsened with adhesive and dressing removal and reapplication.2
Negative pressure wound therapy (NPWT), commonly used in wound care, is applied with a foam dressing and a polyurethane drape with an acrylic adhesive to create a negative pressure seal.3,4 Removal of this drape can be painful and may play a role in periwound skin breakdown during dressing changes. A novel silicone-acrylic hybrid drape (HA-drape) consisting of a polyurethane film with acrylic adhesive and a silicone perforated layer has been developed for use with NPWT to allow for drape repositioning following initial placement and easier drape removal. In a recently published study, periwound skin in patients treated with NPWT and HA-drape showed no skin irritation or other complications, indicating that HA-drape can be used with minimal complications.5 The present case series reports on the use of HA-drape in 4 patients in whom periwound skin breakdown developed, with the goal of minimizing periwound skin breakdown during NPWT while maintaining a negative pressure seal on the dressing.
Materials and Methods
Four patients with chronic wounds presented to the hospital for care in June 2019. Wounds were assessed and surgical debridement was performed as necessary. Negative pressure wound therapy (V.A.C. Therapy; 3M) was applied using a reticulated open cell foam (ROCF) dressing (V.A.C. Granufoam Dressing; 3M) and traditional adhesive acrylic drape (V.A.C. Drape; 3M). The traditional adhesive acrylic drape was used to seal the ROCF dressing and was applied according to the manufacturer’s instructions. Negative pressure wound therapy was initiated at -125 mm Hg. Dressing changes occurred every 2 days. Wound improvement and periwound skin condition were monitored. After 2 days, mild to moderate periwound skin breakdown had developed in all 4 patients and treatment was switched to NPWT with HA-drape (DERMATAC Drape; 3M). Negative pressure wound therapy was applied utilizing the ROCF dressing followed by placement of HA-drape to create a negative pressure seal. Using the manufacturer’s instructions, HA-drape was placed to seal the ROCF dressing. Negative pressure wound therapy was initiated at -125 mm Hg with dressing changes occurring every 2 days. Wound healing, periwound condition (irritation, redness, and skin breakdown), and patient-reported pain were assessed at dressing changes. The periwound was defined as the 4 cm of skin extending around the wound. Patients provided written consent for use of data and images. This case series did not need Institutional Review Board approval due to the small number of patients included in this retrospective case study.
Results
Patient demographics and outcomes
Four patients presented to the hospital for wound care (Table). Patient age ranged from 62 years to 77 years. Previous medical history included above-knee amputation, paraplegia, and previous surgery. Advanced age placed the patients at increased risk of the development of MARSI during wound care.
Development of healthy granulation tissue was observed with NPWT and traditional drape usage. However, periwound skin breakdown (erythema and irritation) was observed in all patients as well as patient-reported pain at dressing changes. Wound care treatment was changed to include the use of HA-drape with NPWT and ROCF dressings to help protect the periwound skin during NPWT. Following the change to HA-drape, all 4 patients showed significant periwound skin improvement after the first dressing change along with continued development of wound bed granulation tissue. All patients reported a decrease in pain with dressing removal following use of HA-drape.
Case Presentation
Case 1
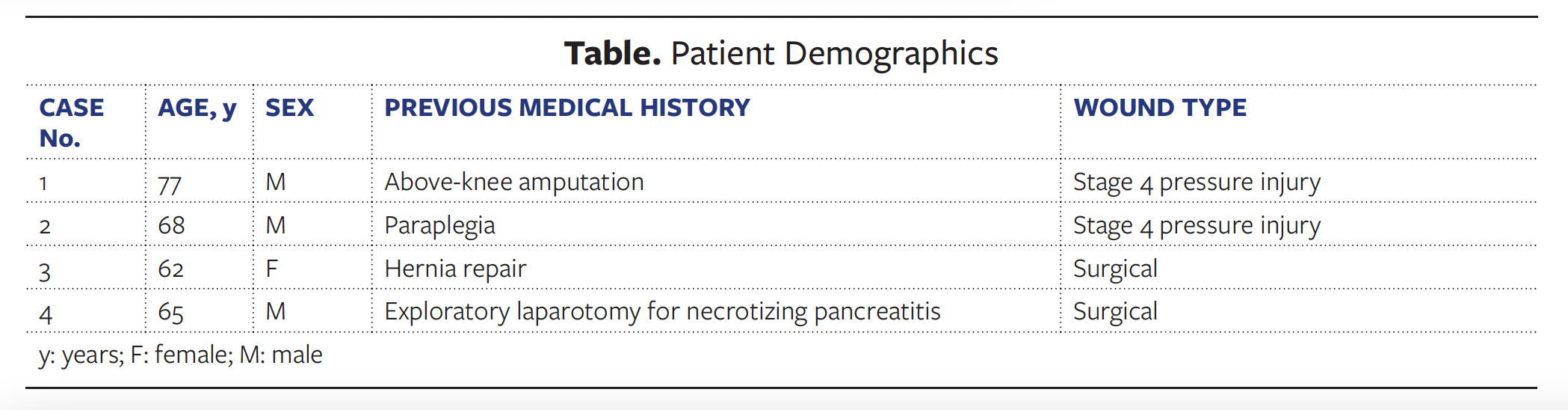
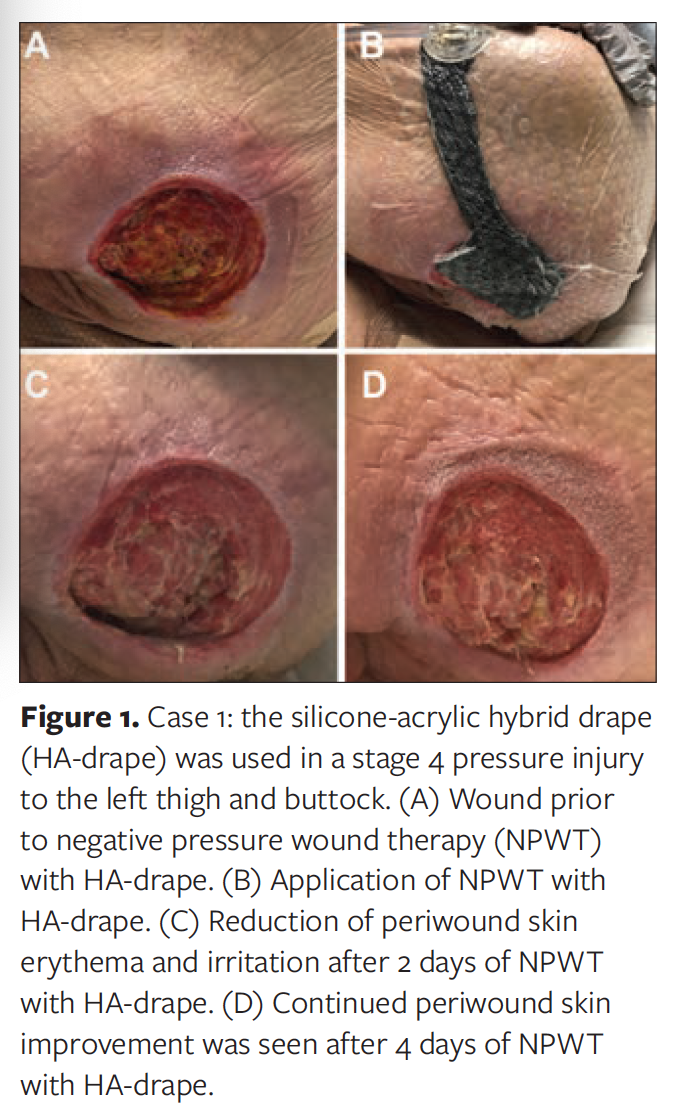
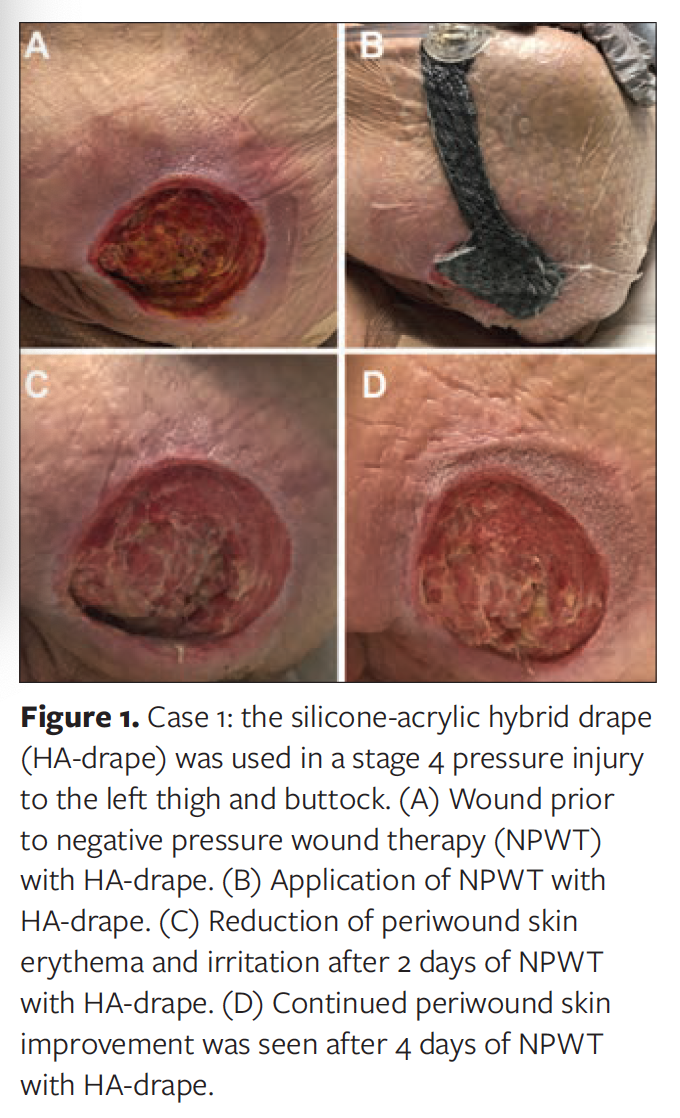
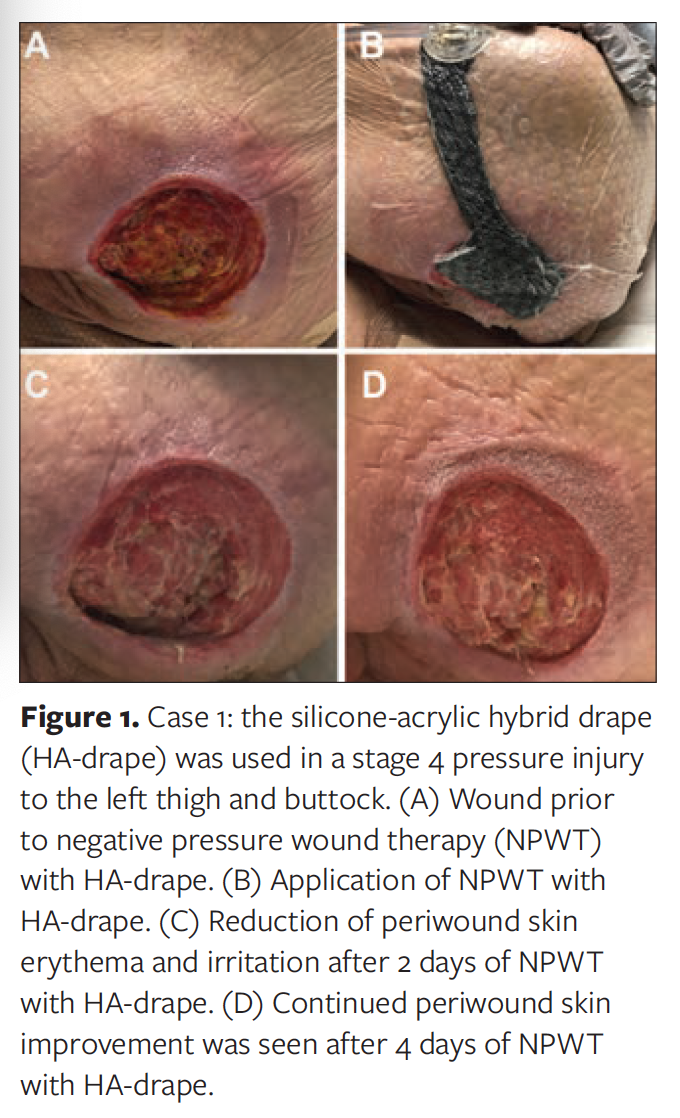
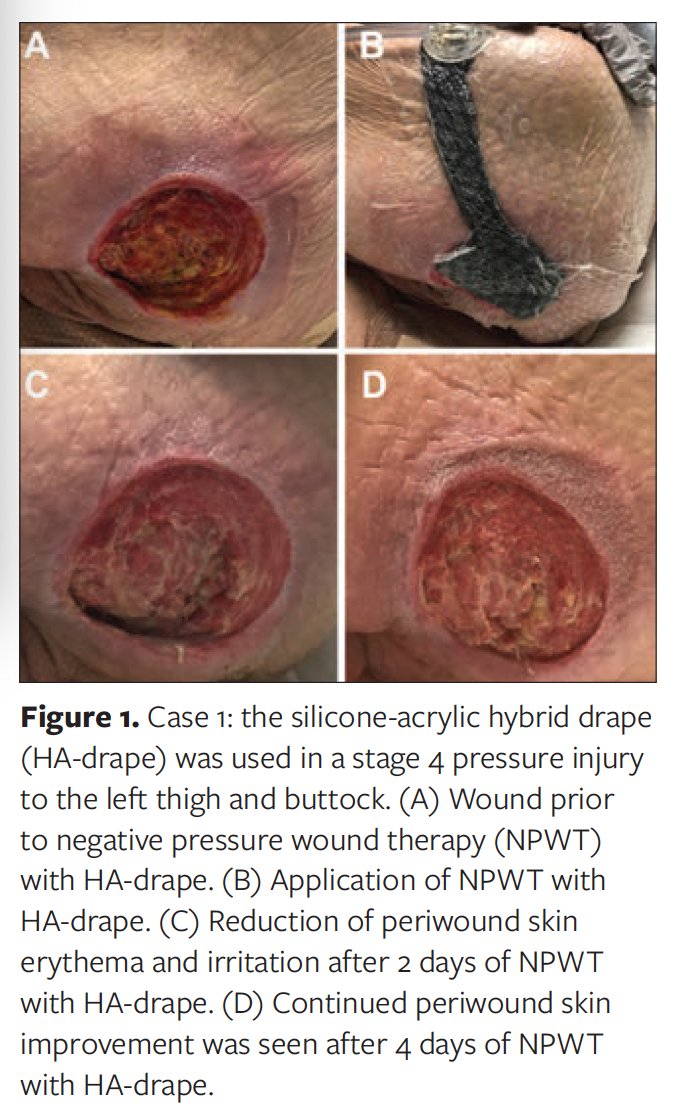
In a 77-year-old male with a history of above-knee amputation, a stage 4 pressure injury developed in the left thigh and buttock following prolonged sitting resulting from the previous amputation. Surgical debridement was performed, followed by application of NPWT with ROCF dressing and traditional drape, with dressing changes every 2 days. Initial NPWT use resulted in the development of periwound skin erythema and irritation (Figure 1A). Treatment was changed to NPWT with ROCF dressing and HA-drape (Figure 1B). Dressing changes occurred every 2 days. After 2 days of NPWT with HA-drape use, a reduction in periwound skin erythema and irritation was noted (Figure 1C). The periwound skin continued to show improvement throughout the period of NPWT with HA-drape use (Figure 1D). Unfortunately, the patient died of natural causes prior to wound closure. The patient’s death was not related to the use of NPWT.
Case 2
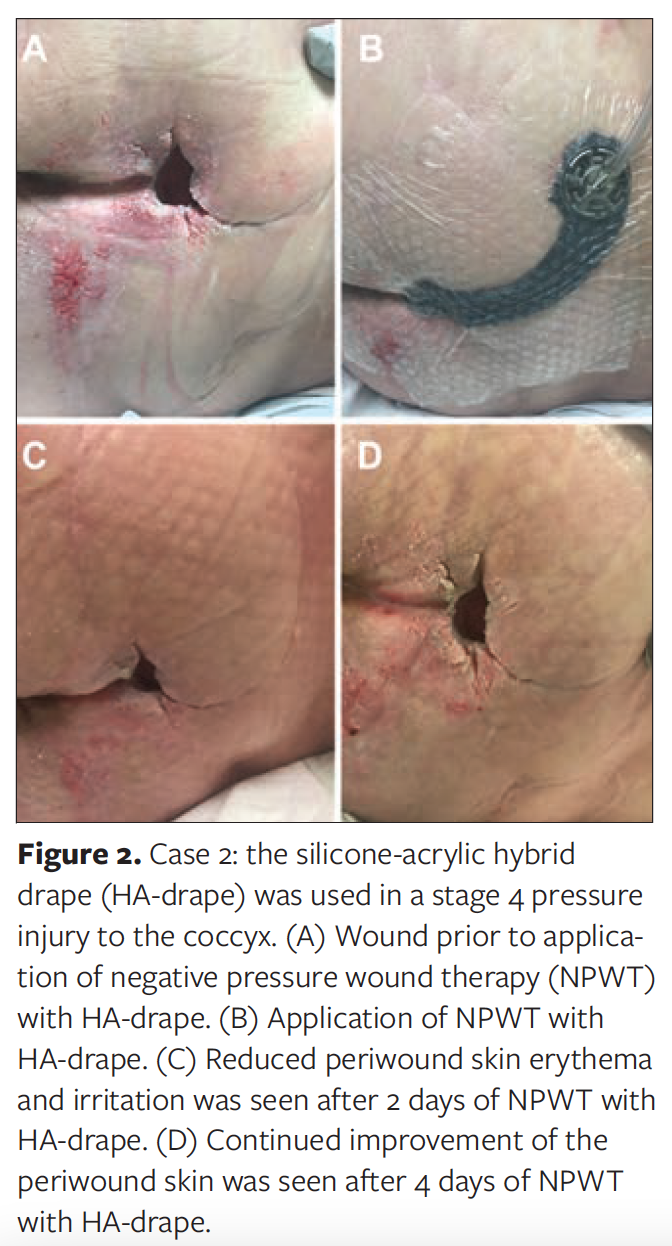
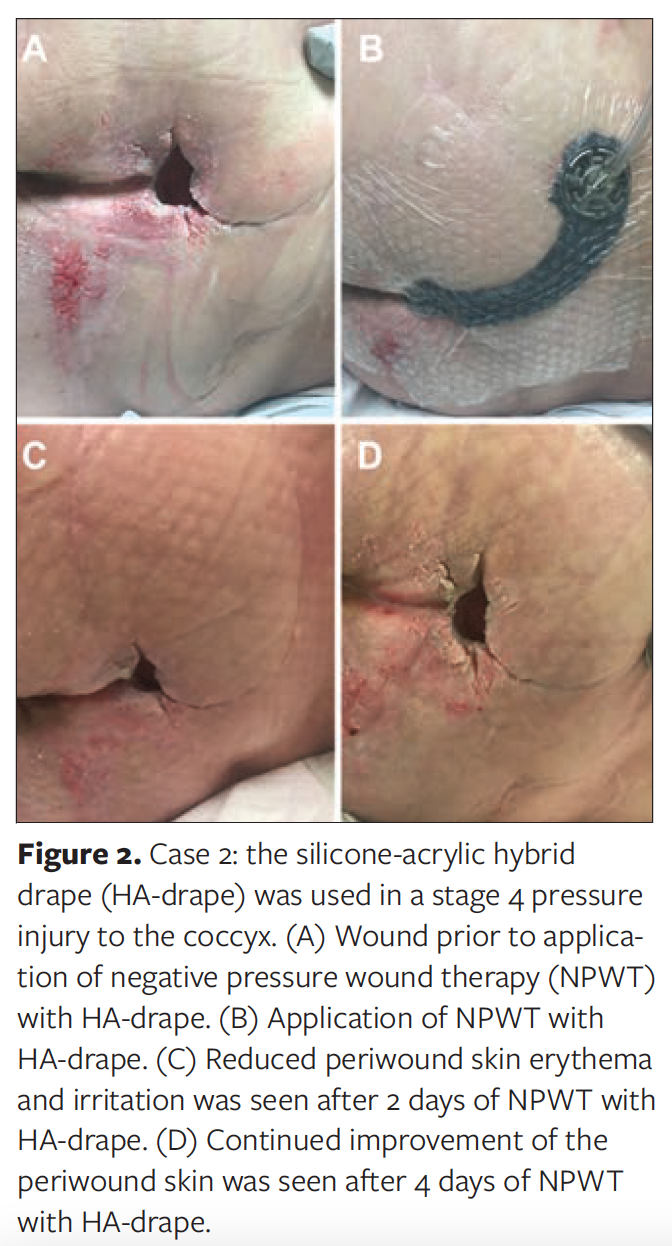
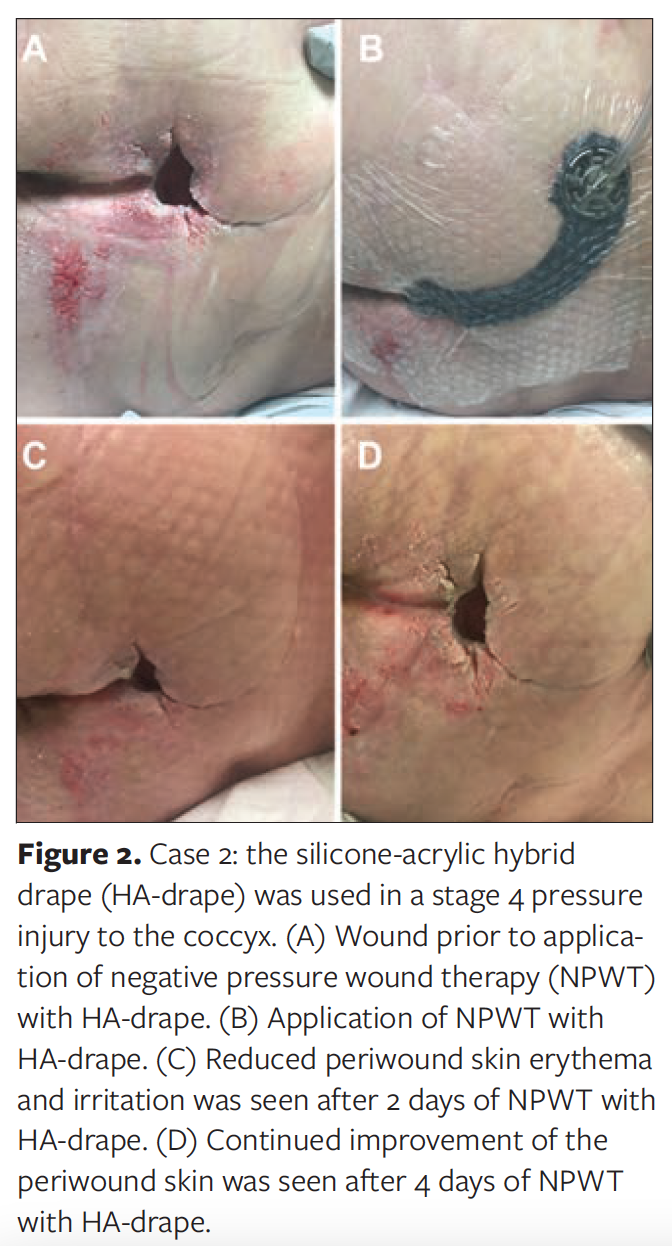
In a 68-year-old male with a history of paraplegia, a stage 4 pressure injury to the coccyx developed following a failed rotational flap placement. Negative pressure wound therapy with ROCF dressing and traditional drape was applied with dressing changes every 2 days. However, initial NPWT use resulted in periwound skin erythema and irritation (Figure 2A). Treatment was switched to NPWT with ROCF dressing and HA-drape, with dressing changes every 2 days (Figure 2B). After 2 days, periwound skin erythema and irritation were reduced (Figure 2C). The periwound skin continued to improve throughout the period of NPWT with HA-drape use (Figure 2D). After 4 days of NPWT, the patient was approved for a rotational flap procedure; however, the patient was lost to follow-up.
Discussion
The use of advanced wound care modalities with medical adhesives can increase the patient’s risk of the development of MARSI and exacerbate periwound skin irriation.1 One commonly used advanced wound care modality is NPWT, which has required the use of a polyurethane drape with an acrylic adhesive to create a negative pressure seal.3,4 However, this drape cannot be removed and repositioned after initial placement, and can be painful to remove during dressing changes. As such, a new hybrid polyurethane drape with acrylic adhesive and a silicone perforated layer has been developed for use with NPWT.
This 4-patient case series evaluated the use of NPWT with ROCF dressing and HA-drape in patients with periwound skin breakdown. In all 4 patients, periwound skin irritation improved with use of HA-drape. Additionally, compared with NPWT with traditional drape dressing changes, patients reported a reduction in pain during drape removal with HA-drape.
To date, only one article has been published regarding the use of NPWT with HA-drape, which evaluated the use of NPWT with HA-drape in complex wounds in 6 patients.5 No periwound skin irritation or complications were observed in any of the patients throughout the treatment period.5 As such, Fernández et al5 recommended NPWT with HA-drape use in patients at higher risk of the development of MARSI. The results of the current study align with the previous findings. At the first dressing change after HA-drape use was initiated, periwound skin irritation was reduced in all patients in this small case series.
Limitations
The small number of patients and lack of currently available literature are limitations of this case series. Additionally, all patients in this study were older; as such, the age range of the cases in this study may not be reflective of the entire wound care population due to differences in skin fragility and risk for development of MARSI. Large-scale, comparative studies are required to fully assess the effects of NPWT with HA-drape use in the population at risk for MARSI and the general wound care population.
Conclusions
In this retrospective case series of 4 patients, use of NPWT with ROCF dressing and HA-drape resulted in intact periwound with improved periwound skin protection and reduced patient-reported pain associated with dressing changes.
Acknowledgments
The authors thank Julie M Robertson, PhD (3M), for assistance with manuscript preparation and editing.
Authors: Emily Greenstein, APRN, CNP; and Nancy Moore, MSN, RN, CWON
Affiliation: Sanford Medical Center Fargo, Fargo, ND
Correspondence: Emily Greenstein, APRN, CNP, Sanford Medical Center Fargo, Wound Care, 801 N Broadway, Fargo, ND 58078; emily.greenstein@sanfordhealth.org
Disclosure: Ms Greenstein is a paid consultant for 3M.
References
1. Fumarola S, Allaway R, Callaghan R, et al. Overlooked and underestimated: medical adhesive-related skin injuries. J Wound Care. 2020;29(Sup3c):S1–S24. doi:10.12968/jowc.2020.29.Sup3c.S1
2. Collier M. Minimising pain and medical adhesive related skin injuries in vulnerable patients. Br J Nurs. 2019;28(15):S26–S32. doi:10.12968/bjon.2019.28.15.S26
3. de Laat EH, van den Boogaard MH, Spauwen PH, van Kuppevelt DH, van Goor H, Schoonhoven L. Faster wound healing with topical negative pressure therapy in difficult-to-heal wounds: a prospective randomized controlled trial. Ann Plast Surg. 2011;67(6):626–631. doi:10.1097/SAP.0b013e31820b3ac1
4. Blume PA, Walters J, Payne W, Ayala J, Lantis J. Comparison of negative pressure wound therapy using vacuum-assisted closure with advanced moist wound therapy in the treatment of diabetic foot ulcers: a multicenter randomized controlled trial. Diabetes Care. 2008;31(4):631–636. doi:10.2337/dc07-2196
5. Fernández LG, Matthews MR, Benton C, et al. Use of a novel silicone-acrylic drape with negative pressure wound therapy in anatomically challenging wounds. Int Wound J. 2020;17(6):1829–1834. doi:10.1111/iwj.13471
Sign Up Today





{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
