

Ilioinguinal Flap Combined With Tensor Fascia Lata Muscle Flap to Repair Deep Electrical Burns in the Lower Abdomen: A Report of Two Cases
This article describes 2 patients with deep electrical burns in the lower abdomen that showed extensive skin and soft tissue damage, partial necrosis of abdominal muscle tissue, and weak abdominal wall.
Abstract
Introduction. Electrical burns are caused by the conversion of electrical energy flowing through the body into heat energy, which can cause coagulative necrosis of the skin and deep tissues. Deep tissue damage is often more serious than skin damage. Electrical burns have the characteristics of destructive and progressive damage and present the common symptoms of severe local tissue damage accompanied by a wide range of deep tissue necrosis, resulting in injury of nerves, blood vessels, bones, and internal organs. Autologous skin grafting alone cannot effectively cover deep tissues or repair electrical burn wounds. Case Report. This article describes 2 patients with deep electrical burns in the lower abdomen that showed extensive skin and soft tissue damage, partial necrosis of abdominal muscle tissue, and weak abdominal wall. As a single tissue flap was too small to effectively cover the defect wound, ilioinguinal flap and tensor fascia lata muscle flap were utilized in both cases with good outcomes. These flaps survived completely, and the wounds were effectively repaired. After repair, the shape was satisfactory, and the function of the lower abdomen was normal. Conclusions. Transfer of flaps from a site near the wound for repairing electrical burns is convenient for transfer with minimal surgical trauma and a simpler operating procedure than the free flap.
Introduction
Electrical burns, caused by electric shock, differ from thermal and chemical burns with persistent injuries, extensive trauma, complications, and long-term morbidity specific to these burns.1 According to Joule law, the heat generated by the conductor after energization is proportional to the square of the current through the body and the resistance of the body, proportional to the contact time.2 The incidence of electrical burns is increasing each year. Beijing Jishuitan Hospital has recorded 25 years of hospitalization of burn patients, of which electrical burns account for 8%.3 In an epidemiological study of burn patients in a teaching hospital of Nepal Medical School, electrical burns comprised 14% of burn patients.4
Electrical burns are characterized by destructive, progressive damage. Generally, electrical burns have severe local tissue damage accompanied by extensive deep tissue necrosis and can affect nerves, blood vessels, bones, and internal organs.5 Autologous skin grafting alone cannot effectively cover deep tissues or repair wounds of electrical burns. In order to reduce the secondary damage and complications caused by electrical burns in the deep tissues and effectively repair these wounds, the authors considered the early treatment of electrical burns and wound repair. Appropriate flaps, such as myocutaneous flaps and other tissue flaps, can effectively repair deep electrical burn wounds and protect the deep tissues and organs against these burns.6 This article reports 2 cases of deep electrical burns in the lower abdomen that were successfully repaired by ilioinguinal flap combined with the tensor fascia lata muscle flap.
Case Report
Case 1
An 11-year old boy fell into a transformer while playing and was burned by high-voltage electricity of 10 000 volts. One hour following injury, he was taken to the authors’ burn department (First Affiliated Hospital of Anhui Medical University [Anhui, China]); he was treated solely by their department. Hospital admission was diagnosed as multiple electrical injuries 25% II.
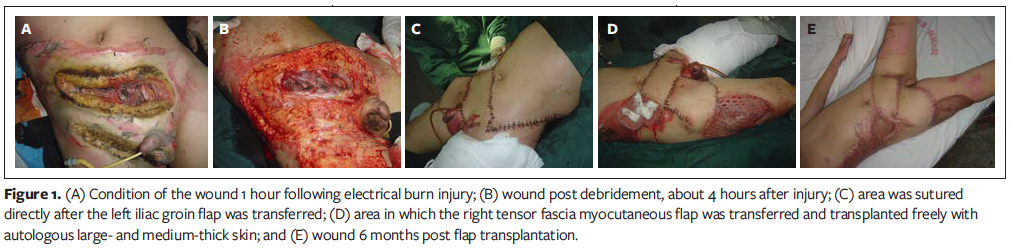
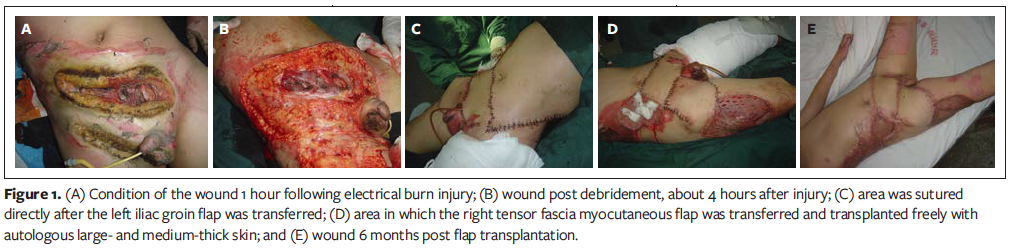
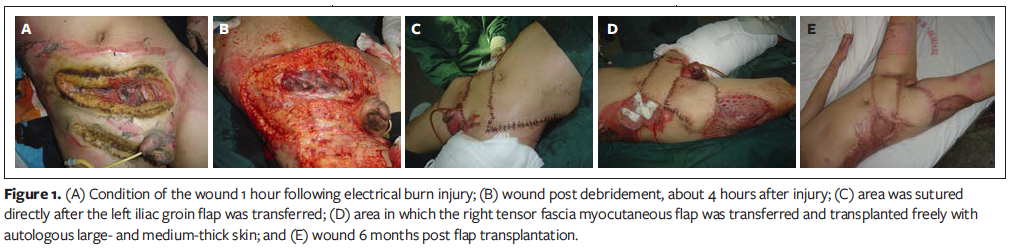
Physical examination showed electrical burn wounds distributed in many parts of the body. In addition, large parts of the skin and soft tissue were defected in the lower abdomen, and the exposed area was partially charred. Injuries to the body included an exposed and partially necrotic abdominal rectus and its anterior sheath, exposed bladder, scorched skin of the right scrotum, and exposed and necrotic right testicle (Figure 1A).
Various related emergency examinations showed organ function was normal, and the internal environment and vital signs were stable. The patient underwent emergency surgical treatment of the lower abdominal burn wound 4 hours following injury. Preoperative wound evaluation showed the size of large area of skin and soft tissue defects in the lower abdomen was up to 24 cm x 18 cm; the left and right rectus abdominis muscles from 2 cm below the umbilicus to the pubic symphysis were necrotic; the sheath of the rectus abdominis mostly was absent, but the parietal peritoneum was intact; the right inguinal ligament was exposed; and there was a 3-cm longitudinal laceration in the anterior bladder wall and urine spillage (Figure 1B).
The bladder fistula was placed at the anterior wall of the bladder, and the laceration was sutured directly. After bladder spasm and suturing the residual rectus sheath, the authors designed the left ilioinguinal flap combined with the right tensor fascia lata muscle flap to repair the lower abdominal wound. The flap was designed according to the shape of the defect. The left ilioinguinal flap was created with a circumflex suprasuperficial artery as the axial vessel (flap size: 16 cm x 9 cm). The flap was lifted under the deep fascia following in turn cutting the skin, subcutaneous tissue, and deep fascia. In addition, the right tensor fascia lata muscle flap was designed with the lateral circumflex femoral artery as the axial artery (flap size: 20 cm x 9 cm). This flap was lifted under the tensor fasciae muscle after the skin, subcutaneous tissue, and iliac crest at the distal end were in turn cut. The in situ wound bleeding during flap removal was stopped immediately using a electronic surgical generator coagulating and ligated in the operation. The ilioinguinal flap and tensor fascia lata muscle flap were combined to repair the lower abdominal wound. After the left inguinal flap was transferred, the area was sutured directly. The area in which the right tensor fascia myocutaneous flap was transferred then was transplanted freely with autologous large- and medium-thick skin (Figure 1C, 1D).
The metastatic tissue flaps survived completely, and the lower abdominal wound was repaired effectively. The patient had no complications and was discharged after 81 days of hospitalization. After the wound healed, according to the routine treatment of functional rehabilitation in China, the patient received external application of compound heparin sodium and allantoin 3 times daily and wore pressure pants to prevent scar hyperplasia. At 6-month postoperative follow-up, the local shape was satisfactory, and function was normal (Figure 1E).
Case 2
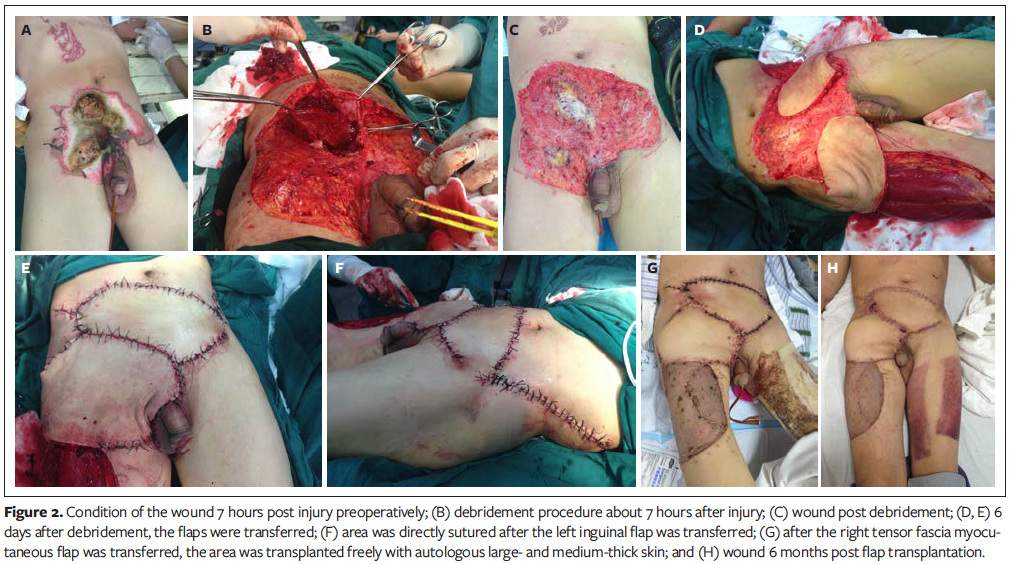
A 52-year-old man accidentally was hit by a 10 000-volt high-voltage electric shock in various parts of the body when he was operating a circuit at about 8:00AM on June 21, 2016. The patient immediately was sent to the authors’ department after injury. During the course of the disease, he was conscious and thirsty without nausea and vomiting and had less urine output (~50 mL) and soy sauce urine. In order to prevent myoglobinuria from clogging the renal tubules and damaging renal function, 5% sodium bicarbonate was instilled intravenously to alkalinize urine and furosemide was injected intravenously for diuretic treatment. The wounds were mainly located in the left shoulder, left upper limb, and lower abdomen. The wounds were all eschar-like changes with many irregular skin defects in the lower abdomen (Figure 2A).
The patient underwent emergency debridement of the lower abdomen with electrical burns 7 hours post injury. Preoperative wound evaluation showed the rectus sheath and rectus abdominis muscle had been degenerated and necrotic. In addition, the injury reached the peritoneum (Figure 2B). After the lower abdomen was debrided, a wound with an irregular size, measuring 30 cm x 20 cm, was drawn by vacuum sealing drainage (VSD) under negative pressure (Figure 2B, 2C).
After the wound was debrided and VSD negative pressure was applied for 6 days at continuous pressure of 0.03 kpa, the left abdominal sacral ilioinguinal flap and the right tensor fascia lata muscle flap were used to repair the lower abdominal defect. The flaps were designed based on the shape of the defect. The left ilioinguinal flap was harvested with a circumflex suprasuperficial artery as the axial blood vessel (flap size: 18 cm x 10 cm). This flap was lifted under the deep fascia after in turn cutting the skin, subcutaneous tissue, and deep fascia. The right tensor fascia lata muscle flap also was created with the lateral circumflex femoral artery as the axial vessel, with the size of the myocutaneous flap at 22 cm x 10 cm. This flap was lifted under the tensor fasciae muscle after the skin, subcutaneous tissue, and iliac crest at the distal end were in turn cut. The in situ wound bleeding during flap removal was stopped immediately using electronic surgical generator coagulating and ligated in the operation. The ilioinguinal flap and tensor fascia lata muscle flap were combined to repair the wound of the lower abdominal defect (Figure 2D, 2E). After the left inguinal flap was transferred, the area was sutured directly. The area in which the right tensor fascia myocutaneous flap was transferred then was transplanted freely with autologous large- and medium-thick skin (Figure 2F, 2G).
The metastatic tissue flaps survived completely, and the lower abdominal wound effectively was repaired. The patient had no complications and was discharged after 55 days of hospitalization. After the wound healed, as per routine treatment of functional rehabilitation in China, the patient received external application of compound heparin sodium and allantoin 3 times daily and wore pressure pants to prevent scar hyperplasia. At 6-month postoperative follow-up, the local shape was satisfactory, and function was normal (Figure 2H).
Discussion
Herein, 2 cases of deep electrical burns in the lower abdomen caused severe damage in large areas of skin and soft tissue defects, partial necrosis of abdominal muscle tissue, and a weakened abdominal wall. After early debridement, the authors used the ilioinguinal flap combined with the tensor fascia lata muscle flap to repair the wound. The flaps completely survived, and the wound was repaired. A very satisfactory outcome was achieved, and the lower abdomen functioned normally after repair.
Timing of surgery
The timing of surgical treatment for deep electrical burn wounds is very important for wound healing, and the length of time between injury and surgery is closely related to the therapeutic outcome. In a previous study,7 medical experts found there were a series of changes in the burn site in a short period of time following the electrical burn. From the moment of injury to the first 24 hours after injury, the area of necrosis of the electrical burn continued to expand, but began to slow down after 48 hours, and it lasted for several days.7 Histological observation showed normal tissue, degeneration tissue, and necrotic tissue were intertwined in the electrical burn area. Over time, normal tissues gradually transformed into degenerative tissues; the degenerative tissues gradually evolved into necrotic tissues, which led to further expansion of tissue necrosis.8 The first 8 hours post injury is suggested to be the best time for treatment.7 Performing surgery early after an electrical burn injury has been shown to contribute to better the wound healing effects.9 Timely, early debridement and surgical wound repair can prevent the expansion of the necrotic area and save the function of the limb.10
Selection of surgical methods
In the past, conservative treatment was used mainly for electrical burn treatment, such as dressing change, dislocations, waiting for the clear demarcation between necrotic tissue and normal tissue, and skin grafting after the formation of wound granulation tissue. However, these conservative treatment methods have shown a long disease duration, poor wound healing, and are likely to negatively impact the function of the anatomical location involved at the burn site.11 Consequently, both patients and doctors are not satisfied with the therapeutic effect.
Presently, some researchers6 advocate early, thorough surgical debridement and effective tissue flap coverage for the treatment of deep electrical burns. Inconsistent with their6 opinions, early, thorough surgical debridement and flap coverage for the 2 cases of deep, inferior electrical burn wounds presented herein achieved significant clinical outcomes.
There are differing thoughts regarding the degree of necrotic tissue debridement. Huang12 advocates thorough debridement to treat electrical burns and proposes that incomplete debridement impacts flap survival. In contrast, Tiengo et al13 advocate appropriate debridement of the wound, flap coverage, and continuous irrigation under the flap. Analyzed and compared the views of the scholars, combined with the therapeutic outcome of 2 cases in this article, the present authors believe electrical burn wounds need to be debrided early, necrotic tissue should be removed, and interorganisms should be effectively protected during debridement. The exposed nerve, blood vessel, tendon, bone, and internal organs involved in the burn wound must be covered with blood flaps, myocutaneous flaps, and/or other tissue flaps.
Principle of selecting tissue flaps
As per the treatment outcomes of flaps used on the present 2 deep electrical burn wounds in the lower abdomen, the selection of tissue flaps should follow the principles of simplicity, then complexity, and first adjacent furthest point of the burn wound.14 Each kind of tissue flap has its advantages and disadvantages.15 For instance, random skin flaps are simple to cut but the length-width ratio needs to be taken into account to avoid excessive tension caused by distal necrosis. The axial flap has good blood supply, so the distal end is less prone to a blood flow disorder, and the anti-infective performance is enhanced. Myocutaneous flaps can be used to fill large tissue defects and have the strongest anti-infective properties, but they inflict a lot of damage to the valve area. Therefore, when selecting the tissue flap, the specific conditions of the wound surface after debridement, the surrounding conditions, and the characteristics of various tissue flaps should be taken into account. In addition, the shape and function of the electrical burn site should be restored as much as possible. In these 2 cases, if only 1 tissue flap is used, the area of the tissue flap is too small to effectively cover the defect wound; as a result, the authors used 2 flaps to repair the wound.
Conclusions
The 2 reported cases of deep electrical burns in the lower abdomen showed extensive skin and soft tissue damage, partial necrosis of abdominal muscle tissue, and a weakened abdominal wall. Considering a single tissue flap was too small to effectively cover the wound, ilioinguinal flap combined with tensor fascia lata muscle flap were used to repair the wound after early debridement; consequently, the flap completely survived. This treatment method achieved very satisfactory outcomes in the appearance of the lower abdomen following the repaired burned area and normal function of the lower abdomen restored. Harvesting skin flaps close to the wound is convenient for transfer and easier for the operation compared with the free flap as well as a less invasive surgical procedure. The present clinical outcome provided an available surgical method for the clinical treatment of deep electrical burn wounds in the lower abdomen. Therefore, deep electrical burn wounds must be repaired with appropriate flaps (eg, myocutaneous flaps) to protect deep tissues and adjacent organs.
Acknowledgments
Authors: Delin Hu, MM; Chengying Meng, BS Med; Jiayan Hu, BS Nurs; Yan Zhou, BS Nurs; Shiping Lu, BS Nurs; Youxin Yu, MM; Linsen Fang, MM; and Yexiang Sun, PhD
Affiliation: Department of Burn, The First Affiliated Hospital of Anhui Medical University, Hefei, Anhui, China
Correspondence: Delin Hu, MM, Department of Burn, The First Affiliated Hospital of Anhui Medical University, No. 218 Jixi Road, Hefei, Anhui 230022 China; hdl0522@163.com
Disclosure: The authors disclose no financial or other conflicts of interest.
References
1. Lunawat A, Datey SM, Vishwani A, Vashistha R, Singh V, Maheshwari T. Evaluation of quantum of disability as sequelae of electric burn injuries [published online March 1, 2015]. J Clin Diagn Res. 2015;9(3):PC01–PC04. 2. Kearns RD, Rich PB, Cairns CB, Holmes JH, Cairns BA. Electrical injury and burn care: a review of best practices. EMS World. 2014;43(9):34–41. 3. Zheng ZZ, Xie WG. Emergency treatment of contact electrical burns. Chinese J Anatomy Clinics. 2001;6(2):123–124. 4. Chalise PR, Shrestha S, Sherpa K, Nepal U, Bhattachan CL, Bhattacharya SK. Epidemiological and bacteriological profile of burn patients at Nepal Medical College Teaching Hospital. Nepal Med Coll J. 2008;10(4):233–237. 5. Maghsoudi H, Adyani Y, Ahmadian N. Electrical and lightning injuries. J Burn Care Res. 2007;28(2):255–261. 6. Jeyakumar P, Hussain AT, Ahamed AR. Reconstruction of extensive post-electric burn scalp defects with exposed bones: a study of 12 cases. Ann Plast Surg. 2018;81(1):39–44. 7. Zhu Zhi-xiang,Li Hui-qin,Liu Xue-yuan,et al. Experimental electrical injury: histology and ultrastructure. [Article in Chinese.] Zhonghua Zheng Xing Shao Shang Wai Ke Za Zhi.1991;7(3):122–125. 8. Cheema SA. Pattern and profile of electric burn injury cases at a burn centre. J Ayub Med Coll Abbottabad. 2016;28(4):702–705. 9. Garcia LP, Huang A, Corlew DS, et al. Factors affecting burn contracture outcome in developing countries: a review of 2506 patients. Ann Plast Surg. 2016;77(3):290–296. 10. Zhu ZX, Zhang YT, Liu XY, Wang TJ, Wang Y. Urgent repair of electrical injuries: analysis of 40 cases. Acta Chir Plast. 1990;32(3):142–151. 11. Sun YH. Achievements and challenge of treatment of electric burn over the past 50 years in China. [Article in Chinese.] Zhonghua Shao Shang Za Zhi. 2008;24(5):381–383. 12. Huang XY. Augmentation of quality of wound healing of deep burn. Zhonghua Shao Shang Za Zhi. 2009;25(1):3–5. 13. Tiengo C, Castagnetti M, Garolla A, Rigamonti W, Foresta C, Azzena B. High-voltage electrical burn of the genitalia, perineum, and upper extremities: the importance of a multidisciplinary approach. J Burn Care Res. 2011;32(6):e168–e171. 14. Demir Z, Velidedeoğlu H, Çelebioğlu S. V-Y-S plasty for scalp defects. Plast Reconstr Surg. 2003;112(4):1054–1058. 15. Lu K, Han Y, Guo S. Application and development of free composite tissue flap in plastic surgery. [Article in Chinese.] Zhongguo Xiu Fu Chong Jian Wai Ke Za Zhi. 2007;21(9):940–944.
Sign Up Today





{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
