




Trends in Pressure Injury Development in Patients With Lower Motor Neuron and Upper Motor Neuron Lesions: A Retrospective Descriptive Study
ABSTRACT
BACKGROUND: Persons with spinal cord injury (SCI) are at high risk of pressure injury (PrI) development, but there is limited information about the effect of injury patterns (ie, upper motor neuron [UMN] or lower motor neuron [LMN] presentations) on PrI risk. PURPOSE: This study was conducted to explore the rate of PrI development in patients with LMN and UMN lesions. METHODS: A retrospective descriptive review of data from patients who were treated at a specialized outpatient SCI rehabilitation center in Baltimore, MD, between January 1, 2013, and December 31, 2019. Patients with neurological levels T8 and below, any type of SCI motor ability, and whose records were complete were included in the study. Data extracted included age, sex, date of injury, injury type, modified Ashworth Scale (MAS) score (ie, scale representing resistance to passive movement), date MAS was performed, body mass index, Spinal Cord Independent Measures-III, Braden Scale scores, ambulatory status, antispasticity medication, presence or history of PrI, and method of closure. Patients with a score of 0 on the MAS and without pharmacological management for spasticity were included in the LMN group, and patients with a score greater than 0 on the MAS with or without pharmacological management were included in the UMN group. Variables were compared using mean ± standard deviations, range, t-test, and Pearson’s chi-squared and Fisher exact tests where appropriate. P values < .05 were considered statistically significant. RESULTS: Of the 602 records examined, 194 were complete and met inclusion criteria. Most patients (119, 61.34%) were male and classified in the UMN group (162, 84%). Mean age and time since injury were 35.20 ± 18.78 and 6.20 ± 7.62 years, respectively. Seventy-three (73) of 194 patients (37.6%) had, or had a history of, a PrI; 21 (66%) in the LMN and 52 (32%) in the UMN group (X21 = 12.8; P < .001). Statistically significant differences were noted between persons with LMN and UMN in terms of Braden Scale scores, age, body mass index, Spinal Cord Independent Measures-III, and time since injury. Compared with the UMN group, more patients in the LMN group had motor complete injuries with ISNCSCI levels A/B (P < .001) and were nonambulatory (P < .001). CONCLUSION: The results of this study confirm that patients with SCI have a high rate of PrI development. The percentage of PrIs was significantly higher in the LMN than in the UMN group. Additional studies to examine the other variables that were significantly different between groups and their effect on PrI risk are needed.
INTRODUCTION
According to National Spinal Cord Injury Statistical Center 2020 data, approximately 17 810 new cases of spinal cord injury (SCI) occur each year and approximately 294 000 people currently live with SCI in the United States.1 A 2019 systematic review and meta-analysis2 of 82 722 patients indicated that more than 1 in 5 individuals with SCI will have a pressure injury (PrI) develop. The National Pressure Injury Advisory Panel3 (NPIAP) defines PrI as localized damage to the skin and underlying soft tissues, resulting from intense and/or prolonged pressure or pressure in combination with shear, over a bony prominence or related to medical and other devices. An observational, cross-sectional study4 of the seated anatomy and deformation of 6 participants (4 of whom were diagnosed with SCI and 2 of whom were in the control group) indicated that persons with SCI (compared with persons without SCI) have reduced mean muscle volume, ranging from 43.5% to 98%, beneath their ischial tuberosities while sitting. These structural changes increase the risk of tissue deformation and ischemic-related tissue damage and place patients with SCI at greater risk of PrI development.4 Although data4-7 show that patients with SCI are at increased risk of PrI development due to neurological, physical, and structural changes, research to determine if SCI injury patterns affect the risk of PrI development is limited.
SCI is categorized according to 2 factors. The first factor is the extent of the injury, classified according to the 1) last intact nerve root above the injured portion of the spinal cord and 2) severity of the lesion. The second factor is the injury pattern—upper motor neuron (UMN) and lower motor neuron (LMN) lesions. UMN injury occurs in the descending motor tract before the anterior horn of the spinal cord.8 Patients with UMN syndrome clinically present with hyperreflexia, spasticity, and a positive Babinski reflex.8 LMN injury occurs in the anterior horn cells or the peripheral motor pathways; persons with LMN syndrome present with hyporeflexia, flaccid paralysis, and atrophy.8
The purpose of this retrospective, descriptive study was to explore further the rate of PrI development in patients with UMN and LMN lesions. The authors hypothesized that patients with LMN lesions were more susceptible to developing PrIs compared with patients with UMN lesions, due to more severe muscle atrophy in patients with LMN lesions.
METHODS
This single-site, descriptive, retrospective study was conducted in the specialized outpatient SCI rehabilitation unit of Kennedy Krieger Institute, Baltimore, MD, between January 1, 2013, and December 31, 2019. Data from outpatient visits were extracted from the institute’s Research Electronic Data Capture (REDCap) (version 10.6.5, Vanderbilt University) by the study coordinator. Inclusion criteria stipulated that participants should be patients with neurological levels of injury, T8 and below, motor complete or motor incomplete SCI as defined by the International Standards for Neurological Classification of Spinal Cord Injury (ISNCSCI), and whose records were complete. The following variables related to PrI development or descriptive of the sample were retrieved: date of birth, sex, date of injury, injury type, Braden Scale scores, body mass index (BMI), Spinal Cord Independent Measures-III (SCIM-III), ISNCSCI, and modified Ashworth Scale [MAS] score as well as the date MAS was performed by a physician. The MAS is a spasticity scale that rates the amount of resistance felt when moving a limb passively through its full range of motion.9 The ISNCSCI examination and classification was developed by the American Spinal Injury Association to classify SCI based on motor and sensory completeness of injury based on the following: motor and sensory levels (right and left), a single neurological level of injury (NLI), the completeness of SCI, zone of partial preservation, and the severity of SCI using the ASIA Impairment Scale (AIS).10 Classifications A/B are considered motor complete, C/D are considered motor incomplete, and E is normal.10 Neurological level of injury (NLI) is determined by identifying the most caudal segment of the spinal cord with both intact sensation and normal antigravity muscle function strength.10 The SCIM-III is a self-report assessment containing 19 items on self-care, respiration and sphincter management, and mobility; the higher the score, the more independent the patient, with a total score of 100 representing complete independence.11
Information on other factors thought to be related to PrI development were manually retrieved by the study team and included ambulatory status and antispasticity medication. In addition, physical therapy notes were reviewed for presence of PrI, history of PrI, and method of closure (when applicable). To avoid collecting outdated data, charts were reviewed for physical therapy initial evaluation within 6 months of the date of the MAS performed by a physician. If no evaluation was found within 6 months, the chart was considered incomplete and was not used.
Data analysis. All data were extracted from REDCap and entered into an Excel (Microsoft Corp.) database and stored in a limited access folder on the Institute’s secured server. This database was used by the study team when manually retrieving data from individual patient charts. Once the retrieval process was completed, the data were de-identified to preserve the confidentiality of patients. These data then were sent to the statistician on the study team for statistical analysis.
The study team categorized antispasticity medication and ambulatory status into yes/no categories. Method of closure was grouped into “need for surgical closure” versus “no need for surgical closure.” Braden score, SCIM-III, BMI, continuous features (age [calculated from date of birth and date of MAS performed by a physician] and time since injury [calculated from the date of injury and date of MAS performed by a physician]) were summarized with means, standard deviations, ranges, and t-test P values. This analysis was performed in Excel. Categorical features (sex, NLI, and ISNCSCI) were summarized using frequency counts and percentages.
Team members used modified Ashworth scores and antispasticity medication data to categorize charts into UMN and LMN groups. The LMN group was classified as having a score of 0 on the MAS and without pharmacological management. The UMN group was classified as having any number greater than 0 on the MAS and with or without pharmacological management. Although a single patient might have had several follow-up visits between 2013 and 2019, variables were recorded only once to prevent duplication of data. The PrI-related outcome categories were “wound never” (defined as the patient reporting no presence of an active PrI at the time of physical therapy initial evaluation and no history of PrI) and “wound ever” (defined as the patient reporting an active PrI at the time of physical therapy initial evaluation or a history of PrI).
Comparisons of factors between UMN and LMN stratifications comprised PrI categories (wound never and wound ever), method of PrI closure (need for surgical closure vs no need for surgical closure), ambulatory status (yes or no), ISNCSCI (A/B vs C/D/E), sex, and NLI (T8-T12 vs L1-below) were evaluated using Pearson’s chi-squared test. This analysis was performed using SPSS version 27 (IBM) and included descriptive statistics for all dependent variables. A Pearson’s chi-squared analysis was used to determine the association between the UMN and LMN stratifications and categories thought to be related to PrI development. The assumption that independent and dependent variables were linearly associated was checked and met using Pearson’s chi-squared and Fisher exact tests. P values <.05 were considered statistically significant.
Ethical considerations. The analysis of electronic health records was approved by the Institutional Review Board of the Johns Hopkins School of Medicine through the retrospective study protocol.
RESULTS
Between January 1, 2013, and December 31, 2019, 602 patient charts were retrieved; 210 were excluded because they did not meet the diagnosis inclusion criteria. Examples of excluded diagnoses included but were not limited to congenital or progressive diseases or secondary brain involvement. An additional 198 charts were excluded because a physical therapy evaluation had not been completed within 6 months of when MAS was performed by the physician. After the exclusions, 194 charts remained and were used for analysis.
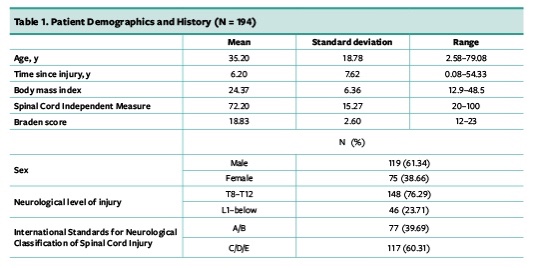
Patient data. The mean age of the 194 patients was 35.20 ± 18.78 (range, 2.58–79.08) years, with time since injury of 6.20 ± 7.62 (range, 0.08–54.33) years. In the total sample, 119 (61.3%) were male, 117 (60.3%) were motor incomplete SCI, and 148 (76.3%) had higher neurological levels of injury (T8–T12). Mean BMI was 24.37 ± 6.36 (range, 12.9–48.5) kg/m2, mean SCIM-III score was 72.20 ± 15.27 (range, 20–100), and mean Braden score was 18.83 ± 2.60 (range, 12–23) (Table 1).
{kind=link}
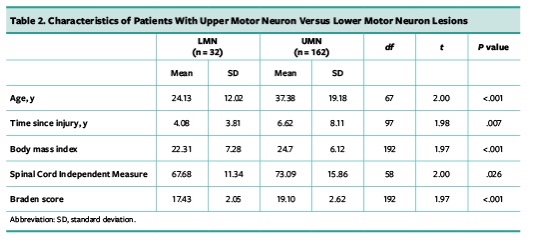
Upper versus lower motor data. Thirty-two (32) patients were classified in the LMN group and 162 patients were classified in the UMN group. Patient with LMN were younger (24.13 ± 12.02 vs 37.38 ± 19.18: t67 = 2.00; P < .001) with more recent injuries (4.08 ± 3.81 vs 6.62 ± 8.11: t97 = 1.98; P = .007) compared with patients with UMN. Patients with LMN had lower Braden scores (17.43 ± 2.05 vs 19.10 ± 2.62: t192 = 1.97; P < .001), lower BMI (22.31 ± 7.28 vs 24.7 ± 6.12: t192 = 1.97; P = .05), and decreased independence as self-reported on the SCIM-III (67.68 ± 11.34 vs 73.09 ± 15.86: t58 = 2.00; P = .03) than patients with UMN (Table 2). Seventy-three (73) of 194 patients (37.6%) had, or had a history of, a PrI.
{kind=link}
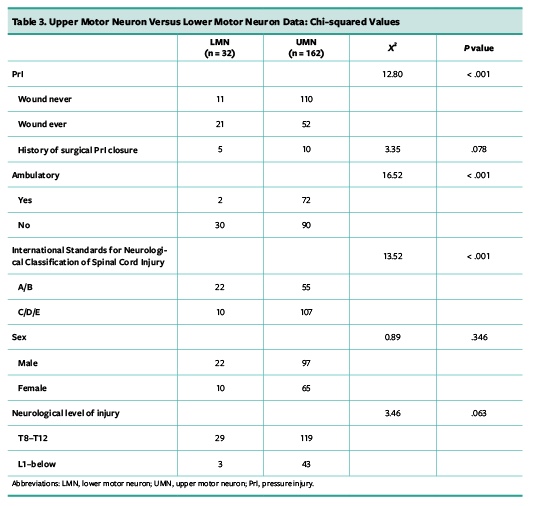
The proportion of patients who had or reported a history of PrI was higher in the LMN group (21, 66%) than in the UMN group (52, 32%) (X21 = 12.8; P < .001). More patients in the LMN group were motor complete (X21 = 13.5; P <.001) and were nonambulatory (X21 = 16.5; P <.001). Within the LMN group, 2 (6%) were considered ambulatory compared with 72 (44%) in the UMN group. Variables that did not significantly differ between UMN and LMN groups included need for surgical closure (X21 = 3.4; P = .08), sex (X21 = 0.9; P = .35), and neurological level of injury (X21 = 3.5; P = .06) (Table 3).
{kind=link}
DISCUSSION
Numerous studies have established that patients with SCI are at risk of developing PrI.2,6,7 The aim of this retrospective study was to determine if SCI lesion characteristics, specifically UMN and LMN syndromes, play a role in the risk of PrI development.
In concordance with the National Spinal Cord Injury Statistical Center,1 the current study had more males (61.3%) and incomplete SCI (60.3%). Although the literature comparing SCI-specific PrIs risk factors with lesion characteristics (UMN vs LMN) is sparse, high-level evidence has identified PrI risk factors in the general SCI population. In this study, 73 of 194 patients (37.6%) had, or had a history of, a PrI. Furthermore, the proportion of patients in the LMN group who were nonambulatory was significantly higher (30, 93%) than in the UMN group (90, 55%). A systematic review noted that significant risk factors for PrI development in persons with SCI include motor completeness of lesion (A/B), high neurological level of injury (tetraplegia), low functional independence measure level of self-care and lower motor independence, presence of comorbidity, previous PrI surgery, self-report of PrI, poor pulmonary function (pulmonary disease/pneumonia), and decreased mobility at time of discharge.6
A 2020 meta-analysis and systematic review7 of 600 078 participants examined multiple risk factors and the complexity of PrI development in the SCI population. Risk factors for PrI in patients with SCI were found to include duration after SCI of > 1 year, increasing age, male sex, poor nutritional status, quadriplegia, smoking, presence of a comorbidity, Braden scores indicating that the patient was at high risk, being underweight, lower level of education, and lack of an intimate partner.7 In the current study, mean time since injury was 6.20 ± 7.62 years and 61.3% were male, which suggests that many patients in this study were at high risk of PrI. Additionally, Braden scores and BMI were significantly lower in the UMN group (P < 0.05), placing patients in the LMN group at greater risk of PrI. However, in the current study, patients in the UMN group were older and had lived with their injuries for longer.
Of the 73 patients in the current study who had a current PrI or history of PrI, 52 (47%) were in the UMN and 21 (65%) were in the LMN group. A 2-year cross-sectional and then longitudinal prospective study5 conducted among 25 persons with LMN lesions showed that within months, muscle fibers were replaced by adipose and fibrous tissues. These severe functional and structural changes were not present in patients with UMN lesions, even 20 years after thoracic level SCI.
Clinicians can play an essential role in reducing the risk of PrI development in the LMN population by prescribing individualized seating surfaces. Due to increased adipose tissue and decreased muscle tissue volumes under their ischial tuberosity,4,5 use of air cushions might not adequately reduce pressure over bony prominences in patients with LMN. One study found great variability in cushion effectiveness among 6 participants and 6 cushion varieties4; therefore, it is imperative to refer all patients, especially persons with LMN, to a seating clinic for comprehensive assessment and an individualized wheelchair cushion prescription.
The results of this study confirm that persons with SCI have a high rate of PrI development and suggest that the risk is highest among persons with LMN lesions. Because an estimated 1 in 3 patients with SCI have PrIs worldwide,7 further prospective observational studies are warranted to examine the effect of upper and lower motor neuron lesion characteristics, such as muscle atrophy and spasticity, on PrI development. Hypertonia or hypotonia could be an SCI-specific risk factor of PrI development; these conditions have a direct impact on a patient’s independence concerning activities of daily living, ability to transfer between bed and chair, and mobility. A better PrI risk assessment tool for patients with SCI may facilitate the implementation of optimal prevention strategies and decrease the prevalence of PrI in these patients.
LIMITATIONS
The limitations of this study include its retrospective design and small sample size. A further limitation is the stratification method used for the UMN and LMN groups. Previously identified clinical factors, such as deep tendon reflex and Babinski sign, were not available for all patients. Furthermore, data on other SCI-specific PrI risk factors identified in systematic reviews, such as nutritional status,7 quadriplegia,7 smoking,7 level of education,7 and pulmonary status,6 were not evaluated in this study.
CONCLUSION
A descriptive retrospective study was conducted to evaluate the rate of PrI development in SCI patients with UMN and LMN lesions. The proportion of patients who had, or reported a history of, PrI was significantly higher in patients with LMN than in patients with UMN lesions (93% vs 55%; P < 0.001). Furthermore, patients in the LMN group were more likely than patients in the UMN group to have the following SCI-specific PrI risk: lower Braden scores, lower SCIM III scores, lower BMI, and motor completeness of injury. Patients with SCI and LMN have greater reduction in muscle tissue volume,4,5 which increases their risk of tissue deformation and ischemic-related tissue damage compared with their counterparts with UMN lesions. Although studies with stronger level of evidence are warranted, the results of this study confirm that clinicians should provide individualized care to decrease the risk of PrIs when working with patients with SCI, specifically those with LMN presentation.
AFFILIATIONS
Dr. Catania is a physical therapist, Ms. Morgan is a physical therapy assistant, and Dr. Martin is a manager of clinical education and training, Kennedy Krieger Institute, International Center for Spinal Cord Injury, Baltimore, MD. Dr. Martin is also a faculty member, Johns Hopkins School of Medicine, Department of Physical Medicine and Rehabilitation, Baltimore, MD. Address all correspondence to: Quyen Nguyen Catania, PT, DPT, CWS, CLT, Kennedy Krieger Institute, International Center for Spinal Cord Injury, Baltimore, MD; email: cataniaq@kennedykrieger.org.
References
1. National Spinal Cord Injury Statistical Center. 2020 Annual Statistical Report. Birmingham, AL: National Spinal Cord Injury Statistical Center. Accessed August 21, 2020. https://www.nscisc.uab.edu/Public/Facts%20and%20Figures%20-%202021.pdf.
2. Hong-Lin C, Ji-Yu C, Lin D, et al. Incidence of pressure injury in individuals with spinal cord injury: a systematic review and meta-analysis. J Wound Ostomy Continence Nurs. 2020; 47(3):215–223. doi:10.1097/WON.0000000000000633
3. Edsberg LE, Black JM, Goldberg M, McNichol L, Moore L, Sieggreen M. Revised National Pressure Ulcer Advisory Panel Pressure Injury Staging System: revised Pressure injury staging system. J Wound Ostomy Continence Nurs. 2016;43(6):585–597. doi:10.1097/WON.0000000000000281
4. Brienza D, Vallely J, Karg P, Akins J, Gefen A. An MRI investigation of the effects of user anatomy and wheelchair cushion type on tissue deformation. J Tissue Viability. 2017;27(1):42–53. doi:10.1016/j.jtv.2017.04.001
5. Kern H, Stramare R, Martino L, Zanato R, Gargiulo P, Carraro U. Permanent LMN denervation of human skeletal muscle and recovery by h-b FES: management and monitoring. Eur J Transl Myol. 2010;1(3):91–104.
6. Marin J, Nixon J, Gorecki C. A systematic review of risk factors for the development and reoccurrence of pressure injuries in people with spinal cord injuries. Spinal Cord. 2013;51(7):522–527. doi:10.1038/sc.2013.29
7. Hiferaw WS, Akalu TY, Mulugeta H, et al. The global burden of pressure ulcers among patients with spinal cord injury: a systematic review and meta-analysis. BMC Musculoskelet Disord. 2020;21(1):334. doi:10.1186/s12891-020-03369-0
8. Zayia LC, Tadi P. Motor neuron. In: StatPearls. Neuroanatomy. Treasure Island, FL: StatPearls Publishing; 2020: Accessed February 1, 2021. https://www.ncbi.nlm.nih.gov/books/NBK554616/.
9. Haas B, Bergström E, Jamous A, Bennie A. The inter rater reliability of the original and of the modified Ashworth scale for the assessment of spasticity in patients with spinal cord injury. Spinal Cord. 1996;34(9):560–564. doi:10.1038/sc.1996.100
10. Walden K, Bélanger LM, Biering-Sørensen F, et al. Development and validation of a computerized algorithm for International Standards for Neurological Classification of Spinal Cord Injury (ISNCSCI). Spinal Cord. 2016;54(3):197–203. doi:10.1038/sc.2015.137
11. Fekete C, Eriks-Hoogland I, Baumberger M, et al. Development and validation of a self-report version of the Spinal Cord Independence Measure (SCIM III). Spinal Cord. 2013;51(1):40–47. doi:10.1038/sc.2012.87
