



Understanding Recent Regulatory Guidelines for Hospital-Acquired Catheter-Related Urinary Tract Infections and Pressure Ulcers
The Centers for Medicare and Medicaid Services issued a final rule to update the hospital inpatient prospective payment system for fiscal year 2008. Included in this new ruling is the need to identify conditions present on admission as well as guidelines underscoring that payment will not be rendered for certain conditions determined to be hospital-acquired. Two of the eight conditions affect patients with incontinence: catheter-associated urinary tract infections and pressure ulcers. These conditions, if present on admission to an acute care facility, must be identified by the clinical staff and the attending physician. For patients admitted without these conditions, evidence-based, preventive protocols of care must be implemented in order to provide optimal care and prevent costly complications.
During the past several decades o wound care history, major advances have been made that address biochemical events occurring in skin. Manufacturers of skin and wound care products are partnering with clinicians to identify materials that help manage simple and complex skin conditions and wounds. A solid foundation of information now exists to facilitate skin and wound healing. Yet despite widely accepted standards of practice and well-intentioned healthcare practitioners, managing the patient’s skin in the presence of incontinence remains a challenge.
Information has shown that:
• As of 1996, the direct costs of caring for all ages of persons with incontinence was documented at $11.2 billion annually in the community and $5.2 billion in nursing homes1 and the numbers are increasing
• Fecal incontinence affects up to 5% of the general population and up to 39% of nursing home residents.2 In acute care, 33% of patients were reported to have fecal incontinence2 and 15% to 34% of hospitalized patients are incontinent of urine3
• The urinary tract is the most common site of nosocomial infection. More than 40% of the total number of nosocomial infections reported by acute-care hospitals are urinary tract infections (UTIs); they affect an estimated 600,000 patients per year. Of these infections, 66% to 86% follow introduction of instrumentation into the urinary tract, mainly urinary catheterization4,5
• Urinary incontinence affects 38% of women and 17% of men age 60 and older2
• Perineal skin damage secondary to incontinence has been reported to occur in 31% of acute care patients and 41% of long-term care patients6
• Perineal dermatitis has been reported to increase risk for UTIs, microbial skin infections, and pressure ulcers7
• Fecal incontinence has been documented as one of the most common risk factors for pressure ulcer development.8
These facts and figures tell only part of the story. Alteration in skin integrity secondary to incontinence directly impacts patients and caregivers. Frustration and confusion continue to be problematic among clinicians trying to determine which skin care products/devices are appropriate to use with which type of incontinence, when to change the type of product/device, how to document the condition of the skin appropriately, and how to track outcomes based on care practices. Despite the availability of published clinical practice guidelines,1,5,9-11 research results, and documented best practices, skin breakdown remains a key issue.
This article is intended to highlight changes to reimbursement policies and underscore the need not only to develop but also to implement and follow protocols for incontinence management.
2008 Fiscal Year (FY08) Inpatient Prospective Payment System (IPPS) Final Rule
Awareness of coordinated skin (and wound) care programs has heightened with the advent of the new 2008 Centers for Medicare and Medicaid Services (CMS) Guidelines.12 As of October 1, 2008, Medicare can deny payment for eight costly and sometimes deadly preventable hospital-acquired conditions (HACs) (see Table 1) — ie, those that develop during an inpatient stay (they do not apply to the patient admitted with these conditions). In addition to the national CMS rule, states have already enacted similar guidelines with fines associated with the negative outcomes.13 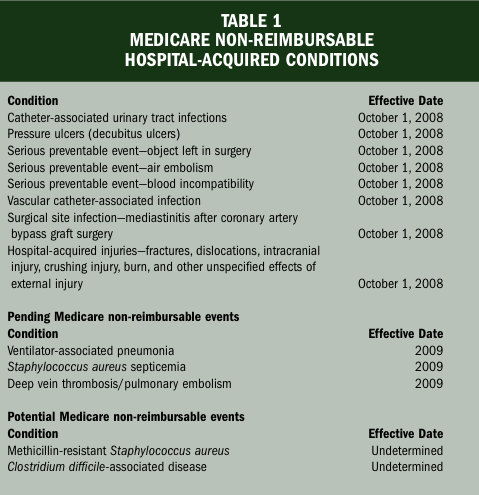 Moreover, three additional HACs are proposed for inclusion for 2009 and additional HACs undergoing further investigation are to be included in the future (see Table 1).
Moreover, three additional HACs are proposed for inclusion for 2009 and additional HACs undergoing further investigation are to be included in the future (see Table 1).
2008 Fiscal Year (FY08) IPPS Final Rule: Background
The 2008 IPPS final rule includes some of the most challenging rule changes since the prospective payment system was introduced in 198314 (see “History of Medicare Hospital Reimbursement”). The CMS projects that under this final rule, payments will better reflect the severity of illness and the cost of treating Medicare beneficiaries. One example of significant cost savings is reported in a recent respective review article, “Modifying DRG-PPS to Include Only Diagnoses Present on Admission: Financial Implications and Challenges.”15
To facilitate assimilation of the new ruling, conditions present on acute care admission will need to be identified by the clinical staff inclusive of the attending physician. It must be emphasized that physician documentation is crucial to obtaining reimbursement.
Present On Admission
The CMS began requiring acute care facilities to start the process of determining conditions “present on admission” (POA) in October 2007. The POA indicator helps identify conditions such as pressure ulcers and catheter-associated UTIs that developed during a hospital stay. Once the hospital becomes familiar with POA coding, appropriate policies, procedures, pathways, and algorithms specific to the eight identified HACs should be scrutinized. Clinician documentation of conditions POA impact the reimbursement received by the acute care facility; therefore, adherence to best clinical practices is crucial. All HACs identified should be of concern for all facilities; the two conditions that impact patients with incontinence are catheter-associated UTIs and pressure ulcers. Information regarding POA is available at: www.cms.hhs.gov/HospitalAcqCond.
Catheter-associated UTIs. The CMS included this complication with the objective to reduce the rate of UTIs through decreased use of indwelling catheters in the hospitalized Medicare patient. According to information in the final rule within this guideline,12 catheter-associated UTIs are the most common nosocomial infection; thus, this condition meets the criteria of high volume with associated costs:
CDC reports that there are 561,667 catheter-associated urinary tract infections per year. For FY 2006, there were 11,780 reported cases of Medicare patients who had a catheter-associated urinary tract infection as a secondary diagnosis. The cases had average charges of $40,347 for the entire hospital stay. According to a study in the American Journal of Medicine, catheter-associated urinary tract infection is the most common nosocomial infection, accounting for more than 1 million cases in hospitals and nursing homes nationwide.
Approximately 11.3 million women in the United States had at least one presumed acute community-acquired urinary tract infection resulting in antimicrobial therapy in 1995, with direct costs estimated at $659 million and indirect costs totaling $936 million. Nosocomial urinary tract infection necessitates one extra hospital day per patient or nearly 1 million extra hospital days per year. It is estimated that each episode of symptomatic urinary tract infection adds $676 to a hospital bill. In total, according to the study, the estimated annual cost of nosocomial urinary tract infection in the United States ranges between $424 and $451 million.
According to the CDC,5 “Catheter-associated urinary tract infections are caused by a variety of pathogens, including Escherichia coli, Klebsiella, Proteus, Enterococcus, Pseudomonas, Enterobacter, Serratia, and Candida. Many of these microorganisms are part of the patient’s endogenous bowel flora, but they can also be acquired by cross-contamination from other patients or hospital personnel or by exposure to contaminated solutions or non-sterile equipment.”
Additionally, after extensive research, the CMS determined that clearly defined prevention guidelines are available to assist practitioners in determining the length of time a urinary catheter may remain in place.5,12 The summary of the latest recommendations presented by the CDC appears in Table 2. Prevention guidelines for avoiding catheter-associated UTIs are scheduled to be updated by the CDC’s Healthcare Infection Control Practices Committee (HICPAC).12 Additionally, and according to the final rule, the National Quality Forum (NQF) is currently working to update hospital-acquired infection definitions.12 The effort currently underway will update prevention guidelines that have been in place since 1981.12 Lastly, the final rule states that the prevention guidelines that currently exist will be updated before the October 1, 2008 implementation date of the provision.12 Acute care facilities should work closely with their attending physicians to establish the appropriate protocols and documentation requirements to support the criteria set forth in the final ruling.
 Pressure ulcers. The first criterion necessary for inclusion as HACs12 are distinct ICD-9 codes used to identify pressure ulcers. Additionally (as stated in the final rule), this condition is both high-cost and high-volume. According to the final rule in FY 2006, 322,946 cases of Medicare patients with a secondary diagnosis of pressure ulcer with an associated average cost of $40,381 per patient were reported.12
Pressure ulcers. The first criterion necessary for inclusion as HACs12 are distinct ICD-9 codes used to identify pressure ulcers. Additionally (as stated in the final rule), this condition is both high-cost and high-volume. According to the final rule in FY 2006, 322,946 cases of Medicare patients with a secondary diagnosis of pressure ulcer with an associated average cost of $40,381 per patient were reported.12
The final rule clearly defines prevention guidelines. These guidelines can be found at https://www.npuap.org/positn1.htm16 and https://www.ncbi.nlm.nih.gov/books/bv.fcgi?rid=hstat2.chapter.440911. Specific areas reviewed include Risk Assessment Tools and Risk Factors, Skin Care and Early Treatment, Mechanical Loading and Support Surfaces, and Education.
By including pressure ulcers as a HAC, the CMS hopes to 1) improve screening of patients for pressure ulcers on admission, 2) promote early identification of pressure ulcers to improve treatment, and 3) greatly improve patients’ quality of care.12
In order to fulfill the expectations of the provisions set forth in the final rule of 2008, acute care facilities will need to look closely at their admission guidelines for skin assessments and ensure documentation by the attending physician and hospital clinician. Improvements in the admission assessment will influence the associated diagnosis related group (DRG) classifications at discharge, which in turn will affect the reimbursement received for an individual inpatient stay. The CMS now expects physicians and hospitals to perform a more accurate skin assessment on admission to identify pressure ulcers earlier and institute appropriate prevention and management pathways.12 Therefore, the use of accurate assessment skills, coupled with coordinated skin care formularies and management pathways based on clinical practice guidelines, should be initiated on all patients incontinent of urine and feces admitted to the facility. These pathways should be initiated as either a prevention pathway (patients with intact skin) and/or intervention pathway (patients with skin injury).
Skin Care Formularies
The fundamental building blocks addressing prevention of skin breakdown are generally overshadowed by the large number of intervention strategies available for patients with chronic wounds. To that end, the clinician must understand the anatomy and physiology of the skin, current clinical practice guidelines, and indications and contraindications of skin care products used in clinical practice.17
Products and devices to consider when creating the skin care formulary to maintain or manage skin integrity relevant to incontinence and/or divert, contain, and manage urinary incontinence and the consistency of stool for fecal incontinence should include17:
• Topical antifungals and antimicrobials — products that inhibit the growth of organisms that cause superficial skin infections such as yeast or Candida albicans
• Liquid skin protectants (also called skin sealants) — products that protect the skin by forming a transparent protective barrier
• Skin cleansers — products to remove urine and/or feces without patient discomfort that also provide moisture and are pH-balanced
• Moisture barriers (also called skin protectants) — ointments, creams, or pastes that protect the skin from the effects of urinary and fecal incontinence by shielding the skin from irritants or moisture such as dimethicone, petrolatum, and zinc oxide
• Therapeutic moisturizing products — lotions and creams that replace lost lipids
• Intermittent or indwelling catheters — devices that divert the urine. Caution should be exercised regarding length of use; a thorough urological assessment must be completed by a qualified professional
• Fecal collectors — devices used to contain liquid feces through a closed system. In clinical practice, fecal collectors are generally considered only for short-term (<2 days) use
• Indwelling bowel catheters (also known as bowel management systems) — devices that divert fecal matter to minimize contact with patient skin and facilitate collection for patients requiring stool management. One product, the Zassi® Bowel Management System (Hollister Inc, Libertyville, Ill) also provides access for colonic irrigation, allowing the irrigant (typically lukewarm tap water) to be retained in the rectum to help break up thickening stool. According to manufacturer indications, this device can remain in place up to 29 days (independent studies have demonstrated a median dwell time of between 10 and 22.5 days). This device has US Food and Drug Administration (FDA) clearance for rectal administration of enemas/medications; some institutions have had success with administration of vancomycin for Clostridium difficile and lactulose for hepatic encephalopathy.
• Support surfaces and additional adjunctive therapies and products — pressure-reducing or -relieving devices as well as offloading devices should be considered when choosing products for patients at risk for skin breakdown.
It is paramount that providers take proactive steps in clinical practice to develop sound skin care prevention and intervention pathways. The following work plan was created to help the reader understand the importance of accurate assessment and management using the guidelines referenced in the CMS IPPS final rule related to catheter-associated UTIs and pressure ulcer prevention. This compilation depicting a typical case is intended to provide a patient management approach that incorporates CMS and CDC guidelines. 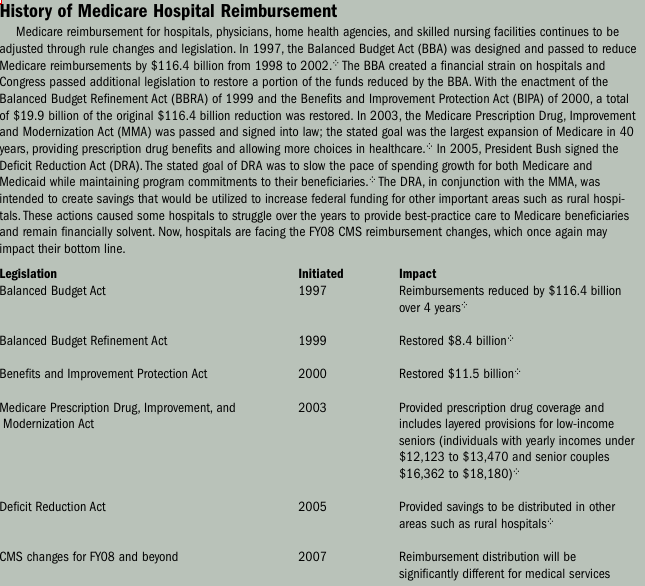
Sample Patient Scenario with Work Plan
Patient history. An 83-year-old female resident of an extended care facility was admitted to the Intensive Care Unit of the hospital. Her admitting diagnoses included acute exacerbation of chronic obstructive pulmonary disease with pneumonia, failure to thrive, and extensive weight loss. She had a history of right-sided paralysis with limited movement of right leg and arm. She required a splint on her right hand for contracture prevention. She did not respond to verbal commands consistently.
Clinical assessment. A thorough nursing admission assessment was conducted and documented by the intensive care clinical staff per hospital protocol. This assessment included an extensive skin and pressure ulcer risk assessment based on the hospital’s protocols. The skin assessment revealed intact skin with the notation of slightly reddened areas on the right heel and right elbow. The right-hand splint was in place. The patient was found to be at high risk for pressure ulcer development following the completion of the hospital’s validated pressure ulcer risk assessment tool. The patient was incontinent of large amounts of liquid stool and urine. A pain assessment tool was completed and no non-verbal pain indicators were noted. Physician assessment concurred with historic and admission assessment findings.
Orders. The physician wrote for urine culture and sensitivity and stool culture for C. difficile following placement of indwelling bowel catheter. If culture results were positive, vancomycin was to be provided. In addition, the physician requested a chest X-ray to rule out pneumonia and implementation of pressure ulcer prevention measures, including heel and elbow protectors, specialty mattress, Physical Therapy evaluation, and dietitian consultation. A Certified Wound, Ostomy Continence Nurse was to be consulted for skin care assessment and recommendations. An indwelling Foley catheter was to be placed for incontinence as well as a bowel management device or indwelling bowel catheter to manage bowel effluent until the patient regained mobility. The hospital’s Intensive Care Guidelines for patients at high risk for skin breakdown were to be followed and blood counts and pre-albumin were to be monitored.
Specific skin care recommendations per hospital protocol. To address skin compromise, skin assessments were to be conducted every shift. The patient was to be turned and repositioned at least once an hour and more frequently if skin showed signs of redness.18 The patient’s bed was to be maintained at a 30-degree angle. She was to be placed on site-specific pressure-reducing surfaces to prevent pressure on bony prominences and extremities. Her skin was to be kept skin dry, well hydrated, and free from injury; skin care barriers were to be applied to prevent skin breakdown and lifting devices employed to avoid friction and shearing during movement. Nutritional support was to be provided and mobility and activity maintained.
Indwelling catheter care (clinician should refer to the hospital’s indwelling catheter care policies and procedures). To facilitate best-practice care, personnel were to be educated in correct techniques of catheter insertion and care. The patient was to be catheterized only when necessary. Handwashing was emphasized. The catheter should be securely inserted using aseptic technique and sterile equipment and closed sterile drainage maintained to ensure unobstructed urine flow. Urine samples could be obtained aseptically. The catheter was to be changed and secured properly per hospital policy.
Indwelling bowel catheter management (clinician should refer to the hospital’s indwelling bowel catheter policies and procedures). Similar in practice to urinary catheter use, personnel must be educated in correct techniques of catheter insertion and care and changes per hospital protocol. The catheter must be secured to prevent migration and/or inadvertent removal. Handwashing must be emphasized, stool samples obtained aseptically, and the bowel catheter contents disposed of per hospital protocol.
Clinical goals. All measures described were implemented to prevent skin breakdown related to pressure ulcers, to prevent skin breakdown related to incontinence, to protect intact skin from incontinence and moisture, and to decrease sequelae from immobility.
Documentation
The documented provision of care details become facts for the medical record. Words and terms such as consent, release of information, compliance with standards, and patient confidentiality are increasingly familiar in the clinical workplace. The clinician should understand that the medical record serves as the vehicle for demonstrating the planning, evaluation, and coordination of patient care. Documentation also supports utilization of processes, research, and education. Documented details are not only imperative for clinical outcomes and benchmarking, but also could be viewed as: 1) a legal instrument in a malpractice claim, 2) a source of information to support the level of service billed, and 3) a record to substantiate that clinicians meet accrediting agency standards of care.
The release of the FY08 final rule appears to affirm CMS’ expectation to improve Medicare patients’ quality of care. This is a clear indication that hospital-developed protocols should reflect the criteria set forth in the final rule, which include documentation of POA conditions, prevention guidelines addressing risk of acquiring conditions, and identification of conditions that can occur even with preventative measures. Thus, to meet the specific guidelines for the identification of diagnosis coding for a specific inpatient stay, the medical record should accurately reflect and document the work performed and recorded by the clinician and attending physician.
Conclusion
Urinary and fecal incontinence present many challenges to the bedside clinician and physician as well as the patient. Skin care formularies detailing appropriate product choices are needed to manage each patient’s condition present on admission.
Medicare reimbursement changes will affect how facilities are paid in the next several years. Educating and re-educating clinical staff and attending physicians on the need for accurate assessments, prevention guideline implementation, and accurate documentation will impact coding and reimbursement and most importantly, reinforce the need for best practice in the care of individuals whose incontinence threatens skin integrity.
1. Fantl JA, Newman DK, Colling J, et al. Urinary Incontinence in Adults: Acute and Chronic Management. Clinical Practice Guideline No. 2, 1996 Update. Rockville, Md: U.S. Department of Health and Human Services. Public Health Service. Agency for Health Care Policy and Research. AHCPR Publication No. 96-0682. March 1996.
2. NIH State-of-the-Science Conference: Prevention of Fecal and Urinary Incontinence in Adults. December 10–12, 2007. Available at: http://consensus.nih.gov/2007/2007IncontinenceSOS030main.htm. Accessed November 27, 2007.
3. Driver D. Perineal dermatitis in critical care patients. Critical Care Nurse. 2007;27(4):42–46.
4. Centers for Disease Control and Prevention (CDC). Urinary incontinence among hospitalized persons aged 65 years and older – United States, 1984-1987. Morbidity and Mortality Weekly Report. 1991;40(26):433–436.
5. Wong E, Hooton T. Centers for Disease Control (CDC). Guideline for Prevention of Catheter-associated Urinary Tract Infections. February 1, 1981. Available at: http://www.cdc.gov/ncidod/dhqp/gl_catheter_assoc.html. Accessed October 1, 2007.
6. Nix D, Ermer-Seltun J. A review of perineal skin care protocols and skin barrier product use. Ostomy Wound Manage. 2004;50(12):59–67.
7. Gray M. Preventing and managing perineal dermatitis: a shared goal for wound and continence care. J WOCN. 2004;31(1 suppl):S2–S9.
8. Bliss DZ, Johnson S, Savik K, Clabots CR, Gerding DN. Fecal incontinence in hospitalized patients who are acutely ill. Nurs Res. 2000;49(2):101–108.
9. Acute Pain Management Guideline Panel. Clinical Practice Guideline: Acute Pain Management: Operative or Medical Procedures and Trauma. Rockville, Md: US Department of Health and Human Services. Public Health Service. Agency for Health Care Policy and Research; February 1992. AHCPR Pub. No. 92-0032.
10. Panel for the Prediction and Prevention of Pressure Ulcers in Adults. Clinical Practice Guideline Number 3: Pressure Ulcers in Adults: Prediction and Prevention. Rockville, Md: US Department of Health and Human Services. Public Health Service. Agency for Health Care Policy and Research, 1992. AHCPR Publication 92-0047.
11. Wound, Ostomy, and Continence Nurses Society. Guideline for Prevention and Management of Pressure Ulcers, WOCN Clinical Practice Guideline Series. Glenview, Ill: WOCN Society;2003:14.
12. Medicare Program: Changes to the Hospital Inpatient Prospective Payment Systems and Fiscal Year 2008 Rates. Federal Register. 2007;72:162. Centers for Medicare and Medicaid Services. 42 CFR Parts 411, 412, 413, and 489. Available at: http://www.cms.hhs.gov/quarterlyproviderupdates/downloads/cms1533fc.pdf. Accessed October 2, 2007.
13. Cody DA, Pitts P. United States: California update: new laws on adverse event reporting and facility inspection. Available at: http://www.mondaq.com/article.asp?article_id=44316. Accessed October 2, 2007.
14. Proposed Medicare Reimbursement Changes to Impact Hospitals Profitability. American Hospital Directory. Available at: http://www.ahd.com/press_rel070710.html. Accessed October 1, 2007.
15. Zhan C, Elixhauser A, Friedman B, Houchens R, Chiang YP. Modifying DRG-PPS to include only diagnoses present on admission: financial implications and challenges. Med Care. 2007;45(4):288–291.
16. National Pressure Ulcer Advisory Panel. Statement on pressure ulcer prevention. 1992. Available at: http://www.npuap.org/positn1.htm. Accessed October 1, 2007.
17. Hess CT. Clinical Guide to Skin and Wound Care, 6th ed. Ambler, Pa: Lippincott Williams & Wilkins;2007.
18. Revis DR. Decubitus ulcers. Available at: http://emedicine.com/med/topic2709.htm. Accessed November 27, 2007.
19. Volpp KG, Konetzka RT, Zhu J, Parsons L, Peterson E. Effect of cuts in Medicare reimbursement on process and outcome of care for acute myocardial infarction patients. National Registry of Myocardial Infarction Investigators. American Heart Association. 2005;112:2268–2275. Available at: http://www.circ.ahajournals.org/cgi/content/full/112/15/2268. Accessed October 1, 2007.
20. Fact Sheet: Medicare Prescription Drug, Improvement, and Modernization Act of 2003. White House Press Release. December 8, 2003. Available at: http://www.whitehouse.gov/news/releases/2003/12/20031208-3.html. Accessed October 1, 2007.
21. Fact Sheet: President Bush Signs the Deficit Reduction Act. White House Press Release. February 8, 2006. Available at http://www.whitehouse.gov/news/releases/2006/02/20060208-9.html. Accessed October 1, 2007.
