



The Yellow-Red-Black Bladder Diary: Red-Yellow-Black is Not Just for Wounds
Abstract
The Red-Yellow-Black (RYB) wound classification system was introduced to the US in the late 1980s for the purpose of simplifying wound assessment and guiding treatment. Although the color system was found to have limitations for wound care, the colors (in revised order) may be useful for a bladder diary. Colored pencils are used to record fluid intake and voided output. For fluid intake, yellow signifies nonirritants (water); red, low bladder irritants (alcoholic, artificially sweetened, carbonated, or citrus beverages); and black, high bladder irritants (caffeinated beverages).
For voided output, yellow denotes continent voids and red, incontinent voids. Output quantity is measured using a commode “hat”. The completed diary allows the practitioner to tabulate the colored daily rows and quickly assess progress weekly or monthly and provide appropriate treatment/advice. The YRB diary was used successfully by a 78-year old woman with urge incontinence without evidence of stress incontinence. Modifications to the YRB diary can be made when additional data need to be collected. Studies to evaluate optimal usage criteria of bladder diaries are needed.
Dr. Faller is a board-certified ET Nurse/Clinical Specialist in private practice. Please address correspondence to: Nancy Ann Faller, RN, PhD, ET Nurse, 380 Wilson Street, Carlisle, PA 17013; email: nafaller@aol.com.
The Red-Yellow-Black (RYB) wound classification system was introduced to the US from Europe in the late 1980s1 by Marion Laboratories (now Marion Merrell Dow) (see Figure 1). The colors were heralded for simplifying wound assessment to direct wound treatment. This system had at least two problems from its inception. First, the RYB assessment only includes the wound bed. Additional variables — ie, wound depth, size, undermining, and tunneling; wound shape, dimensions, and volume; wound edges and surrounding skin; wound exudate and odor; and wound stage (if a pressure ulcer) are not included. Furthermore, this system does not accommodate for the presence of foreign bodies (eg, mesh, prosthesis, and sutures) or  underlying structures (eg, tendon and bone) in the wound nor does it facilitate assessment of wounds with various tissue in the wound bed.2,3
underlying structures (eg, tendon and bone) in the wound nor does it facilitate assessment of wounds with various tissue in the wound bed.2,3
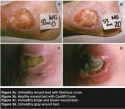
Second, the colors and suggested treatments are problematic. Red wounds (see Figure 2a) were described as being in one of three reparative phases of healing (reactive, regenerative, or reconstructive). This description does not allow for either a healthy muscular wound bed immediately post dehiscence or debridement (see Figure 2b) or an unhealthy stagnant granulating wound bed months post dehiscence or debridement (see Figure 2c). Yellow wounds were described as infected or fibrinous and not ready to heal (see Figure 3a), not taking into consideration the healthy wound bed with Cardiff Cover as described by Harding4 (see Figure 3b),  nor the unhealthy wound bed with cream, beige, brown, green, or gray tissue (see Figure 3c,d). Black wounds were described as covered with a dehydrated eschar; the suggested intervention was debridement, an intervention not necessarily appropriate for all wounds or for all patients (eg, patients with dry heal pressure ulcers or arterial ulcers)5-7 (see Figure 4a,b).
nor the unhealthy wound bed with cream, beige, brown, green, or gray tissue (see Figure 3c,d). Black wounds were described as covered with a dehydrated eschar; the suggested intervention was debridement, an intervention not necessarily appropriate for all wounds or for all patients (eg, patients with dry heal pressure ulcers or arterial ulcers)5-7 (see Figure 4a,b).
Primarily, the problems described result from over-simplification of wound assessment; plus, the validity and reliability of the RYB instrument were never established. However, despite its many disadvantages, the RYB wound classification  system has important advantages — mainly, it is easy to teach and use — making it an excellent starting point for novice practitioners or other nonprofessional caregivers, including family members. Prudently transferring this uncomplicated approach may offer a worthwhile alternative to continence care. The purpose of this case study is to describe the use of these colors to classify fluid intake and output for a bladder diary.
system has important advantages — mainly, it is easy to teach and use — making it an excellent starting point for novice practitioners or other nonprofessional caregivers, including family members. Prudently transferring this uncomplicated approach may offer a worthwhile alternative to continence care. The purpose of this case study is to describe the use of these colors to classify fluid intake and output for a bladder diary.
Literature Review
The International Continence Society (ICS)8 has identified three tools for measuring lower urinary tract symptoms: the micturition chart (records the time of continent voids), the frequency volume chart (records time and volume of continent voids), and the bladder diary. The bladder diary records time and volume of all voids, pad usage, fluid intake, and degree of urgency. Although the bladder diary provides more detailed data than the micturition chart and the frequency volume chart, it may be more difficult to complete.9,10 Various bladder diary designs are available.9,11,13,14,16
A recent best practice document (BPD)11 reinforces the usefulness of a bladder diary not only for assessment, but also for monitoring urinary incontinence or voiding dysfunction treatment. In addition to assessment and monitoring treatment, the completed bladder diary demonstrates patient motivation to the practitioner10 and can be fundamental to continence research.10,12
Bladder diary selection is based on availability, type of suspected voiding dysfunction, data desired, and patient or caregiver willingness to complete the tool.9,10 Occasionally, bladder diaries do not meet the needs of particular patient populations. When this occurs, an existing bladder diary is modified or a new bladder diary is designed by the practitioner.11,13
The use of colors for recording voids was reported previously. Clay’s14 “Habit Retraining Chart” was described for use as a “Voiding Record in a 457-bed, long-term/rehab/tuberculosis hospital by Autry et al.15 The tool utilizes four colors of self-adhesive dots to document micturition: dry (green) or wet (red) and voiding (blue) or not voiding (yellow). Therefore, it only meets the ICS criteria as a micturition chart because it does not record volume of voids. In addition, with handling and age, the dots may be lost from the record.
Design of the Yellow, Red, and Black for a Bladder Diary
Although use of the RYB color system can be problematic for wound assessment and treatment, the colors re-ordered to yellow, red, and black — YRB — were helpful in the design of a weekly bladder diary. The new diary was designed for a patient who presented with urge incontinence without evidence of stress incontinence when existing diaries seemed to be more complex than necessary. Data collected were specific to this patient— ie, frequency, urgency, and urge incontinence — and thought to be related to bladder irritability due to amount and type of fluid intake.
The YRB diary collects data on fluid intake and voided output. Intake includes quantity and quality of fluid. Output includes quantity and quality of void. Although this diary was not designed to collect activity data, all other data suggested by the BPD are collected — ie, time, amount, and type of fluid intake as well as time and amount of voided output, both continent and incontinent.
Fluid intake is recorded in ounces (oz) and voided output is recorded as small — 249 cc or less or damp; medium — 250 cc to 350 cc or wet; large — 250 cc to 450 cc or soaked; and extra large — 451 cc or more or change of clothing 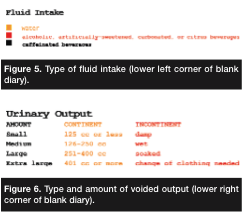 necessary. For fluid intake, yellow is used for nonirritants (water), red for low bladder irritants (alcoholic beverages, artificially sweetened, carbonated, or citrus beverages), and black for high bladder irritants (caffeinated beverages) (see Figure 5). For voided output, yellow is used for continent voids and red for incontinent voids (see Figure 6).
necessary. For fluid intake, yellow is used for nonirritants (water), red for low bladder irritants (alcoholic beverages, artificially sweetened, carbonated, or citrus beverages), and black for high bladder irritants (caffeinated beverages) (see Figure 5). For voided output, yellow is used for continent voids and red for incontinent voids (see Figure 6).
Use of the Yellow, Red, and Black Bladder Diary
The practitioner provides the patient with a blank diary (see Figure 7), three colored pencils (yellow, red, and black), and a commode “hat” for measuring output. The patient is given instructions on completing the diary. Intake is recorded by filling the squares corresponding to the approximate time of day. The amount of fluid is recorded by filling one box for each ounce of intake. The type of fluid isrecorded by filling the boxes with the color indicated for the specific intake (found in the lower left corner of the diary) (see Figure 5). The time is recorded on line 1. Output is recorded on lines 1 and 2 corresponding to the approximate time of day. The amount and type of void is recorded on line 2 with the amount and color indicated for the output (found in the lower right corner of the diary) (see Figure 6). 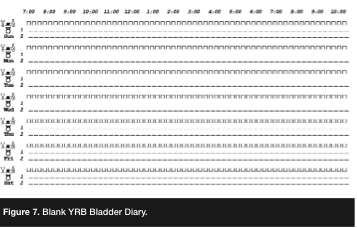
The completed diary allows the practitioner to tabulate the daily rows and quickly assess progress over an appropriate time period (eg, weekly or monthly). Changes then can be made to the treatment plan via phone consultation or an office visit.
Case Study
Ms. E was a 78-year-old woman who presented with urge incontinence (failure to store urine secondary to an overactive bladder) without evidence of stress incontinence (failure to store urine secondary to an underactive sphincter). Additional health problems included osteoarthritis (not limiting ability to toilet), constipation (managed with a stool softener), hypertension (managed with an angiotensin receptor blocker), sleep apnea (managed with continuous positive airway pressure [CPAP]), and supraventricular tachycardia (managed with a beta-blocker).
Presenting symptoms included frequency, urgency, and urge incontinence. Ms. E’s etiology, assessed by the practitioner, was bladder irritability due to limited fluid intake consisting primarily of high bladder irritants (alcoholic, artificially sweetened, caffeinated, carbonated, and citrus beverages). To help this patient visualize the quantity and quality of her fluid intake, the practitioner designed a bladder diary. This diary accounted for the needed data as well as the patient’s skill level.
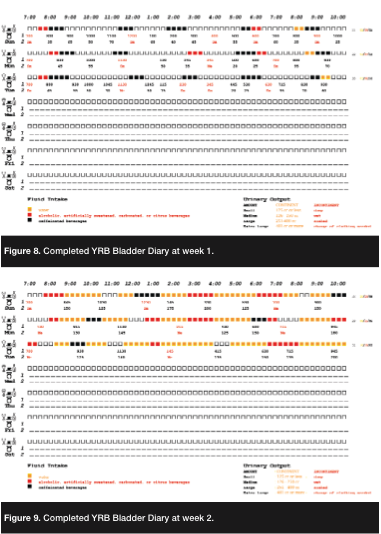 The completed diary was reviewed by the practitioner at the end of week one (see Figure 8) and confirmed Ms. E’s poor fluid intake. She was advised about the relationship between intake and urinary symptoms and counseled on increasing fluid intake while decreasing irritant fluids. No other interventions were introduced.
The completed diary was reviewed by the practitioner at the end of week one (see Figure 8) and confirmed Ms. E’s poor fluid intake. She was advised about the relationship between intake and urinary symptoms and counseled on increasing fluid intake while decreasing irritant fluids. No other interventions were introduced.
At the end of week 2, the completed diary (see Figure 9) demonstrated an improvement in both fluid intake and urinary symptoms. Ms. E was told to continue fluid modifications with the goal of filling each box daily for a total intake of 40 oz (1,200 cc). The completed diary at the end of week three (see Figure 10) again demonstrated a marked improvement in both fluid intake and urinary symptoms. Ms. E appreciated the ability to visualize the colors and the changes over the 3 weeks and was free of her presenting complaints.
Discussion
The YRB diary was designed specifically for this patient. Frequency, urgency, and urge incontinence were considered to be related to bladder irritability due to poor amount and type of fluid intake. Because it focuses on quantity or amount of fluid and quality or type of fluid, this diary may not be as useful for patients with suspected stress incontinence; however, practitioners can modify the diary to collect additional data.

The burden of consistently completing hand-written diaries has been identified.16 Patients must be motivated to fill out a documentation tool each day and must have legible penmanship. Although the YRB diary minimizes the burden of handwriting and legibility, consistent completion remains an issue — not all patients will find it easy to complete.
The original four-color data collection studies were completed in institutional settings with colored self-adhesive dots.14,15 If securing three colored pencils is a burden, the YRB diary might have more use in a care setting where the burden of immediate access to these supplies could be minimized. Alternatively, four colored pencils could be used for the originally described tools instead of the colored self-adhesive dots.
A recent review17 addressed the advantages of handheld-computer data collection compared to traditional paper data collection. Two of the 16 studies were specific to urinary continence. The adaptation of the YRB diary to computerized data collection would provide an alternative to needing three colored pencils for patients or caregivers who are techno-friendly.
As recommended in the BPD,11 research is needed related to the use of bladder diaries. Questions remain regarding appropriate use in terms of patients, populations, providers, interpretation of the results, and resultant appropriate interventions. The YRB bladder diary is no exception and should be included in future research trials.
Conclusion
Although not recommended for wound care, the revised RYB color system was useful for this patient with urinary incontinence. In this case study, the YRB bladder diary was easy for the patient to complete and easy for the practitioner to decipher. Modifications to the YRB diary can be made when additional data need to be collected.
1. Cuzzell JZ. The new RYB color code: next time you assess an open wound, remember to protect red, cleanse yellow, and debride black. Am J Nurs. 1988:88(10):1342–1346.
2. Krasner D. Wound care: how to use the red-yellow-black system. Am J Nurs. 1995:95(5):44–47.
3. van Rijswijk L, Catanzaro J. Wound assessment and documentation. In: Krasner DL, Rodeheaver GT, Sibbald RG (eds). Chronic Wound Care: A Clinical Source Book for Health Care Professionals, 4th ed. Malvern, PA: HMP Communications;2007;113–126.
4. Grey JE, Enoch S, Harding KG. ABC of wound healing. BMJ. 2006;332:285–288.
5. Fowler E, Scott-Williams S, McGuire JB. Practice recommendations for preventing heel pressure ulcers. Ostomy Wound Manage. 2008:54(10):42–57.
6. Langemo D, Thompson P, Hunter S, Hanson D, Anderson J. Heel pressure ulcers: stand guard. Adv Skin Wound Care. 2008:21(6):293–294.
7. Holloway GA. Arterial ulcers: assessment, classification, and management. In: Krasner DL, Rodeheaver GT, Sibbald RG (eds). Chronic Wound Care: A Clinical Source Book for Health Care Professionals, 4th ed. Malvern, PA: HMP Communications;2007;443–449.
8. Abrams P, Cardozo L, Fall M, et al. The standardisation of terminology of lower urinary tract function: report from the Standardisation Sub-committee of the International Continence Society. Neurourol Urodyn. 2002:21(2):167–178.
9. Gray ML, Moore KN. Assessment of patients with urinary incontinence. In: Doughty DB (ed). Urinary & Fecal Incontinence: Current Management Concepts. St. Louis, MO: Mosby;2006:341–412.
10. Krissovich M. Pathology and management of the overactive bladder. In: Doughty DB (ed). Urinary & Fecal Incontinence: Current Management Concepts. St. Louis, MO: Mosby;2006:109–165.
11. Wound, Ostomy, and Continence Nurses Society Clinical Practice Continence Subcommittee. Bladder Diary: A Best Practice Document for Clinicians. Mt. Laurel, NJ: Wound, Ostomy, and Continence Nurses Society;2007.
12. Irby LA. Using the bladder diary as a tool to improve home care outcomes. J WOCN. 2008:35(3 suppl):S40–S41.
13. Hughes E, Anderson CL. The voiding record: a new approach to an old problem. Geriatr Nurs. 1992:13(2):90–93.
14. Clay E. Urinary continence/incontinence. Habit retraining: a tested method to regain urinary control. Geriatr Nurs. 1980:1(4):252–254.
15. Autry D, Lauzon F, Holliday P. The voiding record: an aid to decreasing incontinence. Geriatr Nurs. 1984:5(1):22–25.
16. Pfister SM. Bladder diaries and voiding patterns in older adults. J Gerontol Nurs. 1999:25(3):36–41.
17 Lane SJ, Heddle NM, Arnold E, Walker I. A review of randomized controlled trials comparing the effectiveness of hand-held computers with paper methods for data collection. BMC Med Inform Decis Mak. 2006:6(23):31.
