


The Effect of Intermittent and Variable Negative Pressure Wound Therapy on Wound Edge Microvascular Blood Flow
Abstract: Negative pressure wound therapy (NPWT) alters wound edge microvascular blood flow. Some preclinical data suggest that cycling between low and high negative pressure may be more beneficial than continuous NPWT. The purpose of this in vivo study was to compare the effect of intermittent negative pressure (cycled either from 0 to -75 or to -125 mm Hg) and variable negative pressure (cycled from -10 to -75 or -125 mm Hg or from -45 to -75 or -125 mm Hg) on wound edge microvascular blood flow. Using a peripheral wound model (n = 8 domestic 70-kg pigs), intermittent and variable NPWT was applied to surgically created wounds (5 cm diameter, 2 cm depth) for five cycles of 5 minutes of high and 2 minutes of low pressure. Blood flow was measured using laser Doppler velocimetry in subcutaneous and muscle tissue at 0.5 and 2.5 cm from the wound edge. When NPWT was applied, blood flow decreased an average of 29% ± 2% in muscle tissue and 22 % ± 4% in subcutaneous tissue at -75 mm Hg at 0.5 cm from the wound edge and increased an average of 20% ± 6% for -75 mm Hg at 2.5 cm from the wound edge. Blood flow changed repeatedly when negative pressure was cycled. Large gradients between the cycled pressures (eg, -10 to -75 mm Hg) resulted in greater blood flow alterations than smaller (eg, -45 to -75 mm Hg) gradients. Blood flow alternations were similar between low-pressure settings of -10 mm Hg (variable NPWT) and 0 mm Hg (intermittent NPWT) and between high-pressure settings of -75 or -125 mm Hg. Both intermittent and variable NPWT result in a beneficial combination of increased blood flow, known to facilitate oxygenation and nutrient supply, and decreased blood flow, known to stimulate angiogenesis and granulation tissue formation. Cycling the negative pressure may be especially advantageous when treating poorly vascularized tissue. In cases where intermittent therapy causes patient discomfort, variable therapy may be superior.
Potential Conflicts of Interest: The authors have nothing to disclose. The study was financially supported by the Åke-Wieberg Foundation, the Magn. Bergvall Foundation, the Swedish Medical Association, the Royal Physiographic Society in Lund, the Swedish Medical Research Council, the Crafoord Foundation, the Swedish Government Grant for Clinical Research, and Prospera Fort Worth, TX).
Please address correspondence to: Malin Malmsjö, MD, PhD, BMC A13, 221 84, Lund, Sweden; email: malin.malmsjo@gmail.com.
Negative pressure wound therapy (NPWT) entails sealed, airtight application of negative pressure to a wound. The precise mechanism by which negative pressure brings about wound healing is not known; however, it has been shown that the suction force created by subatmospheric pressure enables drainage of excessive fluid and debris and induces mechanical deformation of the wound edge tissue.1-3 Furthermore, NPWT covers the wound, promoting a moist wound healing environment4; studies indicate that it reduces bacterial colony counts, increases granulation tissue formation,2 removes edema,5 stimulates cell-mediated immune response,6 decreases blood vessel permeability,7 and stimulates angiogenesis and blood flow to the wound margins.8,9
 It has been suggested that the beneficial effects of NPWT on wound healing are enhanced if the level of negative pressure is varied during the treatment.2 Intermittent NPWT involves varying between atmospheric and subatmospheric pressure; variable NPWT involves varying between two different subatmospheric pressures. It has been shown2 that intermittent NPWT with pressure settings of 0 and -125 mm Hg stimulates more tissue granulation than continuous NPWT at -125 mm Hg. Intermittent negative pressure (using -125 mm Hg) also has been shown in vitro to promote proliferation and endothelial cell migration.10 A few studies1,2,10-15 address the biological effects of intermittent NPWT but no studies have been published on variable NPWT. Therefore, it is not known which pressure settings have the most biological effects. Furthermore, no study has yet been performed to examine in detail the effect of intermittent or variable negative pressure on wound edge microvascular blood flow.
It has been suggested that the beneficial effects of NPWT on wound healing are enhanced if the level of negative pressure is varied during the treatment.2 Intermittent NPWT involves varying between atmospheric and subatmospheric pressure; variable NPWT involves varying between two different subatmospheric pressures. It has been shown2 that intermittent NPWT with pressure settings of 0 and -125 mm Hg stimulates more tissue granulation than continuous NPWT at -125 mm Hg. Intermittent negative pressure (using -125 mm Hg) also has been shown in vitro to promote proliferation and endothelial cell migration.10 A few studies1,2,10-15 address the biological effects of intermittent NPWT but no studies have been published on variable NPWT. Therefore, it is not known which pressure settings have the most biological effects. Furthermore, no study has yet been performed to examine in detail the effect of intermittent or variable negative pressure on wound edge microvascular blood flow.
The aim of this experimental in vivo study was to compare the effect of intermittent negative pressure (cycled either from 0 to -75 or to -125 mm Hg) and variable negative pressure (cycled from -10 to -75 or -125 mm Hg or from -45 to -75 or -125 mm Hg) on wound edge microvascular blood flow.
Material and Methods
Animals. Eight healthy domestic pigs of both sexes with a mean body weight of 70 kg were fasted overnight with free access to water. The Ethics Committee for Animal Research, Lund University, Sweden approved the experimental protocol for this study. All animals received humane care in compliance with the European Convention on Animal Care.
Anesthesia and surgical procedure. An intramuscular injection of xylazine (Rompun® vet, 20 mg/mL; Bayer AG, Leverkusen, Germany; 2 mg/kg) mixed with ketamine (Ketaminol® vet, 100 mg/mL; Farmaceutici Gellini S.p.A, Aprilia, Italy; 20 mg/kg) was used for premedication. Anesthesia then was induced with intravenous sodium thiopental (Pentothal®, Abbot Scandinavia, Stockholm, Sweden; 4 mg/kg), and maintained throughout the experiment with a continuous infusion of fentanyl (Leptanal®; Lilly, France) in Ringer’s acetate (3.5 µg/kg/h) in combination with intermittent bolus doses of sodium thiopental. The animals were orally intubated with cuffed endotracheal tubes. Mechanical ventilation was established with a Siemens-Elema ventilator (Siemens-Elema AB, Solna, Sweden) in the volume-controlled mode (65% nitrous oxide, 35% oxygen). Ventilator settings were identical for all animals (respiratory rate, 15 breaths/minute; minute ventilation, 12 L/minute). A positive end-expiratory pressure of 5 cm H2O was applied. A Foley catheter was inserted into the urinary bladder through a suprapubic cystostomy.
A circular wound 5 cm in diameter by 2 cm deep, going through both subcutaneous and muscle tissue, was created on each pig’s back. Saline-soaked AMD gauze (Kendall Healthcare, Mansfield, MA) was used as wound filler. Gauze volume was approximately 1.5 times more than the wound volume to allow volume reduction during negative pressure application. A drainage tube was inserted into the gauze and connected to a vacuum source (Prospera PRO-III®, Prospera Technologies LLC, Fort Worth, TX). The wound then was sealed with transparent adhesive drape, which overlapped the wound margins by 10 cm. All measurements were made while the animals were anesthetized. Euthanasia was performed with a lethal dose (60 mmol) of intravenous potassium chloride when the animal was still anesthetized.
Laser Doppler velocimetry and NPWT settings. Microvascular blood flow was measured by laser Doppler velocimetry using a 4-channel Perimed PF5010 LDPM unit. Laser Doppler velocimetry, a technique that has been applied extensively to measure blood flow in flaps during plastic surgery procedures,16 quantifies the motion of red blood cells in a specific volume. A beam of laser light is carried by a fiber-optic probe. Light hitting moving blood cells undergoes a change in wavelength (Doppler shift), while light hitting static objects is unchanged. The distribution of magnitude and frequency of these changes in wavelength is directly related to the number and velocity of blood cells. The information is detected by a returning fiber, converted into an electronic signal, and analyzed.
In the current experiments, filament probes (Probe 418-1; Perimed, Stockholm, Sweden) were used to measure microvascular blood flow. A Venflon infusion cannula (1.4 mm in diameter; BD Medical, Franklin Lakes, NJ) was used to gain access to the tissue. The filament probe was inserted through the cannula and the cannula was then removed, leaving the filament probe in place. The filament probe was connected to the laser Doppler equipment. Filament probes were placed in either subcutaneous or muscle tissue at 0.5 cm and 2.5 cm from the wound edge. The probes were evaluated for adequate responses when negative pressure therapy was applied to the wound, enabling selection of four probes known to be fully functional.
The following series of intermittent and variable negative pressure were applied: 0 and -75 mm Hg, -10 and -75 mm Hg, 0 and -125 mm Hg, -10 and -125 mm Hg, -45 and -75 mm Hg, -45 and -125 mm Hg. Pressures were selected based on results of a recent study17 showing that for subcutaneous tissue 0.5 cm from the wound edge, a pressure of -10 mm Hg results in 15% of the maximal blood flow change, -45 mm Hg results in 64% change, -80 mm Hg results in 97% of maximal blood flow change, and -125 mm Hg is well above the threshold for maximal blood flow effects. Five cycles of intermittent and variable NPWT at each pressure range were applied; each cycle comprised 5 minutes of high pressure followed by 2 minutes of low pressure.
Microvascular blood flow was measured before application of negative pressure (baseline) and then after every change in negative pressure level. Excessive blood flow responses were not included in the results. Calculations and statistics. Eight experiments were performed. The output from the laser Doppler probes was continuously registered using PeriSoft software (Perimed, Stockholm, Sweden). Microvascular blood flow results were obtained as perfusion units (PU) and the percent change during negative pressure, compared to baseline values, was calculated. 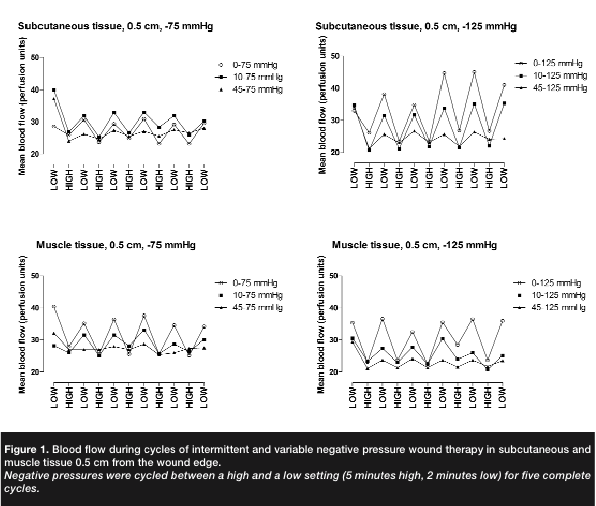 Calculations and statistics were performed using GraphPad 5.0 software (San Diego, CA). Statistical analysis was performed using the Mann-Whitney test when comparing two groups and the Kruskal-Wallis test with Dunn’s post test for multiple comparisons when comparing three groups or more. Significance was defined as P <0.05. Values are presented as means ± the standard error of the mean (SEM).
Calculations and statistics were performed using GraphPad 5.0 software (San Diego, CA). Statistical analysis was performed using the Mann-Whitney test when comparing two groups and the Kruskal-Wallis test with Dunn’s post test for multiple comparisons when comparing three groups or more. Significance was defined as P <0.05. Values are presented as means ± the standard error of the mean (SEM).
Results
Average baseline blood flow for the eight pigs was 40 ± 7 PU in muscle tissue and 28 ± 7 PU in subcutaneous tissue. At 0.5 cm from the wound edge, blood flow decreased in muscle and in subcutaneous tissue (-29% ± 2% and -22% ± 4%, respectively) when negative pressure -75 mm Hg was applied. (see Figure 1). The subcutaneous tissue and muscle tissue recordings 2.5 cm from the wound edge were grouped (soft tissue). In soft tissue further from the wound edge (2.5 cm), blood flow increased following application of negative pressure (20% ± 6% for -75 mm Hg, 24 ± 19% for -125 mm Hg) (see Figure 2). Blood flow returned to baseline values when negative pressure was discontinued.
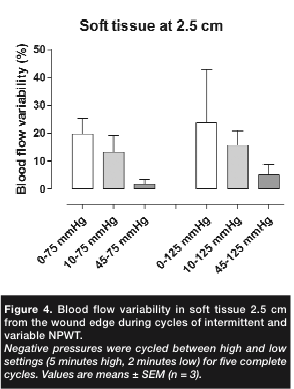
Blood flow changed repeatedly when the pressure was cycled between high and low subatmospheric pressure (variable NPWT) or between a subatmospheric pressure and 0 mm Hg (intermittent NPWT).When the difference in negative pressure settings was small (eg, when varying between -45 and -75 mm Hg), the increase and decrease in blood flow also was small (5% ± 2%) in subcutaneous tissue at 0.5 cm from the wound edge (see Figure 3). The alterations in blood flow seemed to be greater when the difference in negative pressure settings was larger (22% ± 4% for 0 and -75 mm Hg in subcutaneous tissue 0.5 cm from the wound edge; see Figure 2). Blood flow changes were similar when examined in soft tissue at 2.5 cm from the wound edge (see Figure 4).
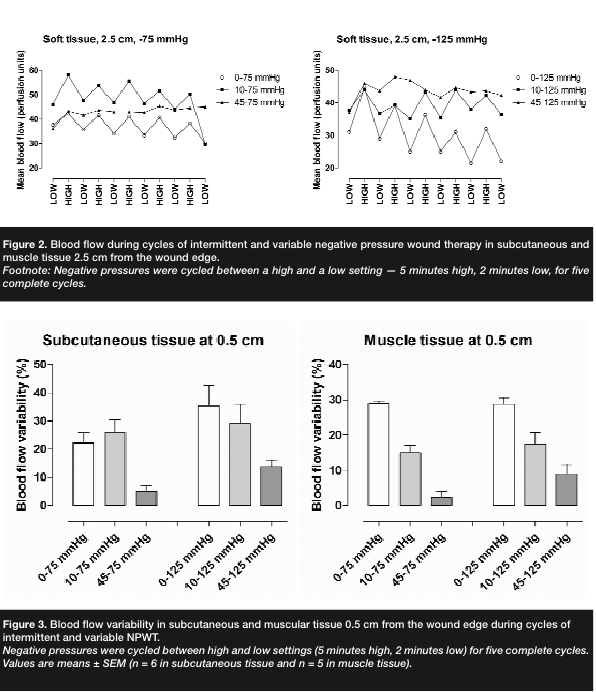 Variable NPWT at a lower pressure setting of -10 mm Hg resulted in blood flow effects similar to intermittent NPWT (26% ± 4% change when using -10 and -75 mm Hg and 22% ± 4% when using 0 and -75 mm Hg in subcutaneous tissue 0.5 cm from the wound edge, P >0.05; see Figure 3). Furthermore, there seemed to be no difference in blood flow alternations between intermittent or variable NPWT with a high pressure setting of -75 or -125 mm Hg (26% ± 4% when using -10 and -75 mm Hg and 29% ± 7% when using -10 and -125 mm Hg, in subcutaneous tissue, 0.5 cm from the wound edge; see Figure 2).
Variable NPWT at a lower pressure setting of -10 mm Hg resulted in blood flow effects similar to intermittent NPWT (26% ± 4% change when using -10 and -75 mm Hg and 22% ± 4% when using 0 and -75 mm Hg in subcutaneous tissue 0.5 cm from the wound edge, P >0.05; see Figure 3). Furthermore, there seemed to be no difference in blood flow alternations between intermittent or variable NPWT with a high pressure setting of -75 or -125 mm Hg (26% ± 4% when using -10 and -75 mm Hg and 29% ± 7% when using -10 and -125 mm Hg, in subcutaneous tissue, 0.5 cm from the wound edge; see Figure 2).
Discussion
The present study is the first to delineate microvascular blood flow changes near the wound edge during intermittent and variable NPWT. When negative pressure is applied, blood flow decreases 0.5 cm from the wound edge and increases 2.5 cm from the wound edge, which is in line with previous studies on pigs and humans.12,18,19 When negative pressure is applied in the intermittent mode (ie, cycling the therapy between atmospheric and subatmospheric pressure) or in the variable mode (ie, cycling the therapy between two different subatmospheric pressures), blood flow changes accordingly. In this study, changes in wound edge microvascular blood flow were largest when the difference in cycling pressures is large — ie, when using a high and a low negative pressure (eg, -75 and -10 mm Hg). When the difference in pressure level is not so large (eg, -75 and -45 mm Hg), the change in blood flow is less pronounced.
 Selecting suitable levels of negative pressure. The pressure levels for intermittent and variable NPWT used in the present study were selected after a series of experiments aimed to elucidate the relationship between the negative pressure level and blood flow response.17 Negative pressure close to zero — ie, -10 mm Hg — is known to have only minimal effect on blood flow. The next pressure level used, -45 mm Hg, results in approximately half of maximal blood flow effect. Maximum blood flow effects are seen at higher negative pressures. Although the clinical golden standard is -125 mm Hg, -75 mm Hg has been shown to offer approximately the same blood flow effects and a lower incidence of pain.17
Selecting suitable levels of negative pressure. The pressure levels for intermittent and variable NPWT used in the present study were selected after a series of experiments aimed to elucidate the relationship between the negative pressure level and blood flow response.17 Negative pressure close to zero — ie, -10 mm Hg — is known to have only minimal effect on blood flow. The next pressure level used, -45 mm Hg, results in approximately half of maximal blood flow effect. Maximum blood flow effects are seen at higher negative pressures. Although the clinical golden standard is -125 mm Hg, -75 mm Hg has been shown to offer approximately the same blood flow effects and a lower incidence of pain.17
In this study, no difference in blood flow alternations was found between intermittent and variable NPWT at -75 or -125 mm Hg. This may be explained by blood flow effect peaking at -75 mm Hg; thus, further elevations of the negative pressure do not cause additional blood flow effects.17 Also, no apparent difference in blood flow stimulating effects was found when variable NPWT is applied at a lower setting of -10 mm Hg compared to intermittent NPWT at 0 mm Hg. This might be explained by the fact that -10 mm Hg only has minimal blood flow effects. Changes in blood flow during NPWT. NPWT causes a decrease in the wound edge microvascular blood flow 0.5 cm from the wound edge. Conversely, microvascular blood flow 2.5 cm from the wound edge increased. These in vivo findings are in line with previously published studies.12,18,19
The mechanism by which NPWT affects blood flow in the wound edge is only partly known. Recently, tissue pressure 1 cm from the wound edge was shown to increase upon application of negative pressure; compression may hinder blood flow.20 The mechanism by which blood flow is increased farther from the wound edge by NPWT is more difficult to elucidate; one possible explanation may be that one of the mechanical effects of NPWT is wound contraction.21 NPWT will create a pulling effect on the tissue that may open vascular beds and cause increased blood flow. Previous experimental studies7,22 have shown that small arterioles and capillaries in the wound edge tissue open when negative pressure is applied. Favorable effects of intermittent and variable NPWT. The results of this study show that varying the level of negative pressure during NPWT using variable and intermittent therapy alters blood flow. Close to the wound edge, blood flow decreases at higher NPWT pressure settings and returns to baseline when NPWT is switched to a lower pressure setting (eg, 0 or -10 mm Hg). Farther from the wound edge, the opposite occurs — blood flow increases when a higher negative pressure is applied and returns to baseline values at the lower pressure setting (0 or -10 mm Hg). Variable or intermittent NPWT may both result in a beneficial combination of blood flow effects. Decreased blood flow is known to stimulate angiogenesis and granulation tissue formation.23 Increased blood flow may be important to ensure adequate oxygenation and nutrient supply and removal of waste products from the healing wound, as well as to facilitate penetration of antibiotics to otherwise poorly perfused tissue. Morykwas et al2 showed that intermittent NPWT resulted in a 103% increase in new granulation tissue formation compared to a more modest 63% increase during continuous NPWT. Thus, it seems that the intermittent mode should be used in order to maximize granulation tissue formation. These findings and the results of the current study appear in concordance with Holle et al,11 who found 100% tissue survival of seven random-pattern flaps with critical tip perfusion following intermittent NPWT. Thus, cycling the level of negative pressure during NPWT accelerates granulation tissue formation.
Clinical perspective. Intermittent or variable NPWT may be particularly advantageous when treating wounds at risk for development of ischemia — ie, where the wound edge tissue is poorly vascularized, such as in superficial flaps. NPWT exerts pressure against the wound edge, which results in hypoperfusion.12,18-20 It is well known that the level of pressure sometimes needs to be reduced during treatment with continuous NPWT to prevent development of ischemia. During intermittent and variable NPWT, pressure is alleviated repeatedly, which may prevent persistent tissue ischemia. For the same reasons, the need for a reduction of the level of negative pressure may be omitted in variable NPWT.
Another advantage to using intermittent and variable negative pressure is that the wound edge is contracted repeatedly, resulting in mechanical stimulation, which has been shown to promote the expression of growth factors (eg, vascular endothelial growth factor and fibroblast growth factor-2) and stimulate granulation tissue formation and angiogenesis.24-26 Venturi et al27 suggested that intermittent negative pressure is more effective than continuous negative pressure in stimulating wound healing because intermittent pressure causes greater cell deformation.
Concerns. Pressure cycling may be limited by patient tolerance.28,29 Intermittent NPWT causes a continuous mechanical tissue deformation, a source of discomfort.14 Pain might be reduced by diminishing the gradient between the cycled negative pressures. Preferably, this could be done without completely decreasing the negative pressure to 0 mm Hg, but rather reducing the pressure to, for example, -10 mm Hg per variable NPWT. Another issue when cycling negative pressure to atmospheric pressure during intermittent therapy may be that the adhesive drape detaches from the skin. This problem may be addressed by cycling to a low subatmospheric pressure (variable NPWT); thereby, negative pressure will not be lost and the suction force will hold the dressing in place. Based on what is known at this time, intermittent or variable NPWT may not be suitable for all wound types. For example, wounds that require stabilization, such as sternotomy wounds, may best be treated with continuous NPWT.23,28
Study Limitations
One limitation is that subcutaneous and muscle data from 2.5 cm from the wound edge were combined. However, because the aim of the study was to examine and compare the effect of intermittent and variable pressure on blood flow in the wound edge and because microvascular blood flow varies with the pressure settings, conclusions were not affected by combining data.
Conclusion
The results of this in vivo study suggest that cycling the level of negative pressure during NPWT (intermittent or variable NPWT) is beneficial. Both intermittent and variable NPWT result in decreased blood flow that is known to stimulate angiogenesis and granulation tissue formation and to increase blood flow that is known to facilitate oxygenation and nutrient supply and removal of waste products. Alternations in wound edge microvascular blood flow are largest when the difference in cycling pressures is large (ie, when using high and low negative pressure settings of -75 and -10 mm Hg). The blood flow is similar when using intermittent or variable NPWT with a high pressure setting of -75 and -125 mm Hg. Also, there is no apparent difference in blood flow stimulating effects when a variable negative pressure, with a lower setting of -10 mm Hg, is compared with an intermittent negative pressure with a lower setting of 0 mm Hg. Cycling the negative pressure level may be beneficial especially when treating poorly vascularized tissue with a risk for development of ischemia, as pressure is released repeatedly. In cases where intermittent therapy causes discomfort, variable therapy may be viable alternative.
Acknowledgment
The authors thank Rola Ba-Abbad, Bodil Gesslein, and Gisela Håkansson, for contributing to the experimental work.
1. Argenta LC, Morykwas MJ. Vacuum-assisted closure: a new method for wound control and treatment: clinical experience. Ann Plast Surg. 1997;38(6):563–576; discussion 577.
2. Morykwas MJ, Argenta LC, Shelton-Brown EI, McGuirt W. Vacuum-assisted closure: a new method for wound control and treatment: animal studies and basic foundation. Ann Plast Surg. 1997;38(6):553–562.
3. Morykwas MJ, Simpson J, Punger K, et al. Vacuum-assisted closure: state of basic research and physiologic foundation. Plast Reconstr Surg. 2006;117(7 suppl):121S–126S.
4. Banwell PE. Topical negative pressure therapy in wound care. J Wound Care. 1999;8(2):79–84.
5. Lu X, Chen S, Li X, et al The experimental study of the effects of vacuum-assisted closure on edema and vessel permeability of the wound. Chinese J Clin Rehabil. 2003;7:1244–1245.
6. Gouttefangeas C, Eberle M, Ruck P, et al. Functional T lymphocytes infiltrate implanted polyvinyl alcohol foams during surgical wound closure therapy. Clin Exp Immunol. 2001;124(3):398–405.
7. Chen SZ, Li J, Li XY, Xu LS. Effects of vacuum-assisted closure on wound microcirculation: an experimental study. Asian J Surg. 2005;28(3):211–217.
8. Evans D, Land L. Topical negative pressure for treating chronic wounds: a systematic review. Br J Plast Surg. 2001;54(3):238–242.
9. Greene AK, Puder M, Roy R, et al. Microdeformational wound therapy: effects on angiogenesis and matrix metalloproteinases in chronic wounds of 3 debilitated patients. Ann Plast Surg. 2006;56:418–422.
10. Baldwin C, Potter M, Clayton E, et al. Topical negative pressure stimulates endothelial migration and proliferation: a suggested mechanism for improved integration of Integra. Ann Plast Surg. 2009;62(1):92–96.
11. Holle GPA, Fritschen VU, Exner K. Von der komplizierten Wunde zum Tissue-engineering. Besondere Indikationen für die V. A. C. Therapie. Jahrestagung Vereinigung der Deutschen Plastischer Chirurgen. 2002(Abstractband 33.):48.
12. Wackenfors A, Sjogren J, Gustafsson R, et al. Effects of vacuum-assisted closure therapy on inguinal wound edge microvascular blood flow. Wound Repair Regen. 2004;12(6):600–606.
13. Ramnarine IR, McLean A, Pollock JC. Vacuum-assisted closure in the paediatric patient with post-cardiotomy mediastinitis. Eur J Cardiothorac Surg. 2002;22(6):1029–1031.
14. Gupta S, Baharestani M, Baranoski S, et al. Guidelines for managing pressure ulcers with negative pressure wound therapy. Adv Skin Wound Care. 2004;17(2 suppl):1–16.
15. Lindstedt S, Malmsjö M, Gesslein B, Ingemansson R. Evaluation of continuous and intermittent myocardial topical negative pressure. J Cardiovasc Med (Hagerstown). 2008;9(8):813–819.
16. Zografos GC, Martis K, Morris DL. Laser Doppler flowmetry in evaluation of cutaneous wound blood flow using various suturing techniques. Ann Surg. 1992;215(3):266–268.
17. Borgquist O, Ingemansson R, Malmsjö M. Wound edge microvascular blood flow during negative pressure wound therapy: examining the effects of pressures from -10 to -175 mm Hg. Plast Reconstr Surg. 2010;125(2):502–509.
18. Wackenfors A, Gustafsson R, Sjogren J, et al. Blood flow responses in the peristernal thoracic wall during vacuum-assisted closure therapy. Ann Thorac Surg. 2005;79(5):1724–1730; discussion 1730–1731.
19. Kairinos N, Voogd AM, Botha PH, et al. Negative-pressure wound therapy II: negative-pressure wound therapy and increased perfusion. Just an illusion? Plast Reconstr Surg. 2009;123(2):601–612.
20. Kairinos N, Solomons M, Hudson DA. The paradox of negative pressure wound therapy — in vitro studies. J Plast Reconstr Aesthet Surg. 2010;63(1):174–179.
21. Malmsjö M, Ingemansson R, Martin R, Huddlestone E. Negative-pressure wound therapy using gauze or open-cell polyurethane foam: similar early effects on pressure transduction and tissue contraction in an experimental porcine wound model. Wound Repair Regen. 2009;17(2):200–205.
22. Ichioka S, Watanabe H, Sekiya N, et al. A technique to visualize wound bed microcirculation and the acute effect of negative pressure. Wound Repair Regen. 2008;16(3):460–465.
23. Malmsjö M, Ingemansson R, Sjogren J. Mechanisms governing the effects of vacuum-assisted closure in cardiac surgery. Plast Reconstr Surg. 2007;120(5):1266–1275.
24. Quinn TP, Schlueter M, Soifer SJ, Gutierrez JA. Cyclic mechanical stretch induces VEGF and FGF-2 expression in pulmonary vascular smooth muscle cells. Am J Physiol Lung Cell Mol Physiol. 2002;282(5):L897–L903.
25. Rivilis I, Milkiewicz M, Boyd P, et al. Differential involvement of MMP-2 and VEGF during muscle stretch- versus shear stress-induced angiogenesis. Am J Physiol Heart Circ Physiol. 2002;283(4):H1430–H1438.
26. Urschel JD, Scott PG, Williams HT. The effect of mechanical stress on soft and hard tissue repair; a review. Br J Plast Surg. 1988;41(2):182–186.
27. Venturi ML, Attinger CE, Mesbahi AN, et al. Mechanisms and clinical applications of the vacuum-assisted closure (VAC) device: a review. Am J Clin Dermatol. 2005;6(3):185–194.
28. Bovill E, Banwell PE, Teot L, et al. Topical negative pressure wound therapy: a review of its role and guidelines for its use in the management of acute wounds. Int Wound J. 2008;5(4):511–529.
29. Jones SM, Banwell PE, Shakespeare PG. Advances in wound healing: topical negative pressure therapy. Postgrad Med J. 2005;81(956):353–357.




